Different Potential Vaccine Candidates of Covid-19 Diseases and their Immunological Aspect
On December 31, 2019, a novel coronavirus outbreak caused cough, fever, and dyspnea with ARDS in residents of Wuhan, Hubei Province, China. Later, it spread throughout the world, affecting not only livelihood but also the economy and social fabric. Scientists from different continents were involved in the discovery of its vaccine, and many vaccines were produced. As a result, the goal of this work is to examine the various potential vaccines for SARS-COV-2 virus and COVID-19 associated disease, as well as their immunological aspects. a new coronavirus that was later dubbed severe acute respiratory syndrome coronavirus-2. By its nature, this virus is a positive-sense single-stranded RNA virus that contains a spiral or circular genome inside of its crown-like structure. Spike proteins, which are structural proteins found in viruses, play an important role in virus entry into the host cell. Following entry, the virus replicated in the cell, causing the immune system to become overly responsive, potentially leading to organ and system failure. Although the first coronavirus outbreak occurred two decades ago, no effective vaccine was developed. However, following the virus’s outbreak, a large number of scientists, clinicians, and researchers were mobilized to develop vaccines in an unprecedented time frame. Owing to their urgent need, some vaccines are licensed with minor side effects. Therefore, vaccine safety and efficacy should be assured prior to approval for emergency use. Since vaccine development and sustainability have faced virus mutation, regular virus genome sequencing and analysis should be recommended to combat the upcoming viral infection.
Introduction
At the end of December 2019, a novel coronavirus was recognized as the reason for the presentation of patients with cough, fever, and dyspnea with acute respiratory distress syndrome (ARDS) of unknown etiology in Wuhan city, from Huanan Seafood Wholesale Market, in the Hubei Province of China [1], the etiological agent of pneumonia was officially announced as a novel coronavirus [2, 3] and abbreviated as 2019-nCoV by the WHO [4]. This pathogen was later renamed as severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) by the International Committee of Taxonomy of Viruses (ICTV), and the disease was named coronavirus disease 2019 (COVID-19) by the WHO [5]. The Chinese Center for Disease Control and Prevention quickly identified the pathogen as a new type of coronavirus and deposited the first viral sequence into GenBank (LR757995, LR757998) on January 30, 2021 [6].
The virus belongs to the Nidovirales order, which consists of three families, namely, Roniviridae, Arteriviridae, and Coronaviridae [7, 8]. At the same time, the Coronaviridae family is divided into two groups, which include the Torovirinae and the Coronavirinae. Further, the Coronavirinae subfamily is classified into alpha-, beta-, gamma-, and delta-COVs [7]. Coronaviruses are large, enveloped, single-stranded RNA viruses found in humans and other mammals, such as dogs, cats, chickens, cattle, pigs, and birds. Coronaviruses cause respiratory, gastrointestinal, and neurological diseases. The coronavirus is a zoonotic virus that causes respiratory infections. It was identified as a coronavirus in 1965 due to its crown-like appearance under microscopy [9].
The types of coronavirus known to date are SARS-CoV, which causes severe acute respiratory syndrome (SARS) that originated in China between 2002 and 2004; MERS-CoV, which causes Middle East respiratory syndrome (MERS) that originated in the Arabian Peninsula in 2012; and SARS-CoV-2, which causes the disease known as coronavirus disease 2019 (COVID-19). It has a diameter of 60 nm to 140 nm and distinctive spikes that give the virions the appearance of a solar corona [10]. Through genetic recombination and variation, coronaviruses can adapt to and infect new hosts. Bats are thought to be a natural reservoir for SARS-CoV-2, but it has been suggested that humans became infected with SARS-CoV-2 via an intermediate host, such as the pangolin [11, 12].
The clinical manifestations of COVID-19 can vary from asymptomatic and mild flu-like symptoms to ARDS and death. Long-term pulmonary, cardiological, and neurological complications have also been reported in COVID-19 cases [13]. Compared with SARSCoV and MERS-CoV, SARS-CoV-2 is highly contagious [14]. It was realized that vaccines could play an essential role in increasing the immunity of the population, preventing severe conditions caused by COVID-19 infection, reducing the burden on healthcare systems, and minimizing economic losses [15]. Traditionally, vaccines require 10–15 years of research, development, and testing before their clinical use can begin [16]. However, in early 2020, scientists embarked on attempts to produce safe and effective SARS-CoV-2 vaccines at record speed [17].
More than 250 vaccine projects were initiated worldwide in 2020, and according to a recent WHO report, 97 vaccines are in clinical trials from phases 1 to 3, and 182 are in their preclinical development stages. Different technologies have been applied in vaccine preparation, some conventional and some newly developed and applied for the first time in humans [18, 19]. The vaccines can initiate an adaptive immune response, particularly B- and T-cell responses, by introducing antigens. Although there are a lot of vaccine candidates in different phases of clinical trials, only a few have been approved for use. The safety, efficacy, and immunogenicity of these vaccines vary. Some licensed vaccines require optimal storage temperatures, while others require ultra-cold storage temperatures, posing a problem for vaccine usage in Poor Countries. In terms of safety, some vaccines have minor side effects, while the safety of others is unknown. Serious public health crisis, and high mortality of COVID-19, an effective, safe, and stable vaccine is urgently needed to control this pandemic. Therefore, the aims of the current work are:
- To review severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2).
- To update the recent development of the COVID-19 vaccine and its immunogenicity.
- To overview the progress of universal COVID 19 vaccine development.
Literature Review
Virology
SARS-CoV-2 is an enveloped, positive-sense single- stranded RNA (ssRNA) virus that can be categorized in the family Coronaviridae and order Nidovirales. The family consists of two subfamilies, Coronavirinae and Torovirinae, and members of the subfamily Coronavirinae are subdivided into four genera: (a) Alpha coronavirus contains the human coronaviruses HCoV-229E and HCoV-NL63; (b) Beta coronavirus includes HCoV-OC43, Severe Acute Respiratory Syndrome human coronavirus (SARS-HCoV), HCoV-HKU1, and Middle Eastern respiratory syndrome coronavirus (MERS-CoV); (c) Gamma coronavirus includes viruses of whales and birds; (d) Delta coronavirus includes viruses isolated from pigs and birds [20] SARS-CoV-2 is a member of the beta-coronavirus family, which also includes two other highly pathogenic viruses, SARS-CoV and MERS-CoV [21].
Genomic Features of SARS-Cov-2
Coronaviruses form enveloping, spherical particles, and they have a cloverleaf structure. Glycoproteins and proteins on the virus’s surface have created a crown-like structure on it. These viruses are called coronaviruses because of their crown structure. A nucleo-capsid is made of capsid-coated proteins that contain the virus’s genetic material Figure 1 [22]. The genome of SARS-CoV-2 is around 30 kb and starts with a 5’ cap structure and ends with a 3’ poly-A tail [23].
The virus genome consists of two terminal untranslated regions (5’ and 3’ UTRs) and twelve putative functional open reading frames (ORFs). The 5′-terminus of the CoV genome contains two overlapping ORFs, ORF 1a and ORF 1b, that span over two-thirds of the genome and encode the large replicase polyproteins (pp1a and pp1ab), which are post-translationally cleaved into 16 putative non-structural proteins (nsps) involving proteases, RNA polymerase, helicase, and other proteins involved in the transcription of the viral genome, replication of SARS-CoV, and subgenomic mRNA synthesis [24, 25, 26]. The SARS-CoV-2 virus is composed of four structural proteins, including S protein, envelope (E), membrane (M), and nucleocapsid (N), which are encoded by the 3′-terminus of the CoV genome [23, 27].
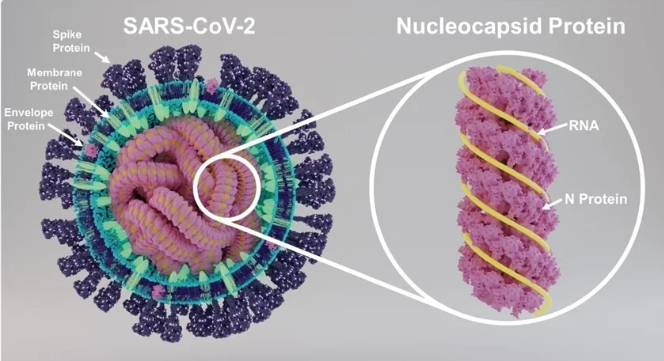
S-protein is responsible for the initial attachment of the virus to the host cell surface. It has two subunits, S1 (specific receptor binding domain known as RBD) and S2 (CoV S2 glycoprotein). S protein, through its specific RBD, binds to its receptor on the host cell [28]. M protein has three transmembrane domains and plays a vital role in introducing the virus into the body and forming envelopes, whereas E protein is responsible for proliferation, germination, envelope formation, assembly, and release of viral particles from the cell. It is also involved in viral pathogenesis [29]. N protein has two domains, both of which can attach to the viral RNA in order to assist replication, and it also acts as a repressor of the RNAi system of the host cell, hence supporting viral replication [30].
