
Citation: Eva Menino G et al. Validation of Diabetes Knowledge Questionnaire (DKQ) in the Portuguese Population. Diabetes Obes Int J 2017, 2(S1): 000S1-002.
*Corresponding author: Eva GM, PhD Nursing, MSc Specialist Community Public Health Nursing, ,Filiation: Portuguese Red Cross Health School, Health Research Unit of Polytechnic Institute of Leiria (IPL), Portugal, Email: emenino@esscvp.eu
Introduction: Diabetes is a chronic disease that is assuming worrying proportions considering the epidemiological data and the clearly negative impact which causes in our societies. So, is necessary to take steps towards improving the quality of services, is essential to know the reality, identifying the points where it is necessary to redefine strategies. Being the knowledge that users with diabetes have about their disease an essential outcome for proper self-care and disease control, it is justified to be assessed the level of knowledge of this population and such that there are calibrated instruments and with quality for this purpose.
Objective: To determine the psychometric characteristics of DKQ-24 scale (Diabetes Knowledge Questionnaire-24) for the sample in question; Knowing the level of knowledge of users with diabetes followed by a Health Centers grouping in Portugal. Methods: Based on the question 'What knowledge have the users with diabetes about the disease? "we developed two studies: an initial one of revalidation of the data collection instrument (a); and a second descriptive study (b) about the level of knowledge of users with diabetes on the various areas of relevance associated with self-management of the disease.To conduct the research work we applied a questionnaire interview which consists of a part related to sociodemographic and clinical data and a second part consisting of the DKQ-24 instrument that evaluates knowledge about diabetes and that was validated by Bastos (2004) to Portugal and revalidated by us for the sample under study (292 users with diabetes followed in basic health care).
Results: DKQ-24 scale has a total value of 0.863, showing a good internal consistency. Most users missed the answers about the disease causality and hypoglycemia signs and revealed ignorance about where insulin is produced, monitorization of blood glucose levels, the effect of exercise in controlling diabetes and hyperglycemia signals.
Conclusion: We concluded that is urgent the investment in the improvement of relevant results for the control of diabetes, particularly in the knowledge that the user has about his disease, as these are the basis for self-management that assumes a central role in this chronic disease.
Keywords: Diabetes Mellitus; Knowledge; Validation studies
Diabetes Mellitus, is significant among the chronic diseases, in accordance with the International Diabetes Federation (IDF) (2012) [1] reaches over 371 million people worldwide, is considered nowadays an epidemic. Half of those who die with diabetes are younger than 60 years and the combination of complications, deaths and loss of income make the disease a real threat not only for patients but also for the economies of the countries themselves.
In Portugal, although the health centers develop programs about the education of users with diabetes is recognized that the evaluation culture is still incipient [2], there is a need for further studies to evaluate the implemented educational programs [3]. One can question which indicators are included in this evaluation of programs implemented in the diabetes area, to be able to be monitored its effectiveness.
Research has shown that knowledge is a central result in the control of diabetes. Investigations reveal that knowledge about medications, diet, physical activity, blood glucose monitoring at home, care for the feet and on the necessary modifications, it is essential to manage diabetes independently [4]. Knowledge about diabetes is a key component to diabetes control in the context of education for self-management; in addition, higher level of knowledge about diabetes has been associated with a higher level of adherence to taking medication, greater longevity, and higher adherence to follow-up appointments with various health professionals [5] and it has been associated with improvements in HbA1c [6].
Although isolated knowledge have been insufficient to achieve changes in HbA1c, there is emerging evidence from existing research that indicates that the behavioural and clinical outcomes remain unchanged unless there is knowledge combined with the understanding of the need for change, about what to change and how to change. Therefore, knowledge is considered a primary outcome in the diabetes area [7]. Whatever is the cause of diabetes epidemic, the population level solution is to change the life styles [8], to undertake this change in the first instance one must be equipped with the necessary knowledge.
The knowledge gained by the user with diabetes is considered an outcome associated with nursing care, being a categorised result [9]: "Knowledge: diabetes control" is defined as the "Achieved range of understanding the diabetes, its treatment and prevention complications ", assumed as a sensitive result to nursing care.
Towards the measurement of the user with diabetes knowledge, was pondered the use of existing instruments or new ones. In fact, if we use an instrument already existing, we contribute to the knowledge of its properties and value and we can compare and contrast results to obtain instruments increasingly reliable and valid [10].
