The Effect of Using a New Technique Karman Injector (Elif Technique) on the Healing Process of Wound Infection-Case Series
Our aim in our case series is to present the effectiveness of a minimally invasive method in wound infections that heal slowly. In this case series, the treatment process of a total of 9 patients was discussed. Intravenous (IV) 1x2 g Ceftriaxone and 3x1 100 ml injection solution containing 0.5% 500 mg metronidazole were started on patients who were followed up with wound infection. C-reaktif protein (CRP) and leukocyte levels of the patients were checked at the time of admission and 48-hour intervals. Wound cultures were taken under appropriate conditions at the time of hospitalization from patients who were followed up with wound infection. The vital signs of the patients were checked and recorded. The BMI values of the patients were checked and recorded. Additional risk factors and diseases of the patients were also recorded. Follow-up CRP and leukocyte values of the cases were checked every 48 hours. A significant decrease of over 50% was detected in CRP values during follow-up at 48-hour intervals. The rapid decrease in CRP and leukocyte values was found to be statistically significant (p=0.001). Fever occurred at the time of initial admission, and no high fever was detected during the treatment process. No wound separation occurred in any of the patients. Again, no debridement or secondary suturing was required for infection. The patients did not require additional treatment other than debridement with a Karman injector. As an effective and minimally invasive method, the use of a Karman syringe will be an effective treatment for wound infections.
Abbrevations
SSI: Surgical Site Infection; DM: Diabetes Mellitus; BMI: Body Mass Index; CRP: C-Reactive Protein; GDM: Gestational Diabetes Mellitus.
Introduction
Surgical site infection (SSI) is defined by the Centers for Disease Control and Prevention as a wound infection that occurs within 30 days following a surgical procedure or one year if the implant is left in place and the infection is considered secondary to the surgery [1]. It is one of the most common healthcare-associated infections and occurs following 1-3% of all surgical procedures [2].
SSI rates are much higher in abdominal surgery than in other types of surgery. Various prospective studies show an incidence of 15-25%, depending on the level of contamination [3, 4, 5].
Surgical site infection is preventable and is associated with high morbidity and mortality. In addition to its devastating effect on the patient’s treatment process, it is also associated with prolonged hospital stays and higher costs [6, 7].
It represents one of the most common causes of morbidity in gynecological patients undergoing open surgery and occurs in approximately 2-5% of cases [8].
According to traditional classification types, SSI rates are 2.1% for clean surgery, 3.3% for clean-contaminated cases, 6.4% for contaminated cases, and 7.1% for dirty or infected cases [9, 10].
The risk of SSI in the surgical patient is affected by many factors that can be classified as intrinsic and extrinsic. Local intrinsic factors include tissue injury occurring during surgery, the presence of nonviable or necrotic tissue, the presence of foreign bodies, and microbiological colonization of the skin. Systemic intrinsic factors include conditions such as tissue hypoxia, advanced age, blood transfusion, malnutrition, obesity, diabetes, other chronic diseases, smoking, steroids, and other immunosuppressants [11].
As for extrinsic factors, surgery lasting more than two hours, lack of antibiotic prophylaxis, or contamination during surgery depends on the type of surgery (Clean, clean-contaminated, contaminated, and dirty), among other factors [12].
Superficial SSIs involve only skin and subcutaneous tissue; deep SSIs involve the fascial and muscular layers. The overall SSI rate after laparotomy for gynecological malignancies varies between 1-37% [13, 14, 15].
The rate of wound complications (i.e., superficial SSI) after laparotomy for benign or malignant indications in obese and morbidly obese women is 27-33% [16, 17].
Wound infection places a great burden on hospitals and healthcare systems. Obstetrics and gynecology are areas where issues related to wound healing are particularly relevant. According to literature data, the rate of infected, difficult-to-heal wounds for cesarean section and abdominal hysterectomy, the two most common interventions in obstetrics and gynecology, is 1.8-12.2% and is associated with 0.3-1.2% of cases [18].