Potential Sars/Cov-2 Vaccine Candidate
A vaccine is a biological product that produces an acquired active immunity against a specific microbial disease [31]. Vaccines are very vital and save the lives of millions of people every year. The primary function of vaccines is to train and prepare the immune system to identify and fight the target pathogen. Vaccines have common components like active ingredients of pathogen antigens that directly stimulate the immune system, adjuvants, antibiotics, stabilizers (sugar or gelatin), preservatives, and trace components. The research and development of COVID-19 vaccines is going very quickly, and the entire vaccine development process, including the required clinical trials, has been amazingly shortened to 15–18 months instead of 10–15 years. As a result, the simultaneous marketing of multiple vaccines began in early 2021 [32, 33].
Universal COVID-19 Vaccine and SARS-COV-2 Variants
The SARS-CoV-2 which causes COVID-19 cases in Wuhan, China is designated as the “Wuhan reference strain”, while the SARS-CoV-2 strains with mutations are referred to as variants [34]. Currently, due to the nature of virus and mutation problems, several SARS-CoV-2 variants have been emerged. Commonly known that has emerged variants are mink Cluster 5, lineage B.1.525, lineage P.3, the UK variants (B.1.1.7, variant of concern [VOC] 202012/01, and VOC 202102/02), Indian variant (B.1.617), Nigerian variant (B.1.1.207), South African variant (B.1.351), California variants (B.1.429 and B.1.427), Brazil variants (lineages P.1 and P.2), and le variant Breton. The transmissibility and lethality of the variants are higher than those of the Wuhan reference strain. Therefore, a universal vaccine for the reference strain and all variants (present and future) is indispensable [35].
Most of currently available vaccines are based on spike protein. The Pfizer/BioNTech and Oxford-AstraZeneca vaccines provided protection against the UK variant of concern (B.1.1.7) [36]. However, whether the currently available spike (S) protein-based COVID-19 vaccines from Pfizer/BioNTech, Moderna, Oxford-AstraZeneca, and Johnson & Johnson have a protective effect against the Indian variant (B.1.617) is still uncertain. Even if these vaccines are effective against B.1.617, there might be still new emergence of SARS-CoV-2 variants, thus a universal vaccine for all variants of SARS-CoV-2 is urgently needed. If the current S protein-based vaccines are found to be ineffective against any of the variants, a universal COVID-19 vaccine would indeed be indispensable [37].
Universal COVID-19 Vaccine Targeting SARS- Cov-2 Envelope Protein
Understanding of the origin, genomic features, and pathogenic mechanisms of SARS-CoV-2 is very subjective to design appropriate corresponding strategies for the development of universal COVID-19 vaccine. The SARS-CoV-2 virus is composed of four structural proteins, including S protein, envelope (E), membrane (M), and nucleocapsid (N), which are encoded by the 3′-terminus of the CoV genome [23, 38]. The coronavirus E protein is a small integral 75 amino acid membrane protein involved in crucial aspects of the viral lifecycle, including assembly, budding, envelope formation, replication and pathogenesis [29]. This protein is thus a potential target for the development of a universal COVID-19 vaccine, because of its highly conserved amino acid sequence. The variant mutations occur mainly in the spike protein, and conservation of E protein remained stable in most Variants of Concern. Therefore, a vaccine targeting the SARS-CoV-2 E protein would be effective against the SARS-CoV-2 Wuhan reference strain and all current and future SARS-CoV-2 variants. These facts suggest a strategy for developing a universal vaccine against SARS-CoV-2 that would be effective against all variants, current and future: a vaccine based on the E protein [37].
Diversity of COVID-19 Vaccine Technology Platforms
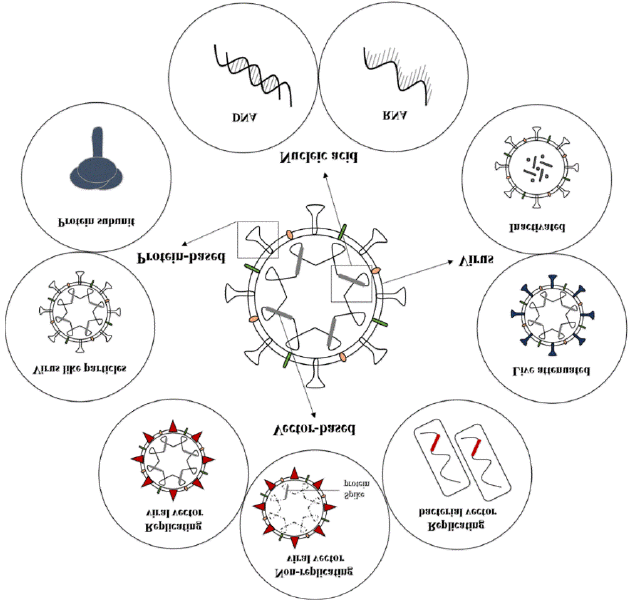
Notably, the technology platforms used on COVID-19 vaccines were abundant, and each of the platforms has some advantages and disadvantages, as listed in Table 1. The most common technology platforms, in descending order of frequency, were protein subunit (PS), RNA, viral vector non- replicating (VVNR), inactivated virus (IV), DNA, virus-like particle (VLP), viral vector replicating (VVR), VVR combined with antigen-presenting cells (APC), live attenuated virus (LAV), dendritic cell vaccine (DCV), and T cell-based vaccine (TCV) [6]. Among all vaccine types being evaluated in trials, types such as nucleic acid, viral vectors, viruses, and protein subunits Figure 3 are more frequently used [39].
In terms of vaccine research and development, vaccine types such as TCV, LAV, DCV, and VVR+APC were still in their early stages, with only a few products designed for each type; no product has been confirmed to have adequate safety to date. Despite the fact that no efficacy has been confirmed as of yet, VVR, VLP, and DNA have more products planned, and some of the involved products have already entered the efficacy confirmatory phase. It is gratifying that there were two RNA vaccines, two PS vaccines, four VVNR vaccines, and seven IV vaccines authorized for emergency use (Table 2) [6].
Formaldehyde inactivation, UV and gamma irradiation, or growing SARS-CoV-2 in cell culture, usually on Vero cells 9 (monkey kidney cells) and growing in bioreactor tanks, followed by chemical inactivation of the virus [40, 41], are all methods for producing inactivated vaccines. Dousing with a chemical called beta-propiolactone could disable the viruses by binding to their genes and thus preventing their replication; however, their proteins, including the spike (S) protein, remained intact [42]. The productivity of the virus in cell culture and the requirement for production facilities at biosafety level 3 are the common bottlenecks for vaccine production. These vaccines are usually administered intramuscularly and can contain alum or other adjuvants to boost the immune response against the inactivated vaccine [43].
Four inactivated vaccines have been given authorization for use. Inactivated vaccines contain a diverse set of native viral antigens [44]. Such multiple antigens can induce a TH2 response and lung eosinophilia, which may be worse in aged hosts [45]. This broad-spectrum immune stimulation may result in a special condition in the post-vaccination period called the vaccine-related enhancement of disease (VRED) [46]. Therefore, TH1-skewing modified alum or other types of adjuvants such as CpG are recommended to be added to the vaccine as alternatives to avoid VRED [47].
| Vaccine platforms | Advantage | Disadvantage |
|---|---|---|
| Inactivated Virus | Stable and safe | Require multiple boosters |
| Can be used together with adjuvant to increase the immunogenicity | Low titre production | |
| Immunocompromised individuals can also be vaccinated | ||
| RNA-based | Low cost and rapid manufacturing | Show instability and thus low |
| Good safety profile | immunogenicity | |
| No risk of viral genome integration into host genome | May be requiring multiple doses | |
| Viral Vector | Highly specific for gene delivery in target cells | Immunity against vector may reduce the efficacy |
| May induce robust immune response | Probability of integration of viral genome into the host genome that may lead to tumorigenesis | |
| Increases cellular immunity | Induces low titre production | |
| Protein Subunit | Good safety profile | Low immunogenicity |
| Immunocompromised individuals can also be immunised | ||
| DNA-based | Stable | Low titre production |
| Low cost manufacturing | May get integrated into host Genome | |
| Good safety profile | ||
| Infectious viral particles are not involved | ||
| Virus-like particles | Can be used with adjuvant to increase the immunogenicity | May require multiple boosters |
| Low titre production | ||
| Live-attenuated Virus | High potency with low cost manufacturing | Viral nucleotide substitution may occur leading to production of recombinant strain |
| Intrinsic ability to stimulate innate immune response | Not suitable for Immunocompromised individuals. |
Table 1: Advantage and Disadvantage of various vaccine platforms used for development of vaccine candidates against viral infecti
| Vaccine | Sponsor | Type | Storage | Dosage | Efficacy |
|---|---|---|---|---|---|
| Gam-COVID-Vac Lyo | Gamaleya Research Institute | VVNR | stable at 2–8°C | 2 doses, 0/21days | 92% |
| BBIBP-CorV* | Sinopharm | IV | stable at 2–8°C | 2 doses, 0/21days | 78.10% |
| EpiVacCorona | Federal Budgetary Research Institution | PS | Unclarified | 2 doses, 0/21- 28day | / |
| BNT162b2 | Pfizer/BioNtech/ Fosun Pharma | RNA | Stable at −80 ~ −60°C; 2 ~ 8°C for 1 month | 2 doses, 0/21 | 95% |
| mRNA-1273 | Moderna/NIAID | RNA for 24 hours | Stable at −50 ~ −15°C; 2 ~ 8°C for 30 d; 8 ~ 25°C | 2 doses, 0/28day | 94% |
| AZD-1222 | Oxford Universty/ AstraZen eca | VVNR | stable at 2–8°C | 2 doses, 0/4-12 w | 70% |
| COVAXIN | Bharat Biotech | IV | stable at 2–8°C | 2 doses, 0/28d | 81% |
| CoronaVac* | Sinovac | IV | stable at 2–8°C | 2 doses, 0/14d | / |
| QAZCOVID-IN | Unclarified | IV | Unclarified | Unclarified | / |
| CoviVac | Russian Academy of Sci ences | IV | Unclarified | Unclarified | 51% |
| Unclarified* | Sinopharm | IV | stable at 2–8°C | 2 doses, 0/21d | 72.80% |
| Ad5-nCoV* | CanSino-BIO | VVNR | stable at 2–8°C | 1 dose | / |
| Ad26.COV2.S | Janssen | VVNR | Stable at −20°C; 2 ~ 8°C for 3 months | 1 dose | / |
| ZF2001 | Zhifei/Chinese Academy of Sciences | PS | stable at 2–8°C | 3 doses, 0/30/60d | / |
| KCONVAC | Beijing Minhai Biotechnol ogy Co | IV | Unclarified | 2 doses, 0/28d | / |
Table 2: Overview of authorized COVID-19 vaccines worldwide [49].
