Citation: Riyanto P. Effect of Soy Isoflavones on the Improvement of Acne Vulgaris Severity by Reducing Tumor Necrosis Factor-α Levels. Clin Dermatol J 2017, 2(3): 000120.
*Corresponding author: Dr. Puguh Riyanto, MD, DV, Department of Dermatology and Venereology, Faculty of Medicine, Diponegoro University/Kariadi Hospital; Semarang, Indonesia, Tel: 0816650792; Email: Puguhungaran@gmail.com
Objective: To demonstrate the effect of soy isoflavone on acne vulgaris (AV) severity by reducing tumour necrosis factor- α(TNF-α) in female patients.
Methods: In this study was a clinical study with randomized controled group pretest-posttest design. 40 patients were randomized into 2 groups: soy isoflavones 160 mg/day and control. The duration of this study was 12 weeks. The dependent variable: AV severity, and the intermediate variable: TNF-αlevel.
Results: AV severity before treatment (p = 1.00) and after treatment (p = 0.001). TNF-α before treatment (p = 0.213) and after treatment (p = 0.001). There was a significant correlation between the severity of AV and TNF-α(r=0.75)( p=0.009). Conclusion: Treatment with soy isoflavones 160 mg / day for 12 weeks can improve the degree of AV severity as a result of a decrease in TNF-α.
Keywords: Acne vulgaris severity; Soybean isoflavones; TNF-α
Abbreviation: AV: Acne Vulgaris; TNF-α: Tumor necrosis factor-α; NFκB: Nuclear factor-kappa; BDI: Beck depression inventory; EER: Experimental event rate; CER: Control event rate; RRR: Relative risk reduction; ARR: Absolute risk reduction; NNT: Number needed to treat; DHT: Dihydrotestosterone
IntroductionAcne vulgaris (AV) is a chronic inflammatory disease of pilosebaceous units and one of the most common skin disorders [1-3]. Acne vulgaris is most common in teenagers and adults between the ages of 11 to 30. East Asian ethnicity, such as Japanese, Chinese, and Korean usually showed lower AV prevalence compared with Caucasian, and white people showed higher nodulocystic acne prevalence compared with black people. In Indonesia, an estimated 15 million people suffer from AV between the ages of 13–40 [1]. Acne vulgaris is a dynamic and multifactorial process, involving four main factors, such as excess sebum production, hypercornification of the pilosebaceous ducts, inflammation caused by the colonization of Propionibacterium acnes (P. acnes), and microcome done caused by hyperkeratosis in the infundibulum of the pilosebaceous duct, corneocyte cohesion, and sebum secretion, pro-inflammatory cytokines IL-1, IL-8, and TNF-α in the pathogenesis of AV [4-6].
Isoflavones are flavonoids that act as antioxidant and inhibitor of inflammation. Isoflavone, through the inhibition of nuclear factor-kappa (NFκB) pathway, mitogen-activating protein (MAP) kinase and several cellular signaling, may decrease the expression of proinflammatory cytokines IL-1, IL-8, and TNF-α [7,8]. Animal studies found that isoflavone may inhibit inflammatory response [9]. Another in vitro study showed that isoflavone was able to reduce TNF-α expression [10].
This study aims to prove that 160 mg oral soy isoflavones supplementation for 12 weeks may influence the improvement of AV severity and reduction of TNF- α levels. This study was expected to contribute to science and technology, the betterment of healthcare, and for the benefit of society.
MethodsThis study is a clinical study with randomized pretestposttest controlled group design. This study gave 160 mg of soy isoflavones supplementation in the treatment group and placebo in the control group for 12 weeks. Forty study subjects between the ages of 17–34 were randomized into2 groups, the control and treatment groups. To anticipate dropouts, the subjects were monitored using the schedule of assessment visit guidelines. Samples for this study were female AV patients treated at the Dermatology specialist clinic Ungaran Cosmetic Medic (UCM) Semarang. Subjects were chosen using the consecutive sampling method and double blind treatment. The standard medication used for treatment was 0.025% tretinoin cream in the evening and SPF 15 sunscreen in the morning. Soy isoflavone used in this study was an extract of soy isoflavone produced and standardized by the pharmaceutical industry Nu-Health, California, United States of America. The treatment group was given 2 capsules; each capsule held 400 mg of soy isoflavone extract containing 80 mg of pure isoflavone [1].