Especially in wound infection, which is a common reason for admission, it is important to treat the wound effectively before it is opened. In this study, the existing infection material in the wound was cleaned by using the Karman syringe, and its effect on the patient’s healing process was investigated.
Cases
Case 1: A 43-year-old patient diagnosed with Type 2 diabetes mellitus (DM) as an additional disease was hospitalized with a wound infection on the 7th day after the operation. Our patient’s body mass index (BMI) is 34. Our patient underwent total abdominal hysterectomy and bilateral salpingo-oophorectomy due to complaints of uterine myoma and abnormal uterine bleeding resistant to treatment. The operating incision is the Pfannestiel incision. Our patient’s admission C-reactive protein (CRP) value was 289 mg/L. Leukocyte values reached 14.520 µL. The temperature was measured as 39o and there was Escherichia coli growth in the wound culture.
Case 2: This is a 33-year-old patient with gestational diabetes mellitus (GDM). Our patient’s BMI is 35. Our patient had a cesarean section. Our patient was admitted to our hospital with a wound infection on the 11th postoperative day. Our patient’s CRP value is 359 mg/L. The leukocyte value is 17.150 µL. The temperature was measured as 39.3o and there was staphylococcus aureus growth in the culture sent from the wound site.
Case 3: A 51-year-old patient with no comorbidities. Our patient’s BMI is 32 and he is obese. Our patient underwent a total abdominal hysterectomy and bilateral salpingo- oophorectomy due to an adnexal mass. Our patient was admitted to our hospital on the 9th postoperative day due to a wound infection. Our patient’s CRP value is 410 mg/L. The leukocyte value is 16.450 µL. The temperature was measured at 39o. Staphylococcus aureus and Escherichia coli were grown in the culture sent from the wound site.
Case 4: This is a 32-year-old patient with undiagnosed type 2 DM. Our patient’s BMI is 25 and he is overweight. Our patient came to the emergency room with a Bartholin abscess. At the time of the operation, it was observed that the abscess was very deep and extended to the gluteus. Our patient’s admission CRP value was 456 mg/L. The leukocyte value is 17.125 µL. The temperature was measured at 39o. Staphylococcus aureus and Escherichia coli were grown in the culture sent from the wound site.
Case 5: A 28-year-old morbidly obese patient. Our patient’s BMI is 36. He has no additional diseases. A cesarean section was performed. Our patient was hospitalized due to a wound infection on the 8th postoperative day. Our patient’s CRP value is 356 mg/L. The leukocyte value is 16.512 µL. The temperature was measured at 39o. Staphylococcus aureus and Escherichia coli were grown in the culture sent from the wound site.
Case 6: Our 39-year-old morbidly obese patient with a BMI of 40 and a diagnosis of type 2 DM. Our patient has a
10-year history of type 2 diabetes. A cesarean section was performed on our patient. Our patient was hospitalized due to a wound infection on the 5th postoperative day. Our patient’s CRP value is 256 mg/L. The leukocyte value is 16.321 µL. The temperature was measured at 39o. Staphylococcus aureus and Escherichia coli were grown in the culture sent from the wound site.
Case 7: This is a 33-year-old patient with no comorbidities. Our patient’s BMI is 25. Our patient had a cesarean section. Our patient was admitted to our hospital with a wound infection on the 5th postoperative day. Our patient’s CRP value is 259 mg/L. The leukocyte value is 16.150 µL. The temperature was measured as 39.3o and there was staphylococcus aureus growth in the culture sent from the wound site.