Viral vector non-replicating (VVNR); Inactivated virus (IV); Protein subunit (PS) Table 2: Overview of authorized COVID-19 vaccines worldwide [49].
Covaxin Vaccine (Cov; Bharat Biotech Vaccine, Bbv152)
It was manufactured by a collaboration of the Indian Bharat Biotechnology Company, the Indian Council of Medical Research, and the National Institute of Virology [44]. The COV has been granted permission in India for restricted use in emergency situations despite being in phase 3 of clinical trials [50, 51]. This vaccine is used in a two-dose regimen with the doses given 4 weeks apart, and its efficacy is reported to be 81% [52], although 82.8 to 91.9% of the vaccinated people generated antibodies (seroconverted) with robust immune responses [52]. It can be stored for one week at room temperature, which makes it suitable for usage in tropical and subtropical countries [50].
Sinopharm Vaccine (SV; BBIBP-Corv)
The Sinopharm vaccine is manufactured by a Chinese company, Sinopharm Group, and is marketed with the cooperation of the UAE. This vaccine used a HB02 strain rather than a WIV04 strain [53]. It is administered in a two-dose regimen, with the doses given 3 weeks apart by intramuscular injection. It showed an efficacy of 79.34% in China and 86% in the UAE, besides being 100% effective in preventing moderate and severe COVID-19 cases. The developers did not report any serious side effects during its phase III clinical trial or after its authorization for use [47].
Sinopharm-Wuhan Vaccine (SWV)
The Sinopharm-Wuhan vaccine was prepared by the Chinese Wuhan Institute of Biological Products. It is effective in preventing COVID-19 in 72.5% of vaccinees (https://www.reuters.com/article/us-health-coronavirus- vaccine-sinopharm). It shows comparable side effects to the Sinopharm vaccine and is also in its Phase III clinical trial [54]. The Wuhan vaccine utilizes the WIV-04 strain, which was isolated and cultivated in a Vero cell line for propagation. Then, the supernatant of the infected cells was inactivated.
This vaccine is given in two doses, three to four weeks apart. A third dose is recommended for those individuals who show weak immune responses [54].
Mrna Vaccines
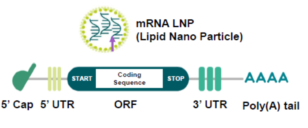
mRNA vaccines are characterized by robust immunogenicity, intrinsic adjuvant properties, low production costs, favorable safety profiles, quick production, and special storage and delivery systems. This vaccine preparation has been investigated over the last 20 years for different viruses, such as rabies, influenza, and Zika [56]. The main advantage of this technology is that it allows the body’s cells to produce S proteins rather than injecting them as in vaccines. This reduces the time required for building the vaccine and hence requires less time compared to that required for classical vaccines [57]. The conventional mRNA vaccines utilize manufactured nucleoside-modified, single- stranded messenger RNA (Figure 4) to deliver genetic instructions to human cells for building up the coronavirus protein known as the spike protein (S) [58].
Some intrinsic features of mRNA molecules demand special strategies to guarantee the stability, efficacy, and safety of mRNA vaccines. First, mRNA is intrinsically unstable and prone to degradation due to the omnipresence of RNases in the serum and plasma [60]. Second, the cellular machinery recognizes exogenous RNA molecules as an immunological mimic of viral infection, which results in an immediate immune response [61]. Thus, it is a prerequisite for the design of mRNA vaccines to maximize the stability of mRNA and translation efficiency and avoid the innate immune response by host cells [62, 63].
The design achieved by 5’-capping the mRNA vaccine, which is critical for protecting mRNA from exonuclease activity, facilitating pre-mRNA splicing, and serving as the binding site for eIF4F, the heterodimeric translation initiation complex) [64, 65], Optimization of the 5’ and 3’ UTRs and the length of the polyadenylation tail are closely associated with translation efficiency [66]. modification of the nucleosides in mRNA molecules by incorporating pseudouridine into mRNA molecules in the place of uridine, in order to suppress the activation of TLR and avoid the degradation of RNA by RNase L [67, 68].
The mRNA enters the human cells encapsulated by lipid nanoparticles (LNP) that prevent the cells of the body from degrading it and give stability to the mRNA, which is a fragile molecule. After mRNA has passed its instructions to the protein-making machinery in the cytoplasm of the body’s cells, enzymes called ribonucleases (RNases) degrade the mRNA [58]. Therefore, it is impossible for the mRNA to integrate with the DNA in the nucleus of the vaccinated cells, posing no risk of inducing genetic changes. After the S protein is produced by the cells of the body, the immune response is initiated with its two arms, i.e., humoral and T-cell-mediated immunity. The neutralizing antibodies can stop the spike in protein. The killer T cells (CD8+) in vaccinated individuals recognize and destroy any coronavirus-infected cells that display spike protein fragments on their surfaces [69].
Moderna Vaccine (MV)
mRNA-1273 was developed by Moderna and consists of mRNA encoding the spike protein stabilized in the prefusion conformation, or SARS-CoV-2 S(2P), formulated in lipid nanoparticles (Corbett et al., 2020a) [70]. This vaccine has an advantage over the Pfizer vaccine in that it can be stored at temperatures equivalent to a standard freezer (-20 oC), making it easier to ship to remote and rural areas, and it has an efficacy of 94.1%. It requires two shots four weeks apart [71]. When mRNA-1273 was tested in nonhuman primates, the vaccine-induced neutralizing antibodies reached levels higher than human convalescent-phase serum (Figure 5). There was a dose-dependent increase in Th1-biased responses, with low or undetectable Th2 or CD8 T-cell responses 4 weeks after the second dose. Vaccinated animals did not have evidence of viral replication or virus RNA identified in broncho-alveolar lavage fluid or nasal samples. There was also limited lung inflammation on day 2 post-exposures to the SARS-CoV-2 virus in the vaccinated group [72].
![Figure 4: Structure of Conventional mRNA Vaccine [59].](/fulltextimages/10650/fig_4.png)
Pfizer–Biontech Vaccine (PBV)
After the onset of the pandemic, Pfizer and German BioNTech collaborated and compared four mRNA-based vaccines to select a potential candidate against SARS-CoV-2 infections. Based on the trial results, vaccine candidate options were narrowed down to two: BNT162b1, encoding a receptor-binding domain, trimerized by adding a T4 fibritin foldon domain, and BNT162b2, encoding a full-length S protein modified by two proline mutations [73]. The PBV is given in two doses, 3 weeks apart [74]. It is also recommended that vaccinated individuals receive a booster shot, or a third dose, within 12 months of being fully vaccinated and then annually thereafter. The vaccine is 95% effective in providing protection [74].
PBV offers strong protection against COVID-19 within 10 to 14 days of the first dose, regardless of the recipient’s race, weight, or age [75]. It can produce strong antibody and T-cell immune responses. This vaccine does not cause any serious side effects but frequently causes short-lived symptoms such as pain at the site of injection, mild fever, fatigue, and muscle pain [76]. It is interesting to note that BTN162b vaccines are suggested to be shipped and stored at an ultra- cold temperature of -80 C, which imposes difficulties on their usage in certain countries [77].
CVNCOV Vaccine of Curevac (CVV)
It is produced by Tübingen’s CureVac biotech firm in partnership with the Bayer Company and is currently in its combined phase 2b/3 clinical trial. This vaccine is considered a rival to the leading mRNA vaccines, PBT and MV [69]. Like the PBT and MV, the CVV utilizes a natural, non- chemically modified, synthetic mRNA coding the prefusion- stabilized full-length spike protein of SARS-CoV-2. The CVV
is administered intramuscularly in a two-dose regimen with an interval of four weeks. This vaccine requires lower doses (12mg) than the 30 mg for PBV and the 100 mg for MV (https://www.curevac.com/en/covid-19/). The manufacturers claimed that it showed an efficacy of 95%. The vaccine remains stable for at least three months when it is stored at 5 oC, as suggested by its manufacturer. Moreover, it can be stored at room temperature as a ready-to-use vaccine for up to 24 hours, which makes it suitable for usage in poorer countries [69].