Inclusion criteria were female AV patients for the last 3 months, not under any medication, and willing to participate in the study by signing the informed consent form. Exclusion criteria were allergy to soy isoflavone. The independent variable was 160 mg/day soy isoflavone, and the dependent variable was the severity of AV according to Lehmann classification. Two dermatologists assessed the severity of AV, and the variability was then calculated using interclass correlation coefficient and alpha coefficient. The intervening variables in this study were age, body mass index (BMI), mean consumption of isoflavones and soy-based foods according to food recall, stress status according to Beck depression inventory (BDI) score, whereas confounding variables were genetic, ethnicity, environmental pollutants, and chemical substances [1].
Data was analyzed using normality and homogeneity tests for age, job, menstruation status, BMI, BDI score, mean consumption of soy isoflavones, number of AV lesion, and TNF-αlevels. The confounding factors were controlled in the randomization process. This study also analyzed the value of clinical importance, such as experimental event rate (EER), control event rate (CER), relative risk reduction (RRR)= CER–EER/CER, absolute risk reduction (ARR)= CER–EER, and number needed to treat (NNT)= 1/AAR. Calculation for ERR is the number of failure in treatment group or the number of subjects in treatment group, whereas CER is the number of failure in control group or the number of SS in control group. RRR and ARR values are the difference between treatment and control group. NNT value in this study is the number of AV patients treated by 160 mg/day soy isoflavone supplementation for 12 weeks that showed clinical improvement or the number that managed to avoid treatment failure. Statistical significance level was defined at p<0.05 with 95% confidence interval.
The Ethic Committee of the Faculty of Medicine Diponegoro University/Dr. Kariadi General Hospital Semarang had approved this study [1].
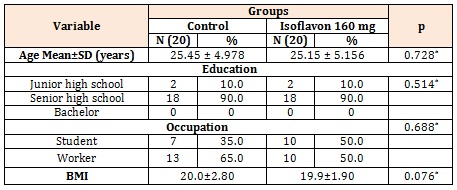
ResultsThe study subjects showed no significant difference (p<0.05) between control and treatment group in mean age or BMI. The majority of our study subjects is high school graduate, and work as laborers (Table 1).
*Mann Whitney, no significant difference (p>0.05) Table 1: Characteristics of Subjects based on age, education, occupation, and BMI between control group and 160 mg/day soy isoflavone group in female AV patients at UCM clinic Semarang, Indonesia. August - November 2015 (N=40).
No Subjects showed moderate and severe BDI score, but 30 subjects (70.0%) had normal and 10 subjects (30.0%) had mild BDI score. There is no statistically significant difference (p>0.05) in BDI score between control and treatment group.
Mean amount of isoflavones consumed per day from soy-based food, such as tempe, tofu and soy milk, based on food recall was 33.5±6.15 mg in the control group, and 31.0±6.30 mg in 160 mg/day isoflavone group. The result of t-test showed no significant difference (p>0.05).
The degree of severity of acne vulgaris in this study after therapy there was a significant improvement in the isoflavone group, while the control group did not improve (Figure 1). Acne vulgaris severity after treatment in the two groups showed a statistically significant difference (p<0.05) (Table 2).
Mean TNF-αlevels before treatment was 500.3±60.54 pg/ml in the control group and 522.3±73.03 pg/ml in the treatment group. Mann Whitney test showed no significant difference (p>0.05) in TNF-α levels between the two study groups before treatment. After receiving treatment for 12 weeks, TNF-αlevels showed a decrease to 334.5±122.74 pg/ml in the control group and 287.7±77.15 pg/ml in the treatment group. Mann Whitney test showed a significant difference (p<0.05) in TNF-α levels between the two study groups after treatment (Table 3).
