Kounis Syndrome with Syncope, Yasser’s Hypocalcemic Sign, and Possible Pulmonary Embolism after AstraZeneca ChAdOx1 nCoV-19 Vaccine in Elderly; Risk and Management
Rationale: Kounis-Zafras syndrome is an acute coronary syndrome (ACS) caused by exposure to an allergic substance. Interestingly, Wavy triple and Wavy double ECG signs (Yasser’s sign) are new specific diagnostic and therapeutic signs seen in the cases of hypocalcemia. The AstraZeneca ChAdOx1 nCoV-19 Vaccine is a viral vector vaccine for the prevention of COVID-19. This vaccine was developed by the UK Oxford University and British-Swedish company AstraZeneca using the modified chimpanzee adenovirus ChAdOx1. Pulmonary embolism and myocardial infarction are the final steps for thromboembolic cardiorespiratory disease. Atrial fibrillation (AF) is a hallmark of an increasing risk of pathological thrombus formation due to a disruption of physiological hemostatic mechanisms. Patient concerns: An elderly widow Farmer male patient was presented to the physician outpatient clinic with angina, syncope, tachypnea, and latent tetany within 8 hours after injection of AstraZeneca ChAdOx1 nCoV-19 vaccine during the vaccination campaign for a traditional COVID-19 prophylaxis. Diagnosis: Kounis-Zavras syndrome with syncope, Wavy triple sign (Yasser’s sign), COVID-19 reactivity, and possible pulmonary embolism after AstraZeneca ChAdOx1 nCoV-19 vaccine in a senile patient with a silent myocardial infarction and chronic atrial fibrillations. Interventions: Electrocardiography, oxygenation, calcium intravenous infusion, and echocardiography. Outcomes: A dramatic clinical, and electrocardiographic improvement had happened. Lessons: AstraZeneca ChAdOx1 nCoV-19 vaccine may induce Kounis-Zafras syndrome, COVID-19 reactivity, possible pulmonary embolism, and hypocalcemia. The associated Kounis-Zafras syndrome, COVID-19 reactivity, possible pulmonary embolism, and hypocalcemia after AstraZeneca ChAdOx1 nCoV-19 vaccine-inducing Kounis-Zafras syndrome are innovative cardiovascular findings. Atrial fibrillation with silent inferior myocardial infarction, low-targeted INR, senility, and male sex are constellation serious risk factors.
Introduction
Kounis-Zafras syndrome is an acute hypersensitivity coronary syndrome (ACS) induced by exposure to allergens [1, 2]. These allergens may be drugs, insect bites, environmental exposures, foods, or coronary stents [1, 3]. This syndrome was initially described by Kounis and Zavras in 1991 as an “allergic angina syndrome”, “allergic angina” or “allergic myocardial infarction (MI)” [2, 3]. The syndrome is a ubiquitous disease and a final trigger pathway of coronary artery spasm and plaque rupture [1, 3]. There is ACS- associated mast cell activation from allergic, hypersensitivity, or anaphylactoid reactions [3]. Vasospastic allergic angina and allergic MI with occluding thrombus infiltrated by eosinophils and/or mast cells constitute the reported variants of this syndrome. It may affect the cerebral, pulmonary, and mesenteric arteries [1]. The allergic angina commonly starts within one hour of exposure to the offending allergen. Longer onset ACS also have been reported [4]. Variant presentations of the syndrome have been reported [3]. Three different variants of this syndrome have been described: Type I occurs in structurally normal