Non-Replicating and Replicating Viral Vector- Based Vaccines
These types of vaccines utilize replication-deficient or attenuated replication-competent (bioengineered) viral vectors [78, 79]. It can effectively introduce genes encoding viral antigens into host cells. The infected cells produce and release immunogenic antigens after a certain period of vaccination [25]. Many viral vector platforms that have been tested in SARS-CoV and MERS-CoV are being explored in COVID-19 vaccines, including adenovirus (both human and non-human primates), measles virus, modified vaccinia virus Ankara (MVA), parainfluenza virus, rabies virus, and vesicular stomatitis virus (VSV) [80]. The most common replication-incompetent viral vectors currently in use are human Ad5 and Ad26 adenoviruses and a modified version of the chimpanzee adenovirus ChAdOx1. This vector carries and delivers a double-stranded DNA segment of the RNA of SARS-CoV-2 that codes the S-protein antigen of the virus [69].
After injection, genetic material escapes from the vectors and travels to the nucleus, where the DNA is stored but does not integrate with the body’s DNA [78, 79]. Afterwards, it is transcribed into mRNA that leaves the nucleus to be read and “translated” into spike proteins; these proteins begin to be assembled on the surfaces of infected cells. Once the S proteins or their fragments are recognized by the immune system, it starts to send warning signals and generate specific neutralizing antibodies and activated T cells (CD4+ and CD8+), as well as memory cells of the B- and T-cell types. The protection generated from these vaccines ranges between 62 and 90% (with an average of 70%) [54]. The vectors used with these vaccines have a tough protein coat that helps protect the genetic material inside them. For this reason, the vaccine does not have to stay frozen and can be stored for at least 6 months at refrigerator temperatures (2–8℃) [42].
Oxford–Astrazeneca Vaccine (OAV; AZD 1222; Vaxzevria)
AZD 1222 was developed by Oxford University and the Jenner Institute (AstraZeneca). It was one of the first to begin clinical trials and the only one using a debilitated chimpanzee adenovirus (ChAdOx1). The SARS-CoV-2 spike protein is expressed by the AZD1222 vaccine [81]. The AZD1222 vaccine team published their phase I/II trial interim report in July 2020 and showed that AZD1222 can elicit S protein-specific antibodies and T-cell responses and induce neutralizing antibodies in all participants after the prime-boost regimen [81].
It has an acceptable safety profile and is efficacious in combating symptomatic COVID-19. In addition, this vaccine is effective against the new and more contagious U.K. SARS- CoV-2 variant B.1.1.7 and partially (10% efficacy) against the South African B.1.351 variant [82]. The OAV was reported to have an efficacy ranging from 62 to 90%, according to the two-dosage protocol of SD/SD or LD/SD, respectively [81, 83]. Furthermore, this vaccine can be kept at refrigerator temperatures (2–8 oC) for at least six months, which makes it easy to store, transport, and distribute globally [81, 83]. The OAV triggers strong humoral and cellular immune responses. Again, this vaccine produces minor side effects, such as fatigue and headache [83].
Sputnik-V or Gam-COVID-Vac Vaccine
The SVV vaccine was developed by the Gamaleya Research Institute of Russia and named in memory of the Soviet-era satellite program. This vaccine utilizes a combination of two adenoviruses that are not recognized by the human immune system as foreign [84, 85]. The first dose contains the vectored HAdV-26 vaccine. The booster dose, given after 21 days, is composed of the HAdV-5 vectored vaccine. It can be stored at a standard freezer temperature of -20 °C. The vaccine is safe and well tolerated, and there were no unexpectedly severe adverse effects. Cellular immunity, neutralizing antibodies, and RBD-specific IgG were detected in all participants being vaccinated. The phase 3 trial results showed that the vaccine had an efficacy of 91.4% on Day 28 after the first dose and efficiency above 95% on Day 42 after the first dose [86].
Johnson and Johnson Vaccine (J&J V; JNJ- 78436735)
The Janssen Pharmaceutical Companies of Johnson & Johnson created JNJ. Their candidate is a replicating-defective adenovirus-26-based vector expressing the stabilized pre- fusion S protein of SARS-CoV-2. Their main difference from the CanSino vaccine candidate is the adenovirus serotype. As opposed to the ubiquitous Ad5 serotype, very few people have been exposed to the rare Ad26 serotype; therefore, pre-existing immunity against the vector reducing this candidate’s immunogenicity is not expected to be a major concern. The second advantage of this candidate is that the dosing schedule involves a single immunization [54]. In the phase I/II clinical trial, the vaccine JNJ-7843-6735 induced robust humoral and cellular immune responses in middle- aged adults and the elderly [87].
JNJ-78436735 was given to participants at either 0.5 or 1 1011 viral particles per vaccination. The reactogenicity of the vaccine was mild, mainly causing injection site pain, fever, headache, and myalgia. It can produce a neutralizing antibody response in 90% of vaccinated people after four weeks and in all recipients after two months. The JJV shows an efficacy of 66% globally and 72% in the United States. It is also capable of protecting against the SARS-CoV-2 variant of the B.I.351 lineage observed in South Africa. It can be stored for up to 3 months at refrigerator temperatures (2– 8℃) and for 2 years at -20 ℃. It showed 66% effectiveness in preventing infection after a single dose and was capable of preventing 85% of severe COVID-19 cases 28 days after vaccination [54].
AD5-nCoV (Convidecia) Vaccine
The AD5-nCoV vaccine is prepared by the Chinese Can Sino Biologics Company in cooperation with the Academy of Military Medical Sciences. The Convidecia vaccine is based on using human adenovirus serotype 5 in cooperation with the Academy of Military Medical Sciences. The Convidecia vaccine is based on using human adenovirus serotype 5 (Ad5) vectors to deliver the information that codes for SARS- CoV-2 full-length S protein into host cells [54]. It is currently in phase 3 clinical trials, and the Chinese government has already approved it for military use for a period of one year. The efficacy of the vaccine after a one-shot dosage is 65.7%. It has the advantage of being suitable for storage at refrigerator temperatures (2–8 °C). No serious adverse reactions after vaccination have been reported [88].
Recombinant Protein Subunit Vaccines
These types of vaccines utilize no genetic materials but use whole or fragments of viral proteins packed in nanoparticles [89, 90]. This type of vaccine is considered very safe and incapable of causing disease. Five vaccines of this type are in preclinical trials utilizing different protein (peptide) subunits [91]. Since these subunits are poorly immunogenic, they require adjuvants and repeated administrations [90]. They can primarily induce reasonable CD4+ T-cell activation and specific neutralizing antibody responses, but they show poorer stimulation of CD8+ T cells. Three types of recombinant protein subunit vaccines are described in the subsections below; they are in the late stages of phase 3 clinical trials or have received authorization in some countries [92].
Novavax (NVX-Cov2373) Vaccine
The NVX vaccine is manufactured by a Maryland-based company, Novavax, in collaboration with GSK and Sanofi, two companies in the United Kingdom and France, respectively. It is a recombinant protein nanoparticle vaccine composed of trimeric spike glycoproteins and a potent Matrix-M1 adjuvant. Attaching viral proteins to a nanoparticle carrier is used to aid efficient delivery and uptake by body cells [9]. The vaccine is administered in two doses, three weeks apart, by intramuscular injection. It can produce a strong antibody response as well as T-cell activation [93]. It is stable at refrigerator temperatures and has an efficacy of 89.3%, reaching up to 96% in a U.K. clinical trial [92].
ZF 2001 (RBD Dimer) Vaccine
The latest subunit vaccine candidate to enter Phase 3 clinical studies is the adjuvanted RBD-dimeric antigen designed by Anhui Zhifei Longcom Biopharmaceutical and the Chinese Academy of Medical Sciences. Phase 3 clinical study was launched on December 20, 2020 (http://en.nhc. gov.cn/2020-11/20/c_82209.htm). The ZF 2001 vaccine is administered in a three-dose course, with the doses given 4 weeks apart by intramuscular injection. The efficacy of this vaccine is officially unknown, as it is in a phase 3 clinical trial, but it has been approved for emergency use in Uzbekistan and China [94].
Epivac Corona Vaccine (EVCV)
The EVCV vaccine is manufactured by the Vector Institute, a Russian biological research center. It is based on using fragments of synthetic viral peptides reflecting SARSCoV-2 antigens. It is given in two doses, three weeks apart, by intramuscular injection to people over 18 years of age as well as older people >60 years of age [69]. The developers claimed that it is stable during storage at refrigerator temperatures for up to two years. Its efficacy is officially unknown, and it is awaiting regulatory approval. However, all the volunteers who were administered the EVCV developed specific antibodies against its antigens [69].
DNA Vaccine
Nucleic acid vaccines are genetic vaccines consisting only of DNA or RNA, which are taken up and translated into proteins by host cells and elicit immune responses. Because they contain no viral coat, naked nucleic acids are generally not subject to pre-existing immunity that can hamper the clinical efficacy of recombinant virus vaccines. In terms of higher safety and lower cost of production, nucleic acid vaccines have some major advantages over other types. Post-translational modifications under natural conditions are reproduced by the plasmid-encoded protein, retaining immunogenicity [95] and humoral and cellular immune- stimulating capabilities simultaneously [96]. Although there have been concerns about the safety of DNA vaccines in these early stages of development [97], it appears that viral gene integration into host genes through plasmid vectors is extremely rare [98].