Mean delta TNF-α levels was –165.9±115.47 pg/ml in the control group and 234.6±96.53 pg/ml in the treatment group. The delta distribution for TNF-α levels in both group was abnormal and Mann Whitney test showed a significant difference (p=0.05) (Table 4).
DiscussionStudy characteristics, including age, education, occupation, stress status, BMI, and mean soy-based food consumption, showed no significant difference between control and soy isoflavone groups.
Acne vulgaris severity before treatment were classified into severity scale as stated by Lehmann, overall no patient had mild AV. Among 40 study subjects, 26 (65.5%) had moderate AV and 14 (35.0%) had severe AV, with equal distribution on both groups with no significant statistical difference (p=0.05). After receiving treatment for 12 weeks, subjects in the treatment group showed improvement in severity, whereas the control group showed no change. Severe acne vulgaris was no longer found in the treatment group.
This effect of soy isoflavone on TNF-αlevels in our female AV patients showed mean delta TNF-αlevels of the treatment group was higher than control group (p<0.05). The administration of 160 mg/day oral soy isoflavone supplementation for 12 weeks in female AV patients while concurrently using topical 0.025% tretinoin cream in the evening and SPF 15 sunscreen in the morning had caused a decrease in the mean difference (delta) of TNF- αlevels between control and treatment groups. There was a significant difference in the decrease of TNF-αlevels after 160 mg/day isoflavone supplementation between control and treatment groups. Soy isoflavone and topical 0.025% tretinoin caused a significant decrease in TNF- αlevels, whereas the decrease in the control group was only caused by 0.025% tretinoin cream. This is in line with the result of an in vitro study where tretinoin and adapalene may reduce TNF-αlevels. Tretinoin is a topical retinoid, vitamin A derivatives, which serves to normalize the proliferation process and has comedolytic effect, and had been used since 30 years ago. Tretinoin is a topical retinoid that was proven effective as monotherapy, and has been the first drug of choice for mild and moderate AV [2,3]. Another study concerning the effect of soy isoflavone on in vitro human prostate cancer cell cultures has demonstrated that isoflavone will reduce the expression of TNF-αand an animal model has demonstrated that isoflavone can inhibit the inflammatory response, by inhibiting the NFκB, MAP kinase and several cellular signaling pathways, and thus reducing the expression of several pro-inflammatory cytokines, such as IL-1, IL-8 and TNF-α [1] (Figure 2).
Studies had proven that soy isoflavone could affect the androgen system. Androgen hormone played an important role in AV, especially in women, where it has been proven that there was a correlation between dihydrotestosterone (DHT) and the number of AV lesions in women [1]. Administration of oral soy isoflavone supplementation with varies dose of 0 mg, 40 mg, 80 mg, 120 mg, and 160 mg/day for 4 weeks at female AV patient receiving standard therapy, have caused significant total lesion reduction difference and show the best dose of soy isoflavone of 160 mg/day. Administration of isoflavone supplementation with the best dose of 160 mg/day for 12 weeks caused significant reduction in total AV lesion and DHT level compared to the standard therapy [1]. Isoflavone has anti-inflammatory effects, several studies in menopausal women found that isoflavone played a role in reducing pro-inflammatory cytokines. Several studies had proven the benefit of 160 mg isoflavone, for example, a study of 160mg isoflavone treatment for 12 weeks in menopausal women found a decrease in TNF-α expression [7,8]. This study found that 160 mg/day isoflavone treatments for 12 weeks would improve quality of life in postmenopausal women [10]. Spearman correlation test showed a significant and strong correlation between AV severity and mean delta TNF- αlevels (p=0.009; r=0.750).