coronary arteries with no cardiovascular risk factors. The coronary spasm was suggested with or without associated acute myocardial infarction (AMI). Type II occurs in patients with pre-existing ischemic heart disease (IHD), in whom the acute release of inflammatory mediators induces CAS that may lead to plaque rupture and MI. Type III occurs in patients with coronary artery stent-associated thrombosis [2, 3, 4, 5, 6]. A Wavy triple ECG (ECG) sign (Yasser’s sign) is a new specific diagnostic sign seen in 97.3% of the cases of hypocalcemia. Wavy triple an ECG sign can be used as a therapeutic guide in the cases of hypocalcemia [7]. A Wavy double ECG sign (Yasser’s sign) was also prescribed in hypocalcemia which is mostly seen with either tachycardia or bradycardia [7, 8]. Pulmonary embolism (PE) is a lethal disease due to dislodged thrombi occluding the pulmonary vasculature most commonly in the lower extremities [9]. The Oxford–AstraZeneca COVID‑19 vaccine is a viral vector vaccine for the prevention of COVID-19. It was developed in the UK by Oxford University and British-Swedish company AstraZeneca using as a vector the modified chimpanzee adenovirus ChAdOx1 [10]. The Oxford–AstraZeneca COVID‑19 vaccine is used to protect against the SARS-CoV-2 virus to prevent COVID-19 infection [11]. There is a rare increase in the risk of the and potentially fatality in recipients of the vaccine [12]. VigiBase reports showed embolic and thrombotic events after vaccination with Oxford–AstraZeneca with an incidence of 0.21 cases per 1 million vaccinated days [13]. The known allergic reactions and anaphylaxis were recorded as side effects of the Oxford– AstraZeneca COVID-19 vaccine [10]. Atherosclerotic plaque rupture or coronary micro-embolization are sequels for coronary thrombus formation and subsequent sudden cardiac death due to acute myocardial infarction [14]. Atrial fibrillation (AF) is a hallmark of an increasing risk of pathological thrombus formation due to a disruption of physiological hemostatic mechanisms due to Virchow’s triad of abnormal blood constituents, vascular wall abnormalities, and abnormal blood flow [15].
Case Presentation
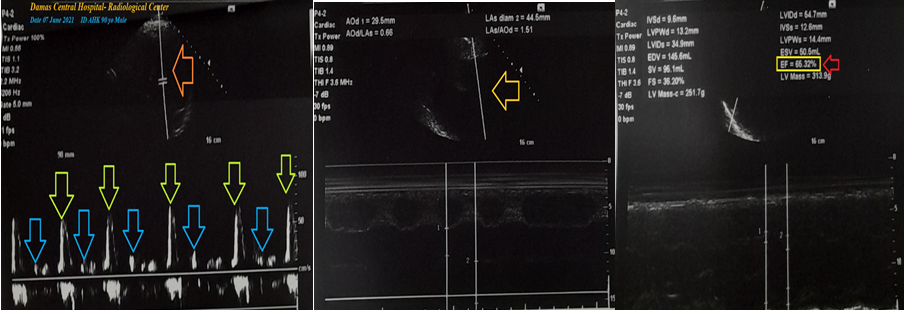
History: A 95-year-old widow male Farmer patient was presented to the physician outpatient clinic (POC) with acute chest pain, transient loss of consciousness, tachypnea, and latent tetany within 8 hours after injection of AstraZeneca ChAdOx1 nCoV-19 Vaccine for a traditional COVID-19 prophylaxis. The chest pain was angina. Circumorally, numbness and extremities paresthesia were associated symptoms. He gave an old history of AF about 15 years ago. He continued on warfarin 5mg (OD), aspocid 75mg (OD), nitroglycerine retard 2.5mg (BID), and bisoprolol 5mg (OD). Clinical examination: Upon general physical examination; the patient was sweaty and distressed, with an irregular pulse rate (AF with VR of 76), blood pressure (BP) of 110/70 mmHg, respiratory rate of 22 bpm, a temperature of 36°C, and pulse oximeter of oxygen (O2) saturation of 95%. Tests for provocative latent tetany were positive. No more relevant clinical data were noted during the clinical examination. The patient refused the referral for admission to the intensive care unit (ICU). Management and investigations: He managed initially at the POC then at home as an angina, COVID-19 