Citation: Hmed BN, et al. The Relationship of Habitual Foods Consuming to Population’s Health. Diabetes Obes Int J 2016, 1(7): 000141.
*Corresponding author: Hmed ben- nasr, Scientific searcher at the Laboratory of Pharmacology at the Medicine Faculty of Sfax, Tunisia, Email: hmedbnasr@gmail.com
Purpose: To evaluate the relationship between specific popular food’s consumption and the prevalence of some chronic diseases.
Methodology: The weekly frequency of couscous and / or macaroni’s consumption was assessed through a questionnaire in a sample of a local population; and its correlation to diabetes mellitus type 2, hypertension and overweight was checked. Our study included 276 volunteers (194 men and 84 women). The collected data was analyzed using Chi square test and Spearman correlation has been checked.
Findings: Our study showed that almost participants (90 %) have at minimum 3 meals composed of couscous and / or macaroni, per week. Our major finding is that 40 to 60 years -old men consuming semolina derivatives (couscous and macaroni) more than seven times a week present higher prevalence of both hypertension and diabetes mellitus type 2 (28.2 % and 25.64 %, respectively), in comparison to whom eating less frequently these foods (12.9 % and 11.1 %, respectively).
Research limitation: This study is strictly based on the diet pattern of this population, and gives information on the possible influence of a specific popular food intake on its health statute; and on basis of the lower sample of population, the obtained results are still discussable.
Originality: Our investigation highlights the requirement of diet diversification to prevent diabetes mellitus type 2 and adult hypertension occurrence.
Keywords: Dietary intake; Cereal foods; Correlation analysis; Diabetes; Cardiovascular disease; Public health
Obesity, diabetes and arterial hypertension are of growing worldwide prevalence. According to the World Health Organization (WHO), there were 972 millions of adult-hypertension, 347 millions of diabetes and 1.4 billion obese patients around the World, in 2008. In Tunisia, there were 250 000 and 207 000 hypertensive and diabetic patients, respectively [1]. These diseases aetiology remains blurry; and several investigations evidenced their relationship to lifestyle, habits, socioeconomic status, and particularly to diet and quality of nutrition [2-7]. More recently, the approach of their genetic determinism emerged [5]. Nowadays, the roles of preventive strategies particularly focusing on dietetic control and recommendations for physical activities in managing these diseases are worldwide admitted [8-11]. Several decades ago, the salt intake of the Mediterranean diet (MD) has been approved in such away. The MD is a diet highly enriched in vegetables and fruits, in association to a lesser meat and saturated fat consumption, facts that decrease the risk factors of many common diseases [12-14]. However, the important geographical, cultural, religious, educational, and socioeconomic variability constitutes a major challenge facing the global appliance of such optimal diet. Because of that, describing the specificity of loco-regional populations’ dietaries may provide important aid to build and rectify models and approaches designated to achieve the optimal healthy diet. Herein, the dietary specificities of a local south- Mediterranean population are investigated and correlated to its public health statute. In raison of that demographic (progressive sedentary lifestyle) influences on the public health [6], the relationship of the studied population’s anthropological behavior with the diseases emergency was also discussed.
Design and MethodologyStudy population
The study was conducted in a southern Tunisian village settled into a desert environment (Figure 1). The recent population has conserved a nomad mode of life based on continual moving for shepherding, for a long time. This village showed an exponential demographic and urbanization increase, indicating for a growing tendency to sedentary lifestyle of the population. Pragmatically, the total urban population grows from 21,000 in 1975 to above 53,000 inhabitants in 2010 (TheNational Institute ofStatisticsof Tunisia’s report, 2010). The transition from continual moving to sedentary lifestyle, in conjunction to the important socio-economic improvement (education and, infrastructure and services’ amelioration), is suspected to influence the public health statute; usually by shifting overweight’s incidence [6,15,16]. The older generation (aged over 60 years), are specifically concerned by these transitional effects.