Case 8: A 55-year-old patient with no comorbidities. Our patient’s BMI is 30 and he is obese. Our patient underwent total abdominal hysterectomy and bilateral salpingo- oophorectomy due to complex hyperplasia with atypia. Our patient was admitted to our hospital on the 6th postoperative day due to a wound infection. Our patient’s CRP value is 412 mg/L. The leukocyte value is 16.235 µL. The temperature was measured at 39.5o. Staphylococcus aureus was grown in the culture sent from the wound site. Case 9: This is a 31-year-old patient diagnosed with GDM. Our patient’s BMI is 33. Our patient had a cesarean section. Our patient was admitted to our hospital with a wound infection on the 8th postoperative day. Our patient’s CRP value is 384 mg/L. The leukocyte value is 16.150 µL. The temperature was measured as 39.4o and the culture sent from the wound showed growth of staphylococcus aureus and Escherichia coli.
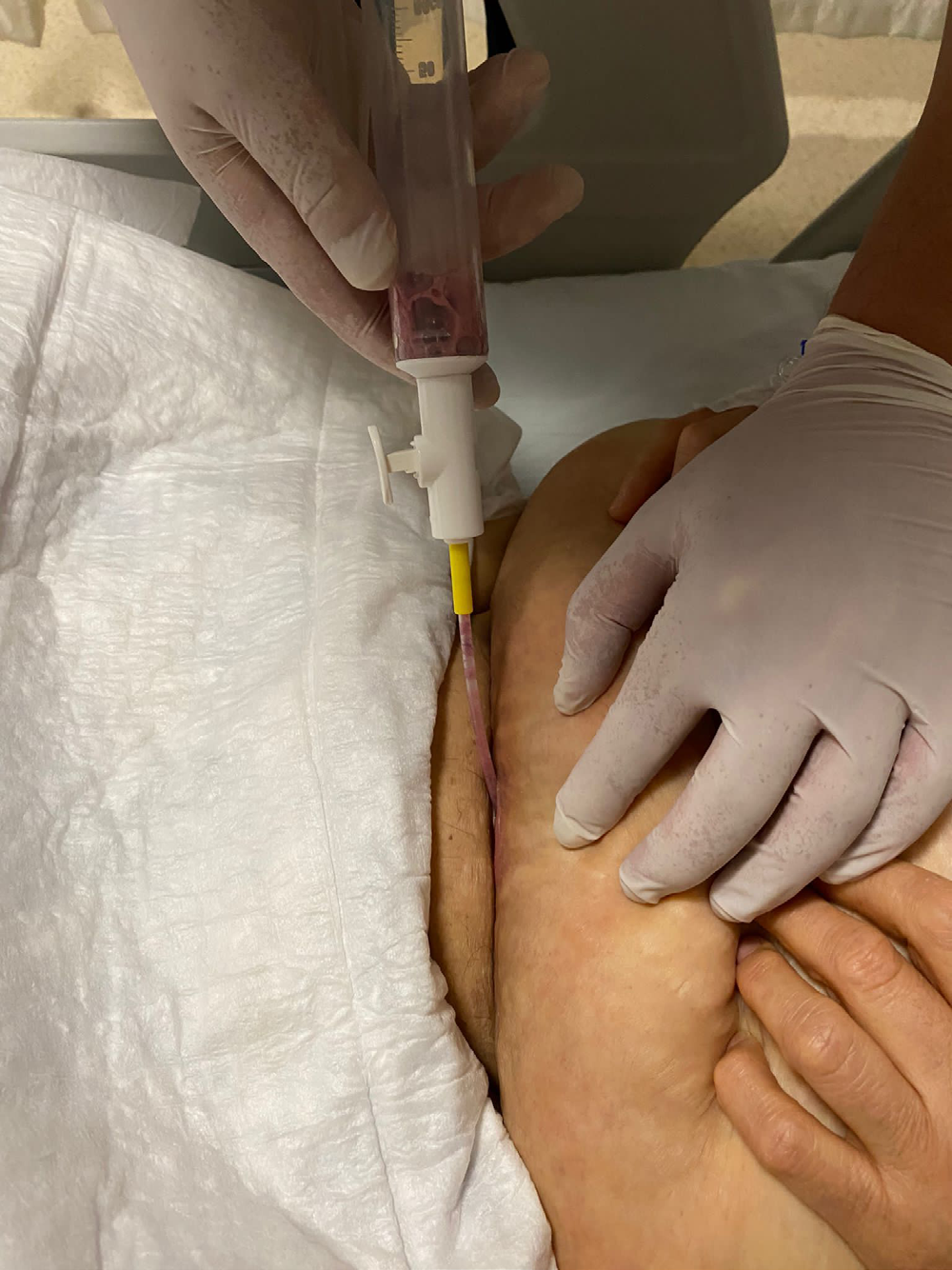
The wound site was not opened in the management of the cases. The area with wound infection was entered with the smallest 4 mm yellow cannula from the corner of the wound. The wound area was thoroughly cleaned with a Karman cannula, leaving no infection material. This process was done two or three times on the first day and repeated once or twice on the other days, depending on the availability of incoming materials. The criterion for terminating the procedure is that the bleeding adipose tissue reaches the Karman syringe. No additional dressing was applied to the wound area of the patients treated with Karman. Additionally, local antibiotic therapy was not applied to the wound site. Povidine-iodine was applied in a thin layer only on the wound area. Wound debridement with the Karman syringe is given in Figure 1.