reactivity, and hypocalcemia post-AstraZeneca ChAdOx1 nCoV-19 vaccine. Initially, the patient was treated with O2 inhalation by O2 inhalation via an oxygen generator (100%, by nasal mask, 5L/min). The patient was maintained and treated with aspirin; 4 oral tablets (75 mg, then OD), clopidogrel; 4 oral tablets (75 mg, then OD), diltiazem tablets (60 mg, OD), enoxaparin SC (60 mg, BID), oral nitroglycerine capsule (2.5 mg, BID), and atorvastatin (20 mg, OD). Cefotaxime vial (1000 mg IV TDS), azithromycin tablets (500 mg, OD), and hydrocortisone sodium succinate (100 mg IV BID) were added. Two calcium gluconate ampoules (10 ml 10% over IV over 20 minutes) were given as an emergency dose and repeated every 12 hours. The patient was monitored hourly for vital signs and O2 saturation for a few hours. The initial ECG was done on the initial presentation to the POC showing AF (of VR 77), with ST-segment depression in the inferior and anterolateral leads (II, III, and V4-6), ST-segment elevation in aVR, evidence of LAD, Wavy triple ECG sign (Yasser’s sign; I, II, aVF, and V3) Wavy double ECG sign (Yasser’s sign; V2) and pathological Q waves in inferior leads (III and aVF) (Figure 1A). The second ECG tracing was taken within 1 minute of the above ECG tracing showing AF (of VR 83) with ST-segment depression in the inferior and anterolateral leads (I, II, and V3-6), ST-segment elevation in aVR, evidence of LAD, Wavy double ECG sign (Yasser’s sign; II), and pathological Q waves in inferior leads (III and aVF) (Figure 1B). The third ECG tracing was taken within 24 hours of the above ECG tracing and after the initial treatment showing AF (of VR 97) with normalization of ST-segment elevation in aVR, normalization of ST-segment depression, disappearance of Wavy triple ECG sign, disappearance of Wavy double ECG sign, and pathological Q waves in inferior leads (III and aVF) (Figure 1C). The initial complete blood count (CBC); Hb was 13.2 g/dl, RBCs; 4.76*103/mm3, WBCs; 5.6*103/mm3 (Neutrophils; 74.8 %, Lymphocytes: 20.5%, Monocytes; 4.7%, Eosinophils; 0% and Basophils 0%), Platelets; 145*103/mm3. CRP was 25.96. SGPT was (21 U/L) and SGOT was (17 U/ L). AFP was 2.43 IU/ml. Serum albumen was 2.8 gm/dl. Serum creatinine was (1.14 mg/ dl) and blood urea was (28 mg/dl). RBS was (83 mg/dl). D-dimer was 0.61ug/ml. Ionized calcium was (3.9mg/d). INR was 1.33 with a prothrombin time of 17 seconds. The troponin test was 0.28 ng/ml. was done within 3 days after the POC presentation showing a good LV systolic function of an EF of 65.32% (red arrow), grade I diastolic dysfunction, tricuspid regurgitation, right side dilation, and left atrial dilation (Figure 2). Kounis-Zavras syndrome with syncope, Wavy triple sign (Yasser’s sign), COVID-19 reactivity, and possible pulmonary embolism after AstraZeneca ChAdOx1 nCoV-19 vaccine in a senile patient with a silent myocardial infarction and chronic atrial fibrillations was the most probable diagnosis. Within three days of the above at-home management, the patient finally showed nearly complete clinical and ECG improvement. The patient was continued on aspirin tablets (75 mg, OD), diltiazem tablets (60 mg, OD), oral nitroglycerine capsules (2.5 mg, BID), warfarin (5mg, OD), oral calcium, and Vitamin-D preparations for 30 days with further recommended cardiac and immunological follow-up.