DNA vaccines are routinely constructed from plasmid DNA molecules that encode one or more antigens. Once delivered, the plasmid DNA vaccine is internalized by host cells at the immunization site or by migrating antigen- presenting cells (APCs), where, in order to induce an adaptive immune response, the DNA must enter the cell nucleus [99]. Finally, the target gene is expressed and translated into protein [100]. DNA vaccines are, to some extent, more stable than mRNA-based vaccines. Plasmid DNA technology allows for the simple production of large quantities of vaccines with the possibility of conferring long-term immunity. An advantage of this kind of vaccine is the stimulation of both humoral and cellular immunity [101]. However, the disadvantages looming over DNA vaccines are due to their limitations in processing protein immunogen and the risk of vector chromosomal integration and mutations in the host genome [102].
ZyCoV-D Vaccine
ZyCoV-D has been developed by Zydus Cadila Health Care Limited in India. It is the world’s first plasmid DNA vaccine for COVID-19 ever approved for mankind [103]. This vaccine encodes the spike protein-induced neutralizing antibody responses and T-helper-1 pro-inflammatory interferon- gamma responses in mice, guinea pigs, and rabbits [104]. The pVAX-1 vector is used in conjunction with a specific order encoding the S-protein from the Wuhan strain of SARS-CoV-2. Phase 3 clinical trials show promising results against the delta variant of SARS-CoV-2. During the trial, the vaccine was found to be safe and effective. The preliminary analysis of symptomatic RT-PCR positive cases revealed that ZyCoV-D had a primary efficacy of approximately 66.6%. The third dose of the vaccine proved to be 100% effective against moderate disease [103].
INO-4800 Vaccine
One of the DNA vaccine candidates developed by the US- based Inovio Pharmaceuticals company It can be delivered to cells intradermally. Administration of this vaccine requires the use of an electroporation device called CELLECTRA to make the human cells more permeable and thus enable proper entry and incorporation of the DNA molecule into the cell. This candidate consists of plasmid DNA that, upon administration, prompts human cells to produce the antigenic SARS-CoV-2 spike protein. While DNA vaccines carry certain advantages, including optimal development speeds and thermostability, past trials have shown that producing sufficient immunogenicity can be a challenge [105]. Additionally, administration can often require larger volumes of DNA vaccine compared to more traditional vaccine types, and it requires the use of an electroporation device, which can be inconvenient [105].
BacTRL-Spike Vaccine or Live Bifidobacterium Vaccine
It is developed by Symvivo Corporation in Canada. This vaccine is constituted by Bifidobacterium longum, engineered to deliver synthetic DNA encoding the spike protein from SARS-CoV-2 contained in a plasmid vector. A phase 1 clinical trial is currently underway to assess the safety and immunogenicity profiles of the bacTRL-spike vaccine against SARS-CoV-2 (NCT04334980). The vaccine is administered orally, and the gut colonization by B. longum should provide continuous delivery and expression of SARS-CoV-2S protein- encoding plasmids. A mucosal, systemic humoral, and cell-mediated immune response is foreseen as a result of the translation of this plasmid within the gastrointestinal lymphoid tissues [106].
Gx-19 Vaccine
The GX-19 vaccine has been developed by biotech firm Genexine Inc. of South Korea. The vaccine is a synthetic, soluble, DNA-based candidate. The ectodomain of the S gene has been codon optimized for increased antigen expression in mammalian cells and subcloned into the plasmid pGX27 vector. Preliminary studies have shown that electroporation- enhanced GX-19 induces robust antibody and T cell responses. Furthermore, vaccination of GX-19 was shown to confer effective protection against SARS-CoV-2 challenge at 10 weeks following the last vaccination in immunized non- human primates, supporting further expectations for GX-19 as a vaccine candidate against SARS-CoV-2 in ongoing human clinical trials [107].
Virus-Like Particle Vaccine
Virus-like particles (VLPs) are self-assembled viral structural proteins that mimic the conformation of native viruses but lack the viral genome. The VLP displays multiple copies of the target antigen on its surface and has a size that enhances recognition and subsequent uptake from antigen-presenting cells, therefore promoting its efficient phagocytosis, processing, and presentation by dendritic cells and inducing strong and broad humoral and cellular immune responses [54]. VLPs are unable to replicate or reverse- mutate, suggesting better safety, especially for viruses that cause high morbidity and mortality. Up until now, VLP
vaccines have been commercialized for protection against human papillomavirus and hepatitis B virus [108].
VLPs are generally produced by encoding the viral structural proteins and expressing them in heterologous systems, such as recombinant vaccinia virus, mammalian cells (293T and CHO), baculovirus, yeast expression systems, and plant expression vectors [109]. In practice, VLP-based vaccines are similar to whole inactivated virus vaccines, but the antigenic proteins may be better preserved and exposed to the immune system since no inactivation step is performed. Therefore, it is less likely to affect the immunogenicity of viral proteins due to the destruction of surface epitopes. Moreover, since no live virus is used in any steps of the production, VLPs are conveniently accomplished in low-containment manufacturing settings [110].
None of the VLP vaccines have yet been approved for use, but there are three promising VLP vaccines under development. Firstly, the Canadian company Medicago has genetically engineered plants. It uses the virus-transfected plant Nicotiana benthamiana to express the prefusion trimeric subunit form of the SARS-CoV-2 S-protein and assemble it on the surface of VLPs, which are harvested and used for immunization [54]. VLP vaccine is in phase 2/3 clinical trials and was recently granted Fast Track designation by the U.S. FDA [69]. Secondly, the ContiVir team at the Max Planck Institute for Dynamics of Complex Technical Systems (Magdeburg, Germany) has designed and produced a virus- like particle vaccine. Thirdly, a Georgia-based biotechnology company, GeoVax Atlanta, has used MVA (modified vaccinia virus ankara viral vectors) to express VLPs [111, 112, 113, 114, 115, 116, 117, 118, 119, 120, 121, 122, 123, 124, 125, 126, 127, 128, 129, 130, 131].
Conclusion and Recommendations
Since the discovery of the human coronavirus, new types of coronavirus have kept emerging and have gradually become a serious threat to global public health. Despite their having been almost two decades since the first coronavirus outbreak. Hence the emergence of the SARS-CoV-2 infection caused a health crisis, psychological fear, economic loss, and socio-political turbulence across the world. Thereafter, a historically large number of scientists, clinicians, researchers, and all government officials around the world were mobilized to work together to develop vaccines to mitigate this global disaster. In an unprecedented timeline, the global scientific community has investigated the virus’s origin, genome, and pathogenesis and has developed many different vaccines with virus immunogenicity. Owing to the urgent need for the vaccine, some vaccines get approval before they have been fully developed for emergent use with minor side effects. In addition, the virus can mutate and become the bottleneck for the development of vaccines and their sustainability. Lastly, with the dedication of global scientific communities and all other stakeholders, sooner or later a safer, more efficient and multivalent vaccine will be developed. Based on the above conclusions, the following recommendations were forwarded:
- Despite the need to develop a vaccine quickly, assurance of its safety and efficacy is critical and should be prioritized.
- Although there are several candidate vaccines licensed for urgent use, still safer and more efficacious vaccines with no minor side effects should be developed.
- Vaccines that can be stored and shipped at optimal temperatures should be developed for use in developing countries.
- The virus genome needed to be regularly sequenced and analyzed to advance vaccine development and maintain vaccine sustainability.
- The current vaccine’s S protein should be replaced with the renovated molecules with the required changes in the specific amino acid to effectively combat the upcoming SARS-CoV-2 infection.
- All responsible parties should be committed to developing invaluable pan-coronavirus vaccines that provide broad protection against multiple pathogenic viruses.
Declaration
Acknowledgments
We, authors, warmly extend our heartfelt gratitude to Jimma University College of Agriculture and Veterinary Medicine (JUCAVM), School of Veterinary Medicine, all librarian and computer labs assistant for their cooperation and support during reviewing this article.
Ethical Considerations
Since this article review was compiled with no original research data and prepared by reviewing different published articles, it did not abuse any welfare protocols and comply with international guidelines. So that we would like to firmly endorse that no ethical approval was required for reviewing this article.
Conflict of Interests
We declare that the authors have no conflict of interests or other interests that might be perceived to influence the results and/or discussion reported in this paper.
Availability of Data and Materials
Since we want to work with the scientific and research community, the data underlying the findings of a paper should be publicly available wherever possible and as open as possible. We therefore firmly support and endorse the Findability, Reusability, and Accessibility of this article. So, we prefer to deposit the data in a public repository that meets appropriate standards of archiving, citation, and curation.
Funding
This article review was not funded by any institution. We write this to inform you that, we haven’t any supporting body (Funding Institution) that makes the payment for the Article processing charge (APC). Hence, we would like to ask for the cancellation of APC and publishing this article without any fee.
Author Contributions
All authors contributed to the manuscript to the final submission. Conceptualization and writing the original draft were performed by Bikila Abebe, and validation, visualization and supervision were mainly done by Motuma Debelo, while reviewing and editing were done by Bikila Abebe and Soressa Bakala. Finally, all authors read and approved the final manuscript submission.
References
-
NHCPRC (2020) New coronavirus cases rise to 571 in Chinese mainland.