Intravenous (IV) 1x2 g Ceftriaxone and 3x1 100 ml injection solution containing 0.5% 500 mg metronidazole were started on patients who were followed up with wound infection. CRP and leukocyte levels of the patients were checked at the time of admission and 48-hour intervals. Wound cultures were taken under appropriate conditions at the time of hospitalization from patients who were followed up with wound infection. The vital signs of the patients were checked and recorded. The BMI values of the patients were checked and recorded. Additional risk factors and diseases of the patients were also recorded. General characteristics of the cases are given in Table 1.
| Age | BMI | Comorbidity | Operation | Fever (O) | Leukocyte (µL) | CRP (mg/L) | Culture | |
|---|---|---|---|---|---|---|---|---|
| Case 1 | 43 | 34 | Tip 2 DM | TAH+BSO | 39 | 14.52 | 289 | Escherichia coli |
| Case 2 | 33 | 35 | GDM | CS | 39.3 | 17.15 | 359 | Staphylococcus aureus |
| Case 3 | 51 | 32 | - | TAH+BSO | 39 | 16.45 | 410 | Staphylococcus aures- Escherichia coli |
| Case 4 | 32 | 25 | Tip 2 DM | Bartholin Apsesi | 39 | 17.125 | 456 | Staphylococcus aures- Escherichia coli |
| Case 5 | 28 | 36 | - | CS | 39 | 16.512 | 356 | Staphylococcus aures- Escherichia coli |
| Case 6 | 39 | 40 | Tip 2 DM | CS | 39 | 16.321 | 256 | Staphylococcus aures- Escherichia coli |
| Case 7 | 33 | 25 | - | CS | 39.3 | 16.15 | 259 | Staphylococcus aureus |
| Case 8 | 55 | 30 | - | TAH+BSO | 39.5 | 16.235 | 412 | Staphylococcus aureus |
| Case 9 | 31 | 33 | GDM | CS | 39.4 | 16.15 | 384 | Staphylococcus aures- Escherichia coli |
Table 1: General Specifications.
BMI: Body Mass Index, DM: Diabetes Mellitus, GDM: Gestational Diabetes Mellitus, TAH+BSO: Total Abdominal Hysterectomy+Bilateral Salpingo-Oophorectomy, CS: Caesarean Section, CRP: C-reaktif protein . Table 1: General Specifications.