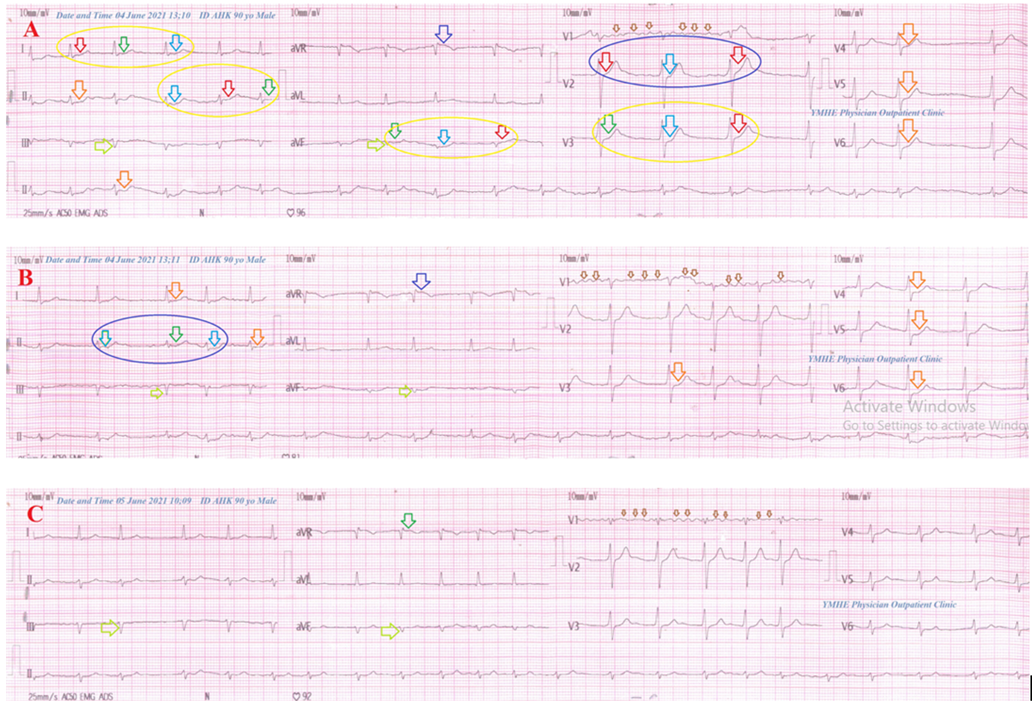
Figure 1: Serial ECG tracings; A: tracing was done on the initial presentation to the POC showing AF (of VR 77; small brown arrows), with ST-segment depression in the inferior and anterolateral leads (orange arrows; II, III, and V4-6), ST-segment elevation (dark blue arrow; aVR), evidence of LAD, Wavy triple ECG sign (Yasser’s sign; I, II, aVF, and V3, light blue, red, and green arrows in yellow circle) Wavy double ECG sign (Yasser’s sign; V2, light blue and red arrows in blue circle) and pathological Q waves in inferior leads (lime arrows; III and aVF). B: tracing was taken within 1 minute of the above ECG tracing showing AF (of VR 83; small brown arrows) with ST-segment depression in the inferior and anterolateral leads (orange arrows; I, II, and V3-6), ST-segment elevation (dark blue arrow; aVR), evidence of LAD, Wavy double ECG sign (Yasser’s sign; II, light blue and green arrows), and pathological Q waves in inferior leads (lime arrows; III and aVF). C: tracing was taken within 24 hours of the above ECG tracing after the initial treatment showing AF (of VR 97; small brown arrows) with normalization of ST- segment elevation (green arrow; aVR), normalization of ST-segment depression, the disappearance of Wavy triple ECG sign, the disappearance of Wavy double ECG sign, and pathological Q waves in inferior leads (lime arrows; III and aVF).
Discussion
Overview
• An elderly widow Farmer male patient was presented to the POC with angina, syncope, and latent tetany within 8 hours after injection of AstraZeneca ChAdOx1 nCoV-19 vaccine during the vaccination campaign for a traditional COVID-19 prophylaxis.
• The primary objective for my case study was the presence of an elderly, widow, male, a Farmer patient was presented to the POC with angina, syncope, tachypnea, and latent tetany. Naranjo’s probability scale in the current case study was +8. It means that there was a probable relationship between these adverse drug reactions and the causing AstraZeneca ChAdOx1 nCoV- 19 vaccine vial (Table 1).