According to the annual reports of the National Program “Taking Care of Diabetic and Hypertensive patients (NPTCDH, Direction régionale des Unités des Soins et de Santé de Base, office of Douz, Ministère de la Santé Publique, Tunisia), averages of the latest three years (2010- 2012) of the prevalence of Diabetes (of all kinds), hypertension, and their association, are respectively of 2.23 ±0.31 %, 5.25 ±0.94 % and 1.96±0.25 %. Their prevalence was estimated as the number of diagnosed patients among all subjects visiting the village’s Hospital and Units of Care and Basic Health for different medications, each year. The NPTCDH report did not show significant evolving of these diseases incidence, while there was a slight increase (from 7.09 % in 2010 to 11.66 % in 2012) of the prevalence of the newly depicted association between diabetes and hypertension (Figure 2).
Diet history
The customary nutritional allowance of the population is practically composed of vegetal products (cereals, grains, legumes and fruits), in association to milk derivatives and eggs [15,17]. As localized far from the sea, fish intake is occasional. However, small quantities of dried juvenile sardine were sometimes added to some traditional meals. Meat consumption is also less frequent, and recently it is always replaced by poultry. Traditionally, sheep and goat meats are commonly consumed, after a religious feast, in form of sausage. Because of religion and habits, alcoholic drinks and wine’s beverage; and cigarette smoking are less frequent, and are obviously a masculine behavior. Habitually, semolina based products (couscous, macaroni or bread) constitute the main component of the principal meal of the population. Couscous, the most ancient known nutrient in the region (238 BJC) [www.Wikipedia.com], is usually prepared using several additives such as legumes (potato, tomato, squash, onion, garlic, carrot, beet, green peeper, etc), grains (bean, chick-pea, lentil, fenugreek, etc.), vegetal oil (olive oil), and many spices. Unless recommended for some people, salt is usually added to each meal. Exceptionally, in summer days, a salad made of fresh onion, green- peeper, tomato and cucumber is frequently consumed; while it is not a routine.
Diet and biological parameters assessment
The study was performed using data registered by the Red Crescent (Cross) Association of Douz, in Marsh 2012. All biological and anthropometric measurements (blood pressure, blood sugar concentration and body weight index) were recorded by an experimented team of the association. The arterial blood pressure measurement was twice effectuated using an armband centimeter, at sitting position and after, at minimum, 15 minutes of quiescence. If the two recorded values differed by more than 10 %, a third measurement was performed, and the mean of the two ones, with closer values was considered in the study. Blood sugar was quantified using an automated apparatus. Subjects with systolic pressure over than 140 mmHg or diastolic pressure over than 90 mmHg were considered as hypertensive. Overweight was estimated as a body mass index (BMI) over than 25 kg/m2.
The diet assessment was based on a qualitative foodfrequency questionnaire. Participants were asked how many they consumed a specific type of food and beverage, each week. The medical history of each person (diabetes mellitus type 2, familial history of diabetes and cardiovascular diseases, if any occurred before) was also noted. Pregnant women were excluded from the study. Among 875 volunteers, only 341 persons have a registered blood sugar concentration; and 276 ones entirely answered the diet questionnaire. Among 875 subjects 23.54% were hypertensive (PS ≥ 140 mmHg and/ or PD ≥ 90 mmHg).
Statistical analysis
In accordance to our designated objective, the studied sample of population was grouped into different classes based on age, gender and the week- frequency of semolina products (couscous and, or macaroni) consumption. The obtained results were analyzed by multivariate tests and chi square one. Simple Spearman correlations were also checked (SPSS program for Windows 11).
ResultsDiet Characteristics
The primary list of nutrients comprised 54 different kinds of foods and beverages. The Spearman linear correlation of the studied health indicators to the fixed foods and beverages frequency consumption did not show any relevant variability, except for soft beverages and pastry which are avoided by diabetic patients, as recommended by their physicians. However, as shown in table 2, the percent of people consuming more than 4 portions of semolina products (excluding bread, which is much common) was remarkably elevated (69% of the total sample of population). A slight gender related difference was observed in such index, with rates ranging from 68 % to 93 % (average of 75 %) and 46 % to 70 % (average of 56 %) in men and women, respectively. Furthermore, subjects consuming more than 4 times a week olive oil and poultry represent 76.86 % and 65.22 % from all the included participants. In the other hand, only 8.7 % ones ate meat twice a week. Grains are usually consumed in few quantities as additives to the principal meal (couscous and macaroni). The percent of people eating grains 4/7 days or more is of 30.46 %, 36.59 %, 43.12 %, and 57.25 % respectively for fenugreek, lentil, bean, and pea- chicken. Interestingly, salt is daily used in preparing foods (73.55 % of the studied sample of population).Also, the percent of peoples abundantly (more than 5 times per week) consuming vegetables (potatoes, tomatoes, carrot, squash, peeper, bean, onion) ranged from 51 % to 75 % of the studied sample. Green tea is daily consumed by 56.16 % of total number of participant, and preferentially by peoples of the third age (68.85 %).