Follow-up CRP and leukocyte values of the cases were checked every 48 hours. A significant decrease of over 50% was detected in CRP values during follow-up at 48-hour intervals. The rapid decrease in CRP and leukocyte values was found to be statistically significant (p=0.001). Fever occurred at the time of initial admission, and no high fever was detected during the treatment process. No wound separation occurred in any of the patients. Again, no debridement or secondary suturing was required for infection. The patients did not require additional treatment other than debridement with a Karman injector. The infection parameters of the patients during follow-up are given in Table 2.
| At First Application | 48 Hours Later | 96 Hours Later | 144 Hours Later | P Value | |||||
|---|---|---|---|---|---|---|---|---|---|
| Leukocyte (µL) | CRP (mg/L) | Leukocyte (µL) | CRP (mg/L) | Leukocyte (µL) | CRP (mg/L) | Leukocyte (µL) | CRP (mg/L) | ||
| Case 1 | 14.52 | 289 | 9.52 | 145 | 8.15 | 70 | 7.56 | 30 | 0.001* |
| Case 2 | 17.15 | 359 | 10.514 | 179 | 9.235 | 84 | 7.854 | 41 | |
| Case 3 | 16.45 | 410 | 11.51 | 201 | 9.851 | 98 | 8.457 | 48 | |
| Case 4 | 17.125 | 456 | 12.589 | 221 | 10.458 | 109 | 7.894 | 53 | |
| Case 5 | 16.512 | 356 | 11.548 | 175 | 10.429 | 88 | 8.965 | 43 | |
| Case 6 | 16.321 | 256 | 12.598 | 112 | 10.258 | 61 | 7.856 | 29 | |
| Case 7 | 16.15 | 259 | 12.425 | 125 | 10.269 | 61 | 7.965 | 28 | |
| Case 8 | 16.235 | 412 | 13.528 | 210 | 11.258 | 102 | 8.965 | 49 | |
| Case 9 | 16.15 | 384 | 13.652 | 196 | 12.365 | 95 | 9.652 | 46 |
Table 2: Infection Values by Hours.
*Pearson Chi-Square test 95% confidence interval p<0.05 values are significant CRP: C-reaktif protein Table 2: Infection Values by Hours.
Discussion
Diagnosis of a local acute wound infection can often be based on distinct clinical signs and symptoms, such as redness, swelling, pain, and warmth. Sometimes, acute wound infections may persist due to biofilm contamination of surgical hardware such as wires or prostheses [19].
In chronic wound infections, a noticeable delay in healing, persistent inflammation, and recurrent infections with poor response to systemic or topical antimicrobial agents are indicators of chronic biofilm infection [20].
Gynecological operations are included in the clean surgery group. The incidence of wound infection is less than 5% after gynecological operations. The risk of infection can be reduced by shortening the preoperative hospital stay, hexachlorophene showers before surgery, shaving the wound area as much as possible 24 hours before the operation, a careful surgical technique, shortening the operation time as much as possible, and placing drains at a distance of at least 2 cm from the surgical wound area [21].
Local treatment for these infections; includes incision and drainage, irrigation of the wound, and frequent moist dressing. The use of antibiotics should be decided according to the degree of invasion of the infection into the skin, subcutaneous and muscle tissue, and the presence of systemic symptoms [22].
Traditional surgical debridement refers to the removal of devitalized tissue that inhibits the growth of normal tissue to reduce the risk of infection and promote normal wound healing. Multiple debridement techniques include surgical debridement, mechanical debridement, biological debridement (autolytic, enzymatic, honey, and maggot treatments), and auxiliary methods (hydrosurgery, ultrasound, negative pressure wound therapy) [23].
Debridement has an irreplaceable place in chronic wound treatment. Prompt and adequate debridement can reduce the burden of infection, which can subsequently shorten the wound-healing process. In our case series, we aimed to debride the patients without opening the wound. It is the only study in the literature with this feature.