| S. No | Question | Yes | No | Do Not Know | Score |
|---|---|---|---|---|---|
| 1 2 3 4 5 6 7 8 9 10 | Are there previous conclusive reports on this reaction? | 1 2 1 2 -1 -1 1 1 1 1 | 0 -1 0 -1 2 1 0 0 0 0 | 0 0 0 0 0 0 0 0 0 0 | 1 2 1 0 2 0 1 0 0 1 |
| Did the adverse event appear after the suspected drug was administered? | |||||
| Did the adverse event improve when the drug was discontinued or a specific antago- nist was administered? | |||||
| Did the adverse event reappear when the drug was re-administered? | |||||
| Are there alternative causes that could on their own have caused the reaction? | |||||
| 6. Did the reaction reappear when a placebo was given? | |||||
| Was the drug detected in blood or other fluids in concentrations known to be toxic? | |||||
| Was the reaction more severe when the dose was increased or less severe when the dose was decreased? | |||||
| Did the patient have a similar reaction to the same or similar drugs in any previous exposure? | |||||
| Was the adverse event confirmed by any objective evidence? | |||||
| Total Score: +8 |
Table 1: Naranjo Algorithm-Adverse Drug Reaction (ADR) Probability Scale in the case report.
- The secondary objective for my case study was the question; how would you manage the case?
- The presence of angina after injection of AstraZeneca ChAdOx1 nCoV-19 vaccine in a previous MI and chronic AF will strengthen the diagnosis of type II Kounis-Zafras syndrome which is an allergic ACS [2, 3, 4, 5, 6].
- The current ST-segment depression in the inferior and anterolateral leads with negative troponin indicates the presence of unstable angina.
- The syncope, ECG ST-segment elevation in the aVR lead, elevated D-dimer, echocardiographic evidence of dilated right side of the heart suggest the possible presence of pulmonary embolism.
- The dramatic normalization of ST-segment depression after the initial treatment may be interpreted as a coronary artery spasm.
- Elevated CRP, elevated neutrophil count, and reduced lymphocytic count may be suggested for
- Clinically, tachypnea, numbness, and paresthesia of extremities with positive tests for latent tetany, laboratory lower ionized calcium, Wavy double ECG sign, and Wavy triple ECG sign (Yasser’s signs) are more parallel to hypocalcemia (Figures 1A and 1B).
- The changeable of affected leads from ECG tracing to another tracing in the Wavy double ECG sign will be a signal to the diagnosis of Movable phenomenon or Yasser’s phenomenon of hypocalcemia (Figures 1A-1C).
- Movable phenomenon or Yasser’s phenomenon of hypocalcemia is a signal for associated tachypnea in the current case.
- The presence of a changeable Wavy triple sign in ECG is a hallmark of the Movable phenomenon (Yasser’s phenomenon) of hypocalcemia [8]. The Wavy triple ECG sign (Yasser’s sign) is a recently innovated diagnostic sign in hypocalcemia [7]. The author’s interpretations are based on the following:
- Different successive three beats in the same lead are affected.
- All ECG leads can be implicated.
- An associated elevated beat is seen with the first of the successive three beats, a depressing beat with the second beat, and an isoelectric ST-segment in the third one.
- The elevated beat is either accompanied by ST-segment elevation or just an elevated beat above the isoelectric line.
- Also, the depressed beat is either associated with ST- segment depression or just a depressing beat below the isoelectric line.
- The configuration for depressions, elevations, and isoelectricities of the ST segment for the subsequent three beats are variable from case to case. So, this arrangement is non-conditional.
- Mostly, there is no participation among the involved leads. The author intended that is not conditionally included in a special coronary artery for the affected leads [7, 8].
- Tachypnea was a possible cause of hypocalcemia and subsequent Wavy triple ECG sign, Wavy double ECG sign, and Movable-weaning phenomenon of hypocalcemia [7, 8].
- Acute ST-segment elevation myocardial infarction (STEMI) is the most implicated differential diagnosis. The ECG against it.
- I can’t compare the current case with similar conditions. There are no similar or known cases with the same management for near comparison.
- The only limitation of the current study was the unavailability of a new CT pulmonary angiography.
Conclusion and Recommendations
- AstraZeneca ChAdOx1 nCoV-19 vaccine may be inducing Kounis-Zafras syndrome, COVID-19 reactivity, possible pulmonary embolism, and hypocalcemia.