Prevalence of Adult-Hypertension
The statistical analysis showed that both systolic and
diastolic pressures were significantly elevated in elders
(over 60 years old) for both genders (p ≤ 0.01) (Table 1).
A sex related difference in these parameters was also
observed in A3 (40 Prevalence of Diabetes Mellitus Type 2 Chi square test did not show any significant differences
in the blood sugar levels between D1 and D2 groups
(Table 1). However, the incidence of diabetes was
importantly elevated in elder women (forth age, A4), than
younger ones (p= 0.0001, 0.004, and 0.031, in comparison
to A1, A2 and A3, respectively.). Sex related difference
was also observed in the overall occurrence of diabetes
(18.29% in women, and 15.98% in men). Irrespectively,
the familial diabetes rate was much greater in women in
A1 (58.82%) than that in A3 group (31.03%). This
difference was also notified between A2 and A4 in men
(20.78% and 11.11%, respectively) (Table2). The
percentage of diabetic men was significantly higher in D2
than in D1 (p <0.05), with a noticeable leveling up at A3
age-class. This observation goes along with the rates of
persons having familial diabetes’ history (Table 3). Overweight Prevalence The calculated body mass index slightly increased
within age, which reflects the elevated rate of
overweighed people with drastic values observed in
women aged from 40 to 60 years (72.41%) and in elder
men (62.22%) (Table1). Rationally, this rate was much
greater in A3 and A4 than A2 and A1, respectively (p=
0.006 and 0.02, respectively) in women. The overweight
incidence of the total sample of population was greater in
men (56.1%) than in women (37.1%) (Table 2).
Unexpectedly, the incidence of BMI over than 25 kg/m2,
in women, was much elevated in D1 (50%) than in D2
(28.57%). Particularly the third aged women in D1
presented the greatest value of overweight incidence
(84.21%) (Table 3). Non- Dietetic Factors The physical effort (moderate to hard) and cigarette
smoking are significantly different between men and
women. As expected, tabagism is a mostly a masculine
behavior, particularly at the age ranging from 20 and 40
years (50%). Also, the same age class (A2) spends much
energy, and shows the greatest percentage of moderate to
hard physical activity (63.04%) (Table 1). Obesity, adult-hypertension and diabetes constitute
worldwide health and socio-economic problems. Their
etiology comprises several factors that complicate their
therapy [2,5,18-20]. Recently, great body of knowledge
approved the improving role of optimized dietaries in
preventing and managing these diseases; and relevant
dietetic recommendations are given by the WHO and
many other health organizations [13,20]. Dansinger et al.