-
Zhou P, Yang XL, Wang XG, Hu B, Zhang L, et al. (2020) A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 579(7798): 270-273.
-
Gao, Q, Bao L, Mao H, Wang L, Xu K, et al. (2020) Development of an inactivated vaccine candidate for SARS-CoV-2. Science 369(6499): 77-81.
-
Hui DS, Azhar EI, Madani TA, Ntoumi F, Kock R, et al. (2020) The continuing 2019-nCoV epidemic threat of novel coronaviruses to global health–the latest 2019novel coronavirus outbreak in Wuhan, China. Int J Infect Dis 91: 264-266.
-
Gorbalenya AE, Baker SC, Baric RS, de Groot RJ, Drosten C, et al. (2020a) Severe acute respiratory syndrome-related coronavirus: the species and its viruses–a tatement of the Coronavirus Study Group. Bio Rxiv 2: 1-15.
-
Huang HY, Wang SH, Tang Y, Sheng W, Zuo CJ, et al. (2021) Landscape and progress of global COVID-19 vaccine development. Human Vaccines & Immunotherapeutics 17(10): 3276-3280.
-
Hassan S, Sheikh FN, Jamal S, Ezeh JK, Akhtar A, et al. (2020) Coronavirus (COVID-19): A Review of Clinical Features, Diagnosis, and Treatment. Cureus 12: 7355.
-
Singhal T (2020) A Review of Coronavirus Disease-2019 (COVID-19). Indian J Pediatr 87(4): 281-286.
-
Keech C, Albert G, Cho I, Robertson A, Reed P, et al. (2020) Phase 1–2 Trial of a SARS-CoV-2 Recombinant Spike Protein Nanoparticle Vaccine. N Engl J Med 383(24): 2320-2332.
-
Goldsmith CS, Tatti KM, Ksiazek TG, Rollin PE, Comer GA, et al. (2004) Ultrastructural characterization of SARS coronavirus. Emerg Infect Dis 10(2): 320-326.
-
Lu R, Zhao X, Li J, Niu P, Yang B, et al. (2020) Genomic characterisation and epidemiology of 2019 novel coronavirus: implications for virus origins and receptor binding. Lancet 395(10224): 565-574.
-
Lam TT, Jia N, Zhang YW, Shum MH, Jiang JF, et al. (2020) Identifying SARS-CoV-2-related coronaviruses in Malayan pangolins. Nature 583(7815): 282-285.
-
Rio CD, Collins LF, Malani P (2020) Long-term health consequences of COVID-19. Jama 324(17): 1723-1724.
-
Li Q, Guan X, Wu P, Wang X, Zhou L, et al. (2020) Early transmission dynamics in Wuhan, China, of Novel Coronavirus-Infected Pneumonia. N Engl J Med 382(13): 1199-1207.
-
Jeon KY (2020) COVID-19 Vaccines-Safety First, Alleged Greater Good Last. Am J Epidemiol Public Health 4(4): 12-16.
-
Du L, He Y, Zhou Y, Liu S, Zheng BJ, et al. (2009) The spike protein of SARS-CoV–a target for vaccine and therapeutic development. Nat Rev Microbiol 7(3): 226-236.
-
Lee P, Kim CU, Seo SH, Kim DJ (2021) Current Status of COVID-19 Vaccine Development: Focusing on Antigen Design and Clinical Trials on Later Stages. Immune Netw 21(1): 1-18.
-
Grun GC (2021) COVID-19 Vaccine Development: What’s the Progress. DW Agency.
-
Forni G, Mantovani A (2021) COVID-19 vaccines: Where we stand and challenges ahead. Cell Death Differ 28: 626-639.
-
Burrell C, Howard C, Murphy F (2016) Fenner and White’s medical virology. 5th (Edn.), United States, Academic Press, pp: 583.
-
Kramer A, Schwebke I, Kampf G (2006) How long do nosocomial pathogens persist on inanimate surfaces? A systematic review. BMC Infect Dis 6: 130.
-
Mittal A, Manjunath K, Ranjan RK, Kaushik S, Kumar S, et al. (2020) COVID-19 pandemic: Insights into structure, function, and hACE2 receptor recognition by SARS- CoV-2. PLoS Pathog 16(8): 1-19.
-
Masters PS (2006) The molecular biology of coronaviruses. Adv Virus Res 66: 193-292.
-
Chen Y, Liu Q, Guo D (2020) Emerging coronaviruses: genome structure, replication, and pathogenesis. J Med Virol 92(4): 418-423.
-
Enjuanes L, Zuniga S, Castano-Rodriguez C, Gutierrez- Alvarez J, Canton J, et al. (2016) Molecular Basis of Coronavirus Virulence and Vaccine Development. Adv Virus Res 96: 245-286.
-
Li G, Chen X, Xu A (2003) Profile of specific antibodies to the SARS-associated coronavirus. N Engl J Med 349(5): 508-909.
-
Williams AE, Chambers RC (2014) The mercurial nature of neutrophils: still an enigma in ARDS. Am J Physiol Lung Cell Mol Physiol 306(3): 217-230.
-
Beniac DR, Andonov A, Grudeski E, Booth TF (2006) Architecture of the SARS coronavirus prefusion spike. Nat Struct Mol Biol 13(8): 751-752.
-
DeDiego ML, Álvarez E, Almazán F, Rejas MT, Lamirande E, et al. (2007) A severe acute respiratory syndrome coronavirus that lacks the E gene is attenuated in vitro and in vivo. J Virol 81(4): 1701-1713.
-
Cui L, Wang H, Ji Y, Yang J, Xu S, et al. (2015) The nucleocapsid protein of coronaviruses acts as a viral suppressor of RNA silencing in mammalian cells. J Virol 89(17): 9029-9043.
-
Baxter D (2007) Active and passive immunity, vaccine types, excipients and licensing. Occup Med 57: 552-556.
-
Noor R (2021) Developmental status of the potential vaccines for the mitigation of the COVID-19 pandemic and a focus on the effectiveness of the Pfizer-BioNTech and Moderna mRNA vaccines. Curr Clin Microbiol Rep 8(3): 178-185.
-
Dutta AK (2020) Vaccine against Covid-19 disease - present status of development. Indian J. Pediatr 87(10): 810-816.
-
Huang C, Wang Y, Li X, Ren L, Zhao J, et al. (2020) Clinical Features of Patients Infected with 2019 Novel Coronavirus in Wuhan, China. Lancet 395(10223): 497- 506.
-
Challen R, Brooks-Pollock E, Read JM, Dyson L, Tsaneva- Atanasova K, et al. (2021) Risk of Mortality in Patients Infected with SARS-CoV-2 Variant of Concern 202012/1: Matched Cohort Study. BMJ 372: 579.
-
Bernal JL, Andrews N, Gower C, Robertson C, Stowe J, et al. (2021) Effectiveness of the Pfizer-BioNTech and Oxford-AstraZeneca Vaccines on Covid-19 Related Symptoms, Hospital Admissions, and Mortality in Older Adults in England: Test Negative Case-Control study. BMJ 373: 1088.
-
Tsai CM (2021) Universal COVID-19 Vaccine Targeting SARS-CoV-2 Envelope Protein. World Journal of Vaccines 11(3): 19-27.
-
Wang F, Kream RM, Stefano GB (2020) An Evidence Based Perspective on mRNA-SARS-CoV-2 Vaccine Development. Med Sci Monit 26: 1-8.
-
Mellet J, Pepper MS (2021) A COVID-19 Vaccine: Big Strides Come with Big Challenges. Vaccines 9(1): 39.
-
Wang H, Zhang Y, Huang B, Deng W, Quan Y, et al. (2020) Development of an inactivated vaccine candidate, BBIBP- CorV, with potent protection against SARS-CoV-2. Cell 182(3): 713-721.
-
Liu C, Mendonça L, Yang Y, Gao, Y, Shen C, et al. (2020) The Architecture of Inactivated SARS-CoV-2 with Post fusion Spikes Revealed by Cryo-EM and Cryo-ET. Structure 28(11): 1218-1224.
-
Peng Y, Mentzer AJ, Liu G, Yao X, Yin Z, et al. (2020) Broad and strong memory CD4+ and CD8+ T cells induced by SARS-CoV-2 in UK convalescent individuals following COVID-19. Nat Immunol 21(11): 1336-1345.
-
Li JX, Zhu FC (2021) Adjuvantation helps to optimise COVID-19 vaccine candidate. Lancet Infect Dis 21(7): 891-893.
-
Ganneru B, Jogdand H, Dharam VK, Molugu NR, Prasad SD, et al. (2020) Evaluation of safety and immunogenicity of an adjuvanted, TH-1 skewed, whole virion inactivated SARS-CoV-2 Vaccine-BBV152. Bio Rxiv 2: 1-32.
-
Simon HU, Karaulov AV, Bachmann MF (2020) Strategies to Prevent SARS-CoV-2-Mediated Eosinophilic Disease in Association with COVID-19 Vaccination and Infection. Int Arch Allergy Immunol 181(8): 624-628.
-
Munoz FM, Cramer JP, Dekker CL, Dudley MZ, Graham BS, et al. (2021) Vaccine-associated enhanced disease: Case definition and guidelines for data collection, analysis, and presentation of immunization safety data. Vaccine 39(22): 3053-3066.