Soy Isoflavones have anti-inflammatory effect, this study improves the severity of acne vulgaris in the therapy group, because isoflavones can decrease TNF-α levels. Inflammatory lesions of acne vulgaris consist of papules, pustus, and nodules. Inflammatory lesions of acne are caused by inflammatory mediators such as TNF- α. Patients with severe acne vulgaris, have inflammatory lesions and higher levels of TNF-α compared with mild and moderate levels. Giving of 160 mg / day soy isoflavones for 12 weeks can improve the severity of acne vulgaris, due to a decrease in TNF-α inflammatory mediators [1].
ConclusionOral supplementation of 160 mg/day soy isoflavones for 12 weeks for female AV patients while concurrently using 0.025% tretinoin cream and SPF 15 sunscreen will improve AV severity by reducing TNF-αlevels.
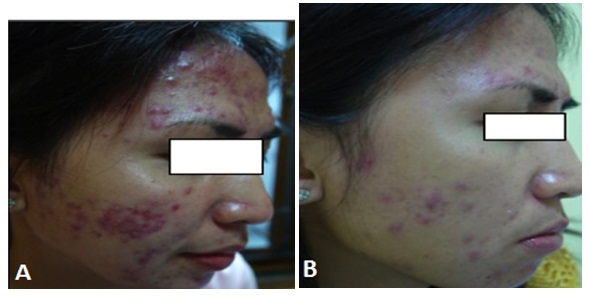
Figure 1: The degree of severity of acne vulgaris in this study after therapy there was a significant improvement in the isoflavone group. A: Before treatment(severe) B: After treatment (mild)
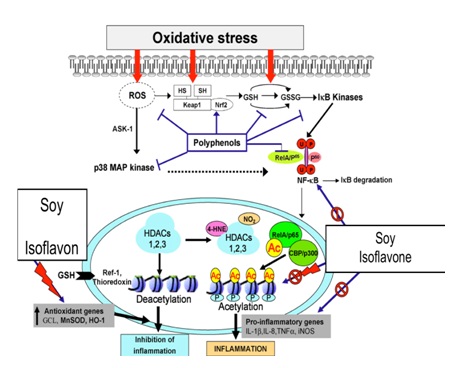
Figure 1: The effect of soy isoflavone will reduce the expression of TNF-αand has demonstrated that isoflavone can inhibit the inflammatory response, by inhibiting the NFκB, MAP kinase and several cellular signaling pathways, and thus reducing the expression of several pro-inflammatory cytokines, such as IL-1, IL-8 and TNF-α
*Mann Whitney, no significant difference (p>0.05)
Table 1: Characteristics of Subjects based on age, education, occupation, and BMI between control group and 160 mg/day soy isoflavone group in female AV patients at UCM clinic Semarang, Indonesia. August - November 2015 (N=40).
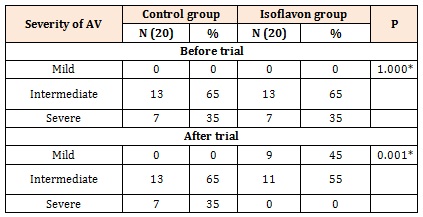
*Chi square test, no significant difference (p>0.05), and significant difference (p<0.05).
Table 2: Acne vulgaris severity between control group and 160 mg soy isoflavone group in female AV patients at UCM clinic Semarang, Indonesia. August-November 2015(N=40).
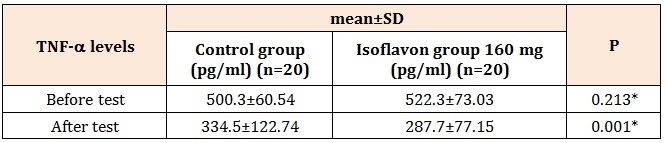
*Mann Whitney, significant difference (p<0.05)
Table 3: TNF-αlevels before and after treatment from the control group and 160 mg isoflavonegroupin female AV patients at UCM clinic Semarang, Indonesia. August - November 2015(N=40).

*Mann Whitney, significant difference (p<0.05)
Table 4: Mean delta TNF-αlevels from the control group and 160 mg isoflavonegroupin female AV patients at UCM clinic Ungaran-Semarang, Indonesia. August-November 2015 (N=40).