reported that each popular dietary has specificities to
prevent or not a certain diseases [21]. In this study, we
evaluated the possible correlations of a specific popular
food (semolina products) intake to these diseases
prevalence, on a sample of a local population. As
presumed, the number of subjects consuming macaroni
and/ or couscous more than seven times a week
surpasses 69 % of the overall studied sample of
population. We found that the systolic and diastolic pressures
correlated to (moderate to intense) physical activity and
cigarette smoking, which are particularly masculine
behaviors. An adequate physical activity augmentation is
known to prevent these diseases development and
ameliorates their therapy [18,22]. In contrary, cigarette
smoking seems to enhance diseases development [7]. In
our studied group of subjects, tabagism negatively
correlates to diabetes and hypertension incidence; and its
influence is suggested to be masked by the important
muscles activity in people aged less than forty years. Both,
overweight and hypertension incidence increased within
aging and reached top levels at the third and fourth age
respectively in women and men. Diabetes mellitus
prevalence was particularly elevated in women and men,
respectively aged over 60 years and between 40 and 60
years. Seemingly, these results could be explained by the
age- quiescence factor [16,23]. Substantial intervening is,
also, attributable to diabetes familial history, and the
detrimental genetic effects [5]. As expected, the
prevalence of hypertension and diabetes mellitus type 2
increased when people weekly consumed more than
seven portions of semolina products. Within sex and age
segregations, it is observed that both high blood pressure
and diabetes frequently occurred in men at the third age
in association to family diabetes’ history. While in women,
only diabetes incidence was elevated at 20 to 40 years
old. At this age, women’s consumption of couscous and /
or macaroni is at the highest level. Apparently, the
enrichment of these two meals in carbohydrates (166 g of
couscous and 148 g of macaroni brings 38 and 42 g of
total sugar, respectively [24]; in addition to additives
(potatoes, squash, beet and carrot) contributions, affects
their metabolic turn-over and participates into obesity
and diabetes physiopathology [25-27]. Also, they do contain important amounts of minerals,
especially salt (73% of participants frequently add salt to
their meals) that induces renal and hemodynamic
systems misbalance [28,29]. Irrespectively, our results
showed that the group of women with reduced- diet in
semolina presented higher prevalence of overweight with
a noticeable value at the third age. Perhaps, such
unexpected observation could be of obesity- related
genetic origin [6], or other specific factors such as the
post- menopause status [30]. In this study, it is suggested
that frequently consuming specific popular foods (herein,
semolina derivatives) could be a risk factor of diabetes,
hypertension and obesity. According to cocking habits
and other foods (adding grains and vegetables) intake
might interfere with the presumed effects. Herein, it
should be noted that many of these nutritional additives
are suggested for healing and preventing the studied
diseases. For example, fenugreek, vegetables and spices
intake may bring supplementary vitamins, polyphenols,
flavonoids and carotenes that play pivotal roles in
reactive oxygen species scavenging and modulating
immune responses. Thus, their ameliorate wound healing
and prevention against diseases [31-33]. In raison of the
lower sample size of the studied group, our results remain
speculative. Lifestyle especially the nutritional habits are involved
in several common diseases (diabetes, blood
hypertension and obesity).Several allowances and
nutritional guidance showed great importance in
preventing diseases; but their generalization remains
difficult in raison of populations’ divergences. Here in, it is
suggested that the frequent consumption of particular.
Traditional foods might enhance some chronic diseases
development. Therefore, it is conceived that loco-regional
societies traditions and nutritional habits should be
considered to develop an accurate healthy- diet. The
requirement of a large scale analysis of such item will
better draw the influence of specific food intakes on the
public health statute. The authors greatly thank the Red Crescent Association
of Douz-Tunisia, and the Regional Direction of Care and
Basic Health of Douz (Ministry of Public Health of
Tunisia), for their collaboration.
Figure 1: Map representing the site of the study.
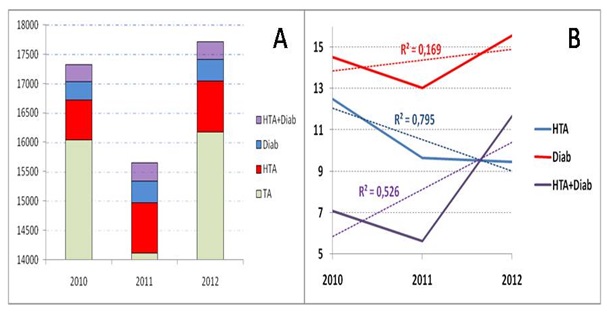
Figure 2: The panel A shows the total number (TA) of hospitalized persons, and which of patients with diabetes (Diab), hypertension (HTA), and their association (Diab + HTA) from 2010 to 2012. The panel B shows the evolution of the rate (%) of newly depicted diabetes, hypertension, or their association; from 210 to 2012.(Data generously offered by the Regional Administration of Basic Health – Office of Douz; Ministry of the Public Health of Tunisia).