-
Klasse PJ, Nixon DF, Moore JP (2021) Immunogenicity of clinically relevant SARS-CoV-2 vaccines in nonhuman primates and humans. Sci Adv 7(12): 1-22.
-
Syeda S, Shrivastava A (2021) COVID-19 Vaccine: The Fight Against SARS-CoV-2 Infection. Vantage Jou of Them Anal 2(1): 42-66.
-
Xu Z, Shi L, Wang Y, Zhang J, Huang L, et al. (2020) Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Resp Med 8(4): 420-422.
-
Ella R, Reddy S, Jogdand H, Sarangi V, Ganneru B, et al. (2021) Safety and immunogenicity of an inactivated SARS-CoV-2 vaccine, BBV152: Interim results from a double-blind, randomised, multicentre, phase 2 trial, and 3-month follow-up of a double-blind, randomised phase 1 trial. Lancet Infect Dis 21(7): 950-960.
-
Thiagarajan K (2021) what do we know about India’s Covaxin vaccine. BMJ 373: 997.
-
Ella R, Vadrevu KM, Jogdand H, Prasad S, Reddy S, et al. (2021) Safety and immunogenicity of an inactivated SARS-CoV-2 vaccine, BBV152: a double-blind, randomised, phase 1 trial. Lancet Infect Dis 21(5): 637- 646.
-
Wang N, Shang J, Jiang S, Du L (2020) Subunit vaccines against emerging pathogenic human coronaviruses. Front Microbiol 11: 298.
-
Kyriakidis NC, López-Cortés A, González EV, Grimaldos AB, Prado EO, et al. (2021) SARS-CoV-2 vaccines strategies: A comprehensive review of phase 3 candidates. NPJ Vaccines 6(1): 1-17.
-
Zhang Y, Zeng G, Pan H, Li C, Hu Y, et al. (2021) Safety, tolerability, and immunogenicity of an inactivated SARS-CoV-2 vaccine in healthy adults aged 18–59 years: A randomised, double-blind, placebo-controlled, phase 1/2 clinical trial. Lancet Infect Dis 21(2): 181-192.
-
Mullard A (2020) COVID-19 vaccine development pipeline gears up. Lancet 395(10239): 1751-1752.
-
Zhu FC, Li YH, Guan XH, Hou LH, Wang WJ, et al. (2020) Safety, tolerability, and immunogenicity of a recombinant adenovirus type-5 vectored COVID-19 vaccine: A dose-escalation, open label, non-randomised, first-in-human trial. Lancet 395(10240): 1845-1854.
-
Alfagih IM, Aldosari B, AlQuadeib B, Almurshedi A, Alfagih MM, et al. (2020) Nanoparticles as Adjuvants and Nanodelivery Systemsfor mRNA-Based Vaccines. Pharmaceutics 13(1): 45.
-
Jackson LA, Anderson EJ, Rouphael NG, Roberts PC, Makhene M, et al. (2020) An mRNA vaccine against SARS-CoV-2-preliminaryreport. N Engl J Med 383(20): 1920-1931.
-
Houseley J, Tollervey D (2009) The Many Pathways of RNA Degradation. Cell 136(4): 763-776.
-
Seth RB, Sun L, Chen ZJ (2006) Antiviral innate immunity pathways. Cell Res 16(2): 141-147.
-
Zhang C, Maruggi G, Shan H, Li J (2019) Advances in mRNA Vaccines for Infectious Diseases. Front Immunol 10: 594.
-
Pardi N, Hogan MJ, Porter FW, Weissman D (2018) mRNA vaccines-a new era in vaccinology. Nat Rev Drug Discov 17(4): 261-729.
-
Gao M, Fritz DT, Ford LP, Wilusz J (2000) Interaction between a poly (A)-specific ribonuclease and the 5’ cap influences mRNA deadenylation rates in vitro. Mol Cell 5(3): 479-488.
-
Izaurralde E, Lewis J, McGuigan C, Jankowska M, Darzynkiewicz E, et al. (1994) A nuclear cap binding protein complex involved in pre-mRNA splicing. Cell 78(4): 657-668.
-
Park JE, Yi H, Kim Y, Chang H, Kim VN, et al. (2016) Regulation of Poly (A) Tail and Translation during the Somatic Cell Cycle. Mol Cell 62(3): 462-471.
-
Kariko K, Buckstein M, Ni H, Weissman D (2005) Suppression of RNA recognition by Toll-like receptors: the impact of nucleoside modification and the evolutionary origin of RNA. Immunity 23(2): 165-175.
-
Anderson BR, Muramatsu H, Jha BK, Silverman RH, Weissman D, et al. (2011) Nucleoside modifications in RNA limit activation of 2’-5’-oligoadenylate synthetase and increase resistance to cleavage by RNase L. Nucleic Acids Res 39(21): 9329-9338.
-
Abdulla ZA, Al-Bashir SM, Al-Salih NS, Aldamen AA, Abdulazeez MZ, et al. (2021) A Summary of the SARS- CoV-2 Vaccines and Technologies Available or under Development. Pathogens 10(7): 788.
-
Corbett KS, Edwards D, Leist SR, Abiona OM, Boyoglu- Barnum S, et al. (2020) SARS-Co-V-2 mRNA vaccine development enabled by prototype pathogen preparedness. Nature 586(7830): 567-571.
-
Baden LR, El-Sahly HM, Essink B, Kotloff K, Frey S, et al. (2021) Efficacy and Safety of the mRNA-1273 SARS- CoV-2 Vaccine. N Engl J Med 384(5): 403-416.
-
Corbett KS, Flynn B, Foulds KE, Francica JR, Boyoglu- Barnum S, et al. (2020b) Evaluation of the mRNA-1273 vaccine against SARS-CoV-2 in nonhuman primates. N Engl J Med 383(16): 1544-1555.
-
Vogel AB, Kanevsky I, Che Y, wanson KA, Muik A, et al. (2020) BNT162b vaccines are immunogenic and protect non-human primates against SARSCoV-2. BioRxiv 12(11): 421008.
-
Seladi-Schulman J, Goodwin M (2021) Why Do You Need Two Doses for Some COVID-19 Vaccines. Healthline.
-
Amit S, Regev-Yochay G, Afek A, Kreiss Y, Leshem E, et al. (2021) Early rate reductions of SARS-CoV-2 infection and COVID-19 in BNT162b2 vaccine recipients. Lancet 397(10277): 875-877.
-
Polack FP, Thomas SJ, Kitchin N, Absalon J, Gurtman A, et al. (2020) Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N Engl J Med 383(27): 2603-2615.
-
Vogel AB, Kanevsky I, Che Y, Swanson KA, Muik A, et al. (2021) Immunogenic BNT162b vaccines protect rhesus macaques from SARS-CoV-2. Nature 592(7853): 283- 289.
-
Lundstorm K (2020) Application of Viral Vectors for Vaccine Development with a Special Emphasis on COVID-19. Viruses 12(11): 1-27.
-
Zhu N, Zhang D, Wang W, Li X, Yang B, et al. (2020a) A novel coronavirus from patients with pneumonia in China 2019. N Engl J Med 382(8): 727-733.
-
WHO (2020) Draft landscape of COVID-19 candidate vaccines.
-
Voysey M, Clemens SA, Madhi SA, Weckx LY, Folegatti PM, et al. (2021) Safety and efficacy of the ChAdOx1 nCoV- 19 vaccine (AZD1222) against SARS-CoV-2: An interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet 397(10269): 99-111.
-
Wise J (2021) Covid-19: The E484K mutation and the risks it poses. BMJ 372: 359.
-
Knoll MD, Wonodi C (2021) Oxford–AstraZeneca COVID-19 vaccine efficacy. Lancet 397(10269): 72-74.
-
Jones I, Roy P (2021) Sputnik V COVID-19 vaccine candidate appears safe and effective. Lancet 397(10275): 642-643.
-
Logunov DY, Dolzhikova IV, Shcheblyakov DV, Tukhvatulin AI, Zubkova OV, et al. (2021) Safety and efficacy of a rAd26 and rAd5 vector-based heterologous prime-boost COVID-19 vaccine: An interim analysis of a randomised controlled phase 3 trial in Russia. Lancet 397(10275): 671-681.
-
Shim BS, Stadler K, Nguyen HH, Yun CH, Kim DW, et al. (2012) Sublingual immunization with recombinant adenovirus encoding SARS-CoV spike protein induces systemic and mucosal immunity without redirection of the virus to the brain. Virol J 9: 215.
-
Sadoff J, Gars ML, Shukarev G, Heerwegh D, Truyers C, et al. (2020) Safety and immunogenicity of the Ad26. COV2.S COVID-19 vaccine candidate: interim results of a phase 1/2a, double-blind, randomized, placebo- controlled trial. Med Rxiv pp: 1-28.
-
Zhu FC, Guan XH, Li YH, Huang JY, Jiang T, et al. (2020) Immunogenicity and safety of a recombinant adenovirus type-5-vectored COVID-19 vaccine in healthy adults aged 18 years or older: A randomised, double-blind, placebo- controlled, phase 2 trial. Lancet 396(10249): 479-488.
-
Pollet J, Chen WH, Strych U (2021) Recombinant protein vaccines, a proven approach against coronavirus pandemics. Adv Drug Deliv Rev 170: 71-82.