Drainage is a very old topic throughout the history of surgery. The ancient Egyptians first introduced drainage, which became a very important approach in the prevention and treatment of infection, in 2000 BC. He did it around 2000. The purpose of drainage includes evacuation of infectious fluid and liquefied necrotic tissue to remove bacterial culture medium, reduce bioburden, and alleviate stimulation of inflammation in surrounding tissue. Conventionally, drainage is divided into two types: passive drainage and active drainage. Passive drainage, where drainage tube and gauze are most commonly used, generally depends on pressure difference and gravity. Active drainage is usually achieved by external forces such as negative pressure; The representative method is negative pressure wound therapy [24].
Drainage is vital in the preparation of the wound bed and, going further, it is an indispensable part of the entire treatment procedure of the chronic wound. In our case series, a Karman syringe was used for drainage. This has offered a more cost-effective treatment opportunity.
In a systematic review (n=785) in which Webster, et al. [25] examined the effect of negative pressure wound therapy on the healing of surgical wounds and skin grafts, they found that considering the cost and frequent use of the effect of negative pressure wound therapy, the new negative pressure wound therapy designed to be used in clean, closed surgical incisions. It has been stated that there is an urgent need for appropriately powered, high-quality studies to evaluate the effects of wound treatment products.
In the systematic review by Ubbink, et al. [26] in which they examined the effect of topical negative pressure wound therapy applied to acute and chronic wounds, patients with diabetic foot wounds, pressure sores, skin grafts, and acute wounds were evaluated in 13 randomized controlled studies. No effective recovery was observed in patients with diabetic foot wounds and the cost of treatment was found to be high.
In another systematic review by Dumville, et al. [27], the difference between negative pressure wound therapy and moist wound dressings was examined (n=605) and it was determined that negative pressure wound therapy was superior to moist wound dressings in healing diabetic foot wounds.
Regarding debridement, the basis of adequate debridement is to maintain a good command of anatomy that can minimize the amount of living tissue sacrificed and maintain basic biological function [28].
In our case series, we aimed to provide adequate debridement and cause minimal damage to functional tissues with a minimally invasive method. In this respect, it is a treatment that can be effective in wound infections.
While antibacterial treatment is generally necessary for the treatment of wound infection, the widespread use of antibiotics has brought about the emergence of drug-resistant bacteria. When infected with such bacteria, it will not only delay the healing process but also worsen the infection by disruption of the newly formed epithelialization [29].
In patients who underwent drainage and debridement with the Karman injector, faster recovery rates were achieved because bacterial growth was prevented.
Therapeutic wound cleansing aims to remove problematic excessive or infected exudate, foreign body, dirt, or bacterial contamination, as well as crust or necrotic tissue. According to Leaper, et al. [30, 31] the application of therapeutic wound cleansing solutions has the potential to disrupt biofilms and kill other microorganisms as well as planktonic bacteria, while exhibiting low cytotoxic potential. Commonly used cleaning solutions range from potable tap water and sterile normal saline to solutions containing surfactants with or without antimicrobials. Agents such as sterile normal saline are not thought to be effective in removing debris and disrupting biofilms. Therefore, the use of wound cleansing solutions containing surfactants such as undecylenamidopropyl betaine or phenoxyethanol has gained popularity. In our case series, no additional dressing or wound cleaning method was used on the patients.
The diversity of modern wound treatment methods is increasing day by day. A good evaluation of the patient and the wound’s condition before wound treatment is important for the effectiveness of the treatment. Studies increase the diversity of products that protect the wound surface accelerate healing and reveal new treatment options. However, more studies need to be done on this subject to provide effective evidence.
Conclusion
It is important to use the Karman syringe in wound infections because it accelerates the treatment process and is a minimally invasive method. The use of a Karman syringe reduces both the length of hospital stay and the dose of medication administered. Again, the use of a Karman syringe prevents wound separation and other complications and additional surgical procedures.