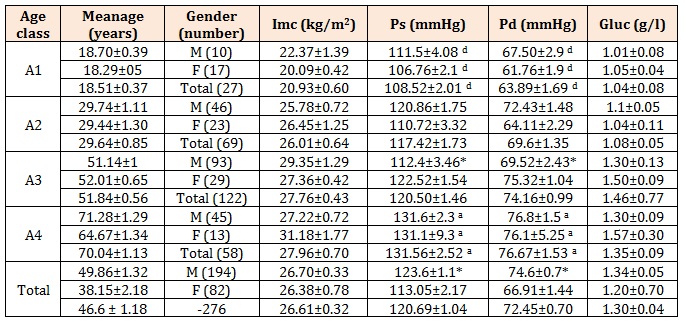
Table 1: Anthropometric and biological parameters of the studied sample of population.
a, b, c, and d represent the significant differences at 0.05 in comparison to A1, A2, A3, and A4 age- groups. Sex related difference (at 0.05) is highlighted by (*).
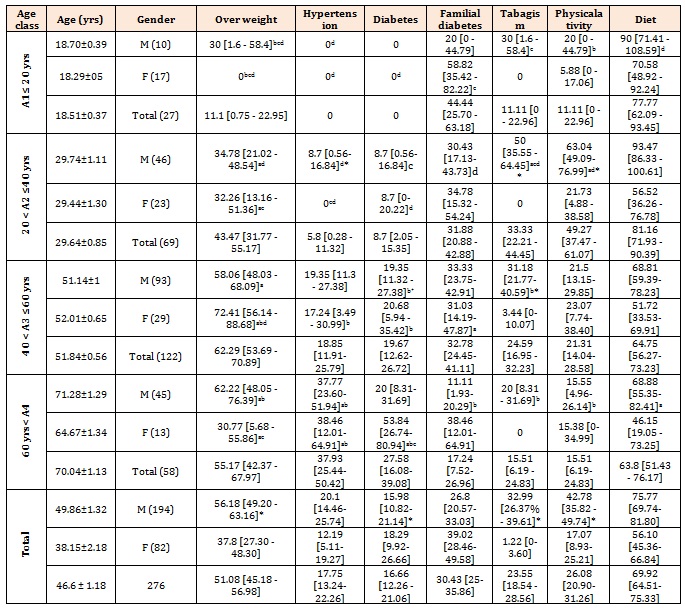
Table 2: The distribution of rates of overweight, hypertension, diabetes, familial diabetes, tabagism, moderate to hard physical activity and Diet (eating 4 or more portions of cousous and / or macaroni per week), within age and gender, of 276 participants.
a, b, c, and d represent the significant differences at 0.05 in comparison to A1, A2, A3, and A4 age- groups. Sex related difference (at 0.05) is highlighted by (*).
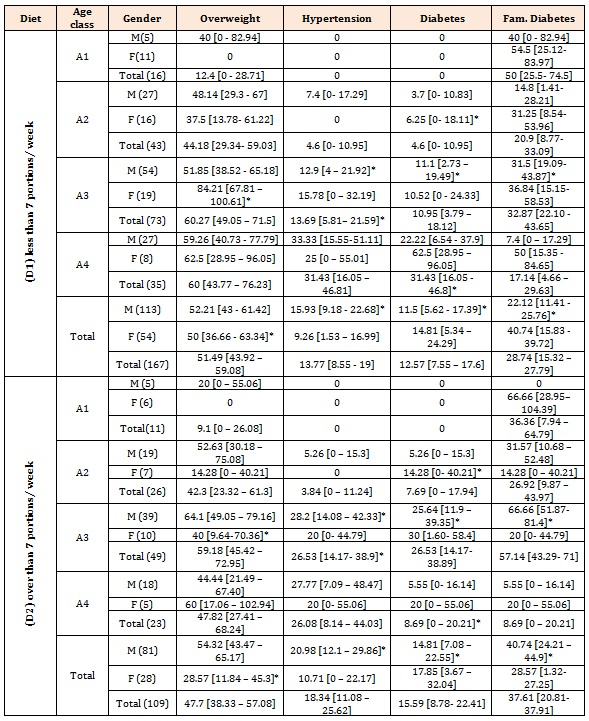
Table 3: the distribution of the prevalence of overweight, hypertension, diabetes mellitus type 2, and familial diabetes within the frequency of foods (couscous and / or macaroni) consumption, age and gender. (*) shows significant differences between D1 and D2.





Chat with us on WhatsApp