-
Arunachalam PS, Walls AC, Golden N, Atyeo C, Fischinger S, et al. (2021) Adjuvanting a subunit COVID-19 vaccine to in-duce protective immunity. Nature 594(7862): 253- 258.
-
Tan HX, Juno JA, Lee WS, Barber-Axthelm I, Kelly HG, et al. (2021) Immunogenicity of prime-boost protein subunit vaccine strategies against SARS-CoV-2 in mice and macaques. Nat Commun 12(1): 1403.
-
Wadman M (2021) Novavax vaccine delivers 89% efficacy against COVID-19 in UK But is less potent in South Africa. Science.
-
Wadman M (2020) The long shot. Science 370(6517): 649-653.
-
Dai L, Zheng T, Xu K, Han Y, Xu L, et al. (2020) A universal design of beta coronavirus vaccines against COVID-19, MERS, and SARS. Cell 182(3): 722-733.
-
Sardesai NY, Weiner DB (2011) Electroporation delivery of DNA vaccines: prospects for success. Curr Opin Immunol 23(3): 421-429.
-
Liu MA (2011) DNA vaccines: an historical perspective and view to the future. Immunol Rev 239(1): 62-84.
-
Nichols WW, Ledwith BJ, Manam SV, Troilo PJ (1995) Potential DNA vaccine integration into host cell genome. Ann New Y Acad Sci 772(1): 30-39.
-
Sheets RL, Stein J, Manetz TS, Duffy C, Nason M, et al. (2006) Biodistribution of DNA plasmid vaccines against HIV-1, Ebola, Severe Acute Respiratory Syndrome, or West Nile virus is similar, without integration, despite differing plasmid backbones or gene inserts. Toxicol Sci of J Soc Toxicol 91(2): 610-619.
-
Porgador A, Irvine KR, Iwasaki A, Barber BH, Restifo NP, et al. (1998) Predominant role for directly transfected dendritic cells in antigen presentation to CD8+T cells after gene gun immunization. J Exp Med 188(6): 1075- 1082.
-
Leitner WW, Ying H, Restifo NP (1999) DNA and RNA based vaccines: principles, progress and prospects. Vaccine 18(9-10): 765-777.
-
Rauch S, Jasny E, Schmidt KE, Petsch B (2018) New vaccine technologies to combat outbreak situations. Front Immunol 9: 1963.
-
Kutzler MA, Weiner DB (2008) DNA vaccines: ready for prime time. Nat Rev Genet 9(10): 776-788.
-
Teijaro JR, Farber DL (2021) COVID-19 vaccines: Modes of immune activation and future challenges. Nat Rev Immunol 21(1): 195-197.
-
Dey A, Rajanathan TC, Chandra H, Pericherla HP, Kumar S, et al. (2021) Immunogenic potential of DNA vaccine candidate, ZyCoV-D against SARS-CoV-2 in animal models. Vaccine 39(30): 4108-4116.
-
Tregoning JS, Kinnear E (2014) Using plasmids as DNA vaccines for infectious diseases. Microbiol Spectr 2(6).
-
Galdiero M, Galdiero M, Folliero V, Zannella C, De Filippis A, et al. (2021) SARS-CoV-2 vaccine development: where are we. Eur Rev Med Pharmacol Sci 25(6): 2752- 2784.
-
Seo YB, Suh YS, Ryu JI, Jang H, Oh H, et al. (2021) Soluble Spike DNA vaccine provides long-term protective immunity against SAR-CoV-2 in mice and nonhuman primates. Bio Rxiv 9(4): 1-15.
-
Lan J, Deng Y, Chen H, Lu G, Wang W, et al. (2014) Tailoring subunit vaccine immunity with adjuvant combinations and delivery routes using the Middle East respiratory coronavirus (MERS-CoV) receptor-binding domain as an antigen. Plos One 9(11): 1-9.
-
Mohsen MO, Zha L, CabralMiranda G, Bachmann MF (2017) Major findings and recent advances in virus-like particle (VLP)-based vaccines. Semin Immunol 34: 123- 132.
-
Kushnir N, Streatfield SJ, Yusibov V (2012) Virus-like particles as a highly efficient vaccine platform: diversity of targets and production systems and advances in clinical development. Vaccine 31(1): 58-83.
-
Jeyanathan M, Afkhami S, Smaill F, Miller MS, Lichty BD, et al. (2020) Immunological considerations for COVID-19 vaccine strategies. Nat Rev Immun 20(10): 615-632.
-
ClinicalTrails.gov (2022) A Phase III Clinical Trial to Determine the Safety and Efficacy of ZF2001 for Prevention of COVID-19. Anhui Zhifei Longcom Biologic Pharmacy Co.
-
BioRender (2021) An In-Depth Look into the Structure of the SARS-CoV2 Spike Glycoprotein.
-
Bolles M, Deming D, Long K, Agnihothram S, Whitmore A, et al. (2011) A double inactivated severe acute respiratory syndrome coronavirus vaccine provides incomplete protection in mice and induces increased eosinophilic pro-inflammatory pulmonary response upon challenge. J Virol 85(23): 12201-12215.
-
Channappanavar R, Perlman S (2017) Pathogenic human coronavirus infections: causes and consequences of cytokine storm and immunopathology. Semin in immunopathol 39(5): 529-539.
-
National Health Commission of the People’s Republic of China (2020) Vaccine to undergo 3rd phase of trials. China Daily.
-
CureVac Press Release (2021) CVnCoV CureVac’s mRNA-Based Vaccine Candidate against COVID-19.
-
Fan YY, Huang ZT, Li L, Wu MH, Yu T, et al. (2009) Characterization of SARS-CoV-specific memory T cells from recovered individuals 4 years after infection. Arch of virol 154(7): 1093-1099.
-
Folegatti PM, Ewer KJ, Aley PK, Angus B, Becker S, et al. (2020) Safety and immunogenicity of the ChAdOx1 nCoV-19 vaccine against SARS-CoV-2: a preliminary report of a phase 1/2, single-blind, randomised controlled trial. Lancet 396(10249): 467-478.
-
Fujimoto I, Pan J, Takizawa T, Nakanishi Y (2000) Virus clearance through apoptosis dependent phagocytosis of influenza A virus-infected cells by macrophages. J virol 74(7): 3399-3403.
-
Gorbalenya AE, Baker S, Baric R, Groot RD, Drosten C, et al. (2020) The species severe acute respiratory syndrome related coronavirus: classifying2019-nCoV and naming it SARS-CoV-2. Nat Microbiol 5: 536-544.
-
Jeffers SA, Tusell SM, Gillim-Ross L, Hemmila EM, Achenbach JE, et al. (2004) CD209L (L-SIGN) is a receptor for severe acute respiratory syndrome coronavirus. Proc Natl Acad Sci USA 101(44): 15748-15753.
-
Li YD, Chi WY, Su JH, Ferrall L, Hung ChF, et al. (2020) Coronavirus vaccine development: from SARS and MERS to COVID‑19. Jou Biomed Scie 27(1): 104.
-
Marzi A, Gramberg T, Simmons G, Rennekamp AJ, Krumbiegel M, et al. (2004) DC-SIGN and D C - SIGNR interact with the glycoprotein of Marburg virus and the S protein of severe acute respiratory syndrome coronavirus. J Virol 78(21): 12090-12095.
-
Mehta P, McAuley DF, Brown M, Sanchez E, Tattersall RS, et al. (2020) COVID- 19: consider cytokine storm syndromes and immunosuppression. The Lancet 395(10229): 1033-1034.
-
Reuters (2021) Sinopharm’sWuhan unit Reports 72.5% Efficacy for COVID Shot, seeks approval in China.
-
Snijder EJ, Decroly E, Ziebuhr J (2016) The nonstructural proteins directing coronavirus RNA synthesis and processing. Adv Virus Res 96: 59-126.
-
Tseng CT, Sbrana E, Iwata-Yoshikawa N, Newman PC, Garron T, et al. (2012) Immunization with SARS coronavirus vaccines leads to pulmonary immunopathology on challenge with the SARS virus. PLoS ONE 7(4): 35421.
-
Wang C, Wang Z, Wang G, Zhang K, Li W, et al. (2021) COVID-19 in early 2021: current status and looking forward. Signal Transduct Target Ther 6: 114.
-
Yang ZY, Huang Y, Ganesh L, Leung K, Kong WP, et al. (2004) PH-dependent entry of severe acute respiratory syndrome coronavirus is mediated by the spike glycoprotein and enhanced by dendritic cell transfer through DC-SIGN J Virol 78(11): 5642-5650.
-
Yoshikawa T, Hill T, Li K, Peters CJ, Tseng CT, et al. (2009) Severe acute respiratory s y n d r o m e (SARS) coronavirus-induced lung epithelial cytokines exacerbate SARS pathogenesis by modulating intrinsic functions of monocyte-derived macrophages and dendritic cells. Journal 83(7): 3039-3048.
- Update on Malariology and Malaria Vaccines
- Addressing Vaccine Hesitancy in the Age of Measles Resurgence: A Mini-Review
- Exploring Barriers and Facilitators of Group Antenatal Care Implementation in Kaduna State, Nigeria: A Qualitative Evaluation
- The Role of IL-11 in Regenerative Medicine and Tissue Engineering
- New Prediction of Mortality rate of Covid -19 According to WHO Estimation
- Measles Vaccine in Kano, Northern Nigeria: Past, Present and Future