• Ethics Approval and Consent to Participate Necessary information was given to the patients included in the study. Consent was obtained from the patients included in the study. Our study was conducted in accordance with the principles stated in the Declaration of Helsinki. • Availability of Data and Materials Datasets are available from the corresponding author on reasonable request after permission from the local authorities • Acknowledgment I would like to thank my son Burak and my daughter Elif for their energy during this process. • Funding This research received no external funding.
• Conflict of Interest The authors declare no conflict of interest. • Informed consent Necessary information was given to the patients included in the study. Consent was obtained from the patients included in the study. Our study was conducted in accordance with the principles stated in the Declaration of Helsinki.
References
-
Horan TC, Andrus M, Dudeck MA (2008) CDC/NHSN surveillance definition of health care-associated infection and criteria for specific types of infections in the acute care setting. Am J Infect Control 36(5): 309- 332.
-
Azoury S, Farrow N, Hu Q (2015) Postoperative abdominal wound infection-epidemiology, risk factors, identification, and management. Chron Wound Care Manage Res 2: 137-148.
-
Aga E, Keinan-Boker L, Eithan A, Mais T, Rabinovich A, et al. (2015) Surgical site infections after abdominal surgery: incidence and risk factors. A prospective cohort study. Infect Dis (Lond) 47(11): 761-767.
-
Legesse Laloto T, Hiko Gemeda D, Abdella SH (2017) Incidence and predictors of surgical site infection in Ethiopia: prospective cohort. BMC Infect Dis 17(1): 119.
-
Mawalla B, Mshana SE, Chalya PL, Imirzalioglu C, Mahalu W (2011) Predictors of surgical site infections among patients undergoing major surgery at Bugando Medical Centre in Northwestern Tanzania. BMC Surg 11: 21.
-
de Lissovoy G, Fraeman K, Hutchins V, Murphy D, Song D, et al. (2009) Surgical site infection: incidence and impact on hospital utilization and treatment costs. Am J Infect Control 37(5): 387-397.
-
Kirkland KB, Briggs JP, Trivette SL, Wilkinson WE, Sexton DJ (1999) The impact of surgical-site infections in the 1990s: attributable mortality, excess length of hospitalization, and extra costs. Infect Control Hosp Epidemiol 20(11): 725-730.
-
(2009) ACOG practice bulletin No. 104: antibiotic prophylaxis for gynecologic procedures. Obstet Gynecol. 113(5): 1180-1189.
-
Steiner HL, Strand EA (2017) Surgical-site infection in gynecologic surgery: pathophysiology and prevention. Am J Obstet Gynecol 217(2): 121-128.
-
Rock JA, Jones HW (2015) III Te Linde’s operative gynecology. In: 11th (Edn.), Philadelphia (PA): Lippincott Williams & Wilkins Wolters Kluwer.
-
Mueck KM, Kao LS (2017) Patients at High-Risk for Surgical Site Infection. Surg Infect (Larchmt) 18(4): 440- 446.
-
Gómez-Romero FJ, Fernández-Prada M, Navarro-Gracia JF (2017) Prevention of Surgical Site Infection: Analysis and Narrative Review of Clinical Practice Guidelines. Cir Esp 95(9): 490-502.
-
Schiavone MB, Moukarzel L, Leong K, Zhou QC, Afonso AM, et al. (2017) Surgical site infection reduction bundle in patients with gynecologic cancer undergoing colon surgery. Gynecol Oncol 147(1): 115-119.
-
Bakkum-Gamez JN, Dowdy SC, Borah BJ, Haas LR, Mariani A, et al. (2013) Predictors and costs of surgical site infections in patients with endometrial cancer. Gynecol Oncol 130(1): 100-106.
-
Johnson MP, Kim SJ, Langstraat CL, Jain S, Habermann EB, et al. (2016) Using Bundled Interventions to Reduce Surgical Site Infection After Major Gynecologic Cancer Surgery. Obstet Gynecol 127(6): 1135-1144.
