Antenatal Diagnosis of Meckel Syndrome: A Case Report
Meckel syndrome, also known as Meckel-Gruber syndrome, is a rare and serious genetic disorder belonging to the group of ciliopathies (diseases affecting cell cilia). The syndrome is characterized by a combination of congenital malformations, including: Multi-cystic renal dysplasia: The kidneys are enlarged and filled with cysts, leading to severe renal failure. Occipital encephalocele: Herniation of brain tissue through a defect in the skull. Postaxial polydactyly: Presence of extra fingers or toes. We report a case of Meckel syndrome discovered on prenatal ultrasound in a pregnant patient of 39 weeks’ amenorrhea whose ultrasound scan showed multiple fetal malformations, including severe hydrocephalus, a poly malformative renal syndrome, and postaxial polydactyly affecting all four limbs, in association with an hydramnios. Unfortunately, the newborn passed away one hour later.
Introduction
Meckel-Gruber syndrome is a rare autosomal recessive genetic disorder classified as a ciliopathy. It is characterized by a combination of congenital malformations, including occipital encephalocele, cystic dysplasia of the kidneys, postaxial polydactyly, and cleft palate. The wide variability in clinical presentations reported in the literature highlights the polymorphic nature of this syndrome. Currently, ultrasound is the most effective method for prenatal screening of this lethal poly malformation [1]. Here, we present a case of Meckel-Gruber syndrome diagnosed through prenatal ultrasound in the prepartum period.
Case Presentation
A 33-year-old primigravida, primiparous patient with no prior medical history and no known consanguinity with her spouse was referred by her attending physician for an hydramnios at term while in labor. The current pregnancy was estimated at 39 weeks of amenorrhea, with inadequate prenatal follow-up, and the second-trimester morphological ultrasound had not been performed. The patient was admitted to our maternity unit for urgent delivery.
On admission, she was conscious, a febrile, and hemodynamically stable. Obstetric examination revealed a uterine height of 30 cm, detectable fetal heart sounds, and regular, painful uterine contractions. Vaginal examination showed a median, centralized cervix dilated to two fingers, with cephalic presentation and an intact amniotic sac.
A fetal ultrasound performed upon admission revealed a viable singleton pregnancy with multiple fetal malformations, including severe hydrocephalus, a poly malformative renal syndrome, and postaxial polydactyly affecting all four limbs, in association with an hydramnios. The patient was transferred to the delivery room 30 minutes after admission. After six hours of labor, she delivered a male neonate weighing 2,900 g, with Apgar scores of 4, 5, and 6 at one, five, and ten minutes, respectively. Unfortunately, the newborn passed away one hour later. Macroscopic Examination:
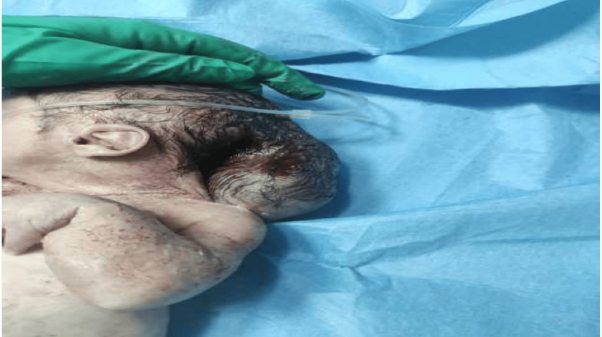
Craniofacial anomalies: Retrognathia with a posterior cleft palate (Figure 1) and occipital encephalocele (Figure 2).
Abdominal findings: Hepatosplenomegaly with ascites. Limb anomalies: Postaxial polydactyly affecting all four distal segments (Figure 3), club feet (Figure 4), and a curved humerus. Spinal and external genitalia: Normal.
The family declined an autopsy examination. Based on the constellation of congenital anomalies, a diagnosis of Meckel-Gruber syndrome was strongly suspected.