- The associated Kounis-Zafras syndrome, COVID-19 reactivity, possible pulmonary embolism, and hypocalcemia after AstraZeneca ChAdOx1 nCoV-19 vaccine-inducing Kounis-Zafras syndrome are innovative cardiovascular findings.
- Atrial fibrillation with silent inferior myocardial infarction, low-targeted INR, senility, and male sex are constellation serious risk factors.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
I wish to thank my wife for saving time and improving the conditions for helping me.
References
-
Kounis NG (2016) Kounis syndrome: an update on epidemiology, pathogenesis, diagnosis and therapeutic management. Clin Chem Lab Med 54(10): 1545-1559.
-
Fassio F, Losappio L, Antolin-Amerigo D, Peveri S, Pala G, et al. (2016) Kounis syndrome: A concise review with focus on management. Eur J Intern Med 30: 7-10.
-
Memon S, Chhabra L, Masrur S, Parker MW (2015) Allergic acute coronary syndrome (Kounis syndrome). Baylor University Medical Center Proceedings 28(3): 358-362.
-
Abdelghany M, Subedi R, Shah S, Kozman H (2017) Kounis syndrome: a review article on epidemiology, diagnostic findings, management and complications of allergic acute coronary syndrome. International Journal of Cardiology 232: 1-4.
-
Hermans MAW, Van Lennep JER, van Daele PLA, Bot I (2019) Mast cells in cardiovascular disease: from bench to bedside. International Journal of Molecular Sciences 20(14): 3395.
-
Giovannini M, Koniari I, Mori F, Ricci S, De Simone L, et al. (2020) Kounis syndrome: a clinical entity penetrating from pediatrics to geriatrics. J Geriatr Cardiol 17(5): 294-299.
-
Elsayed YMH (2019) Wavy Triple an Electrocardiographic Sign (Yasser Sign) in Hypocalcemia. A Novel Diagnostic Sign; Retrospective Observational Study. EC Emergency Medicine and Critical Care (ECEC) 3(2): 1-2.
-
Elsayed YMH (2012) Movable-Weaning off an Electrocardiographic Phenomenon in Hypocalcemia (Changeable Phenomenon or Yasser’s Phenomenon of Hypocalcemia)-Retrospective-Observational Study. CPQ Medicine 11(1): 01-35.
-
Cervantes J, Rojas G (2005) Virchow’s Legacy: deep vein thrombosis and pulmonary embolism. World J Surg 29(S1): S30-S34.
-
O’Reilly P (2020) A Phase III study to investigate a vaccine against COVID-19. ISRCTN (Registry) 1-10.
-
European Medicines Agency (2021) Vaxzevria (previously COVID-19 Vaccine AstraZeneca) EPAR.
-
Lai CC, Ko WC, Chen CJ, Chen PY, Huang YC, et al. (2021) COVID-19 vaccines and thrombosis with thrombocytopenia syndrome. Expert Rev Vaccines. 2021 Aug; 20(8): 1027-1035.
-
Smadja DM, Yue QY, Chocron R, Sanchez O, Lillo-Le Louet A (2021) Vaccination against COVID-19: insight from arterial and venous thrombosis occurrence using data from VigiBase. Eur Respir J 58(1): 2100956.
-
Skyschally A, Erbel R, Heusch G (2003) Coronary microembolization. Circ J 67(4): 279-286.
-
Ding WY, Gupta D, Lip GYH (2020) Atrial fibrillation and the prothrombotic state: revisiting Virchow’s triad in 2020. Heart 106(19): 1463-1468.
- Update on Malariology and Malaria Vaccines
- Addressing Vaccine Hesitancy in the Age of Measles Resurgence: A Mini-Review
- Exploring Barriers and Facilitators of Group Antenatal Care Implementation in Kaduna State, Nigeria: A Qualitative Evaluation
- The Role of IL-11 in Regenerative Medicine and Tissue Engineering
- New Prediction of Mortality rate of Covid -19 According to WHO Estimation
- Measles Vaccine in Kano, Northern Nigeria: Past, Present and Future