-
Kuroki LM, Mullen MM, Massad LS, Wu N, Liu J, et al. (2017) Wound Complication Rates After Staples or Suture for Midline Vertical Skin Closure in Obese Women: A Randomized Controlled Trial. Obstet Gynecol 130(1): 91-99.
-
Leitao MM, Narain WR, Boccamazzo D, Sioulas V, Cassella D, et al. (2016) Impact of Robotic Platforms on Surgical Approach and Costs in the Management of Morbidly Obese Patients with Newly Diagnosed Uterine Cancer. Ann Surg Oncol 23(7): 2192-2198.
-
Antonsen SL, Meyhoff CS, Lundvall L, Høgdall C (2011) Surgical-site infections and postoperative complications: agreement between the Danish Gynecological Cancer Database and a randomized clinical trial. Acta Obstet Gynecol Scand 90(1): 72-76.
-
Elgharably H, Mann E, Awad H, Ganesh K, Ghatak PD, et al. (2013) First evidence of sternal wound biofilm following cardiac surgery. PLoS On 8(8): e70360.
-
Metcalf DG, Bowler PG, Hurlow J (2014) A clinical algorithm for wound biofilm identification. Journal of wound care 23: 137-142.
-
Boyd ME (1987) Postoperative gynecologic infections. Can J Surg 30: 7-12.
-
Hamsell DL, Bernstein SG, Bawdon RE, Hamsell PG, Heard MC, et al. (1989) Preventing major operative site infection after radical abdominal hysterectomy and pelvic lymphadenoctomy. Gynecol Oncol 35: 55-60.
-
Ersilia L, DeFazio BA, Michael V, Jenny C, Janis E et al. (2016) Current Concepts in Debridement: Science and Strategies. Plastic and Reconstructive Surgery 138(3S): 82S-93S.
-
Robinson JO (1986) Surgical drainage: an historical perspective. Br J Surg 73(6): 422-426.
-
Webster J, Scuffham P, Stankievicz M, Chaboyer W (2014) Negative Pressure Wound Therapy for Skin Grafts and Surgical Wounds Healing By Primary Intention. Cochrane Systematic Review 18(4): CD009261.
-
Ubbink DT, Westerbos SJ, Evans D, Land L, Vermeulen H (2008) Topical negative pressure for treating chronic wounds. Cochrane Database Syst Rev 16(3): CD001898.
-
Liu Z, Dumville JC, Hinchliffe RJ, Cullum N, Game F, et al. (2018) Negative pressure wound therapy for treating foot wounds in people with diabetes mellitus. Cochrane Database Syst Rev 10(10): CD010318.
-
Elraiyah T, Domecq JP, Prutsky G (2016) Kronik diyabetik ayak ülserlerinde debridman yöntemlerinin sistematik bir incelemesi ve meta-analizi. J Vasc Surg 63: 37S-45S.
-
Friedman ND, Temkin E, Carmeli Y (2015) The negative impact of antibiotic resistance. Clin Microbiol Infect 22(5): 416-22.
-
Percival SL, Mayer D, Malone M, Swanson T, Gibson D, et al. (2017) Surfactants and their role in wound cleansing and biofilm management. J Wound Car 26(11): 680-690.
-
Kaehn K, Eberlein T (2009) In-vitro test for comparing the efficacy of wound rinsing solutions. Br J Nurs 18(11): S4-S10.
- The Need for Partner Education and Mental Health Support During Pregnancy and the Postpartum Period
- Application of Combined PGT-A and PGT-M for Reproductive Management in a Couple Carrying GCDH Mutations with Prior Affected Offspring: A Rare Case Report
- GSM: Counseling Points to Discuss with Women Fearful of Vaginal Estrogen
- Antenatal Diagnosis of Meckel Syndrome: A Case Report
- Discrimination and Workplace Harassment (Mobbing) against Women in the Post-Pandemic Era
- Enhancing Maternal Care through Spousal Involvement during Perinatal Period in India