Discussion
Meckel-Gruber syndrome (MGS) is a rare, autosomal recessive monogenic disorder with an estimated incidence of approximately 1 in 400 in the general population. Three causative genes have been identified: MKS1 on chromosome 17, MKS2 on chromosome 11, and MKS3 on chromosome 8. The syndrome is typically fatal shortly after birth [2]. MGS is characterized by significant phenotypic variability, with a predominant involvement of the central nervous system (CNS) and kidneys [3]. The syndrome is primarily defined by a triad of occipital encephalocele, cystic renal dysplasia, and postaxial polydactyly. However, additional malformations may be present, including cleft lip and palate, anophthalmia or microphthalmia, urethral atresia, cardiac anomalies, genital malformations, and curvature of the long bones. The major diagnostic criteria include cystic renal dysplasia associated with an hydramnios [4, 5, 6], while minor criteria consist of hepatic fibrosis, occipital encephalocele, polydactyly, and other CNS malformations such as Dandy-Walker malformation and Arnold-Chiari malformation.
Prenatal Diagnosis
• Ultrasound: First-trimester detection may include an anechoic intracranial cyst and/or cranial malformations, while enlarged cystic kidneys can also serve as early indicators [7]. Additional anomalies may become evident in later ultrasounds. • Genetic Testing: Molecular confirmation can be achieved through mutation analysis of associated genes. • Prenatal MRI: This imaging modality can provide a more detailed assessment of brain and kidney malformations. • Amniocentesis: Elevated alpha-fetoprotein (AFP) levels in the amniotic fluid, due to the presence of an encephalocele, may support the diagnosis [8].
If the pregnancy is carried to term, the prognosis remains extremely poor, with perinatal death being the usual outcome.
Genetic Counseling and Differential Diagnosis
Genetic counseling is essential for affected families, as the recurrence risk for subsequent pregnancies is 25%. Karyotyping is necessary to rule out trisomy 13 and trisomy 18, which can present with overlapping features. Differential diagnoses include other ciliopathies such as short-rib polydactyly syndrome, Bardet-Biedl syndrome, Carpenter syndrome, Ellis-van Creveld syndrome, and pseudo-trisomy 13 syndrome, which may present greater diagnostic challenges. The identification of causative genetic mutations plays a crucial role in distinguishing MGS from these syndromes. In our case, the couple refused to have the karyotype done, so we have no idea about the risk of recurrence of the disease in the family.
Conclusions
The phenotypic variability of this monogenic disorder presents challenges in confirming a prenatal diagnosis. However, genetic and molecular analysis to identify the causative gene provides a definitive diagnostic marker and helps predict postnatal outcomes.
References
-
Tanriverdi HA, Hendrik HJ, Ertan K, Schmidt W (2002) European Journal of Ultrasound. Meckel Gruber syndrome: a first trimester diagnosis of a recurrent case. European Journal of Ultrasound 15(1-2): 69-72.
-
Tanriverdi HA, Hendrik HJ, Ertan K, Schmidt W (2002) Meckel Gruber syndrome: a first trimester diagnosis of a recurrent case. European Journal ofUltrasound 15: 69- 72.
-
Nelson J, Nevin NJ, Hanna EJ (1994) Polydactyly in a carrier of the gene for the Meckelsyndrome. Am J Med Genet 53: 207-209.
-
Jha T, Bardhan J, Das B, Patra KK, Dhali B, et al. (2010) Meckel-Gruber syndrome: a rare clinical entity. J Indian Med Assoc 108: 611-612.
-
Desai SR, Wader JV (2004) Meckel Gruber Syndrome--a case report. Indian J Pathol Microbiol. 2004, 47: 430-432.
-
Walsh M, Graupman P (2006) Meckle Gruber syndrome in association with occipital meningocele. Pediatr Neurosurg 42: 333-334.
-
Van Wymersch D, Favre R (1995) Intérêt de l’échographie tridimensionnelle en obstétrique et gynécologie. Réf Gynécol Obstét 31: 82-87.
-
Ickowicz V, Eurin D, Maugey-Laulom B (2006) Meckel- Grüber syndrome: sonography and pathology. Ultrasound ObstetGynecol 27: 296-300.
- The Need for Partner Education and Mental Health Support During Pregnancy and the Postpartum Period
- Application of Combined PGT-A and PGT-M for Reproductive Management in a Couple Carrying GCDH Mutations with Prior Affected Offspring: A Rare Case Report
- The Effect of Using a New Technique Karman Injector (Elif Technique) on the Healing Process of Wound Infection-Case Series
- GSM: Counseling Points to Discuss with Women Fearful of Vaginal Estrogen
- Discrimination and Workplace Harassment (Mobbing) against Women in the Post-Pandemic Era
- Enhancing Maternal Care through Spousal Involvement during Perinatal Period in India