With the dissemination of transnational and crosscultural research, the need to adapt measuring instruments for use in other languages than the original appeared associated. The cross-cultural adaptation of questionnaires for use in another country, culture and / or language requires specific methodologies in order to obtain equivalence between the original source and the new version [11]. Although the measuring instruments have been translated and adapted culturally, this methodological validation study refers to a nonprobabilistic sampling and is more reliable to make these instruments revalidation [11]. For this reason, we revalidated DKQ, since although they have previously been subject to validation for a population with similar characteristics and in Portugal, these results cannot be considered generalizable, given the characteristics of the studies.
The DKQ instrument originally created with 60 items (extended version) and in English, was developed and validated for the Spanish and English language in a reduced version of 24 items [12], from which was made the translation and validation for Portuguese [13]. From the Portuguese version was made the revalidation presented in this study.
This scale seeks to identify the knowledge that users with diabetes have about the disease, having been developed in order to include the content recommended by guidelines in education to the patient with diabetes [12].
The questionnaire covers, in this sense, questions related to general knowledge about diabetes and relevant aspects of the disease, as the cause production of insulin and hyperglycemia, duration of the disease and tendency to heredity, aspects related to the therapeutic regimen and its effects on glycemic control misconceptions, consequences and symptoms of hypoand hyperglycemia [12].
The methodological study described, has as aim to ensure the necessary conditions for the validity and reliability of the instrument, intending to retain the Portuguese version of the instrument Diabetes Knowledge Questionnaire - 24 (DKQ) to measure the knowledge, testing its psychometric properties for users with type 2. After guaranteed the conditions of applicability of applicability of the instrument, it goes to the descriptive study that aims to identify the level of knowledge of users with diabetes about the disease.
MethodAfter authorization n°32543 of the Governing Board of the Centre's Regional Health Administration for the study and approval of the Ethics Committee for Health and the direct contact with the heads of each data collection place, participation was requested by informed consent for users with type 2 diabetes who had diabetes appointments with doctor and nurse in this place at the time of data collection. It was mentioned that all information would be confidential and that could give up when they wished, providing all the attention regarding the clarification of doubts and questions, according to the Helsinki Declaration.
The DKQ was applied by interview to users with type 2 diabetes because significant portions of the population have difficulties in completing and reading documents of this nature. Thus, in order to respect the principle of consistency during data collection, to reach an adequate methodological rigor we mobilized this data collection method for all participants. This option is suitable designating up, in this case, the data collection method questionnaire interview [10].
The statistical treatment of the data was performed using the SPSS (Statistical Package for Social Sciences), version 21.0. We used techniques of descriptive analysis, namely: measures of central tendency and variability measures of dispersion for the descriptive study.
To validate the DKQ we followed what was proposed by Bastos (2004) [13], author of the Portuguese validation, to determine the psychometric characteristics.
In order to be able to analyse the fidelity through internal consistency, was determined the alpha coefficient of Cronbach which is the most advised indicator to assess the internal consistency of measure instruments [15].
In addition to this indicator, we proceeded to determine the mean of the correlations between all the test items, which corresponds to the homogeneity of the set of items [16]. Were eliminated those items whose correlation coefficient was less than 0.20 as proposed by Streiner and Norman (2008) [17].
As proposed by the author of validation for Portuguese, the questionnaire was coded in right answers (1), wrong (0) and do not know (2). Subsequently, and for the presentation and analysis of the results of the sample, modified in a dichotomous scale (1 and 0) to distinguish between the presence of knowledge and presence of unknowns and misconceptions, being transformed into one of the answers that match the right answer for the desired variable (eg knowledge: right answer = 1) and the rest to 0 (for wrong answers or ignorance).
The population was constituted by users with diabetes type 2 followed by nursing consultation and monitoring of diabetes in health centers Grouping (ACES) in primary health care in the period from November 2013 to April 2014. The sampling technique used was intentional and acidental16 considering the probabilistic accessibility of respondents in the reporting period and verified the following inclusion criteria: being diagnosed with diabetes type 2 mellitus; being accompanied in nursing consultations in the diabetes area; have over 18 years; speak and understand Portuguese; have cognitive ability to answer the questionnaire (assessed by nurses accompanying users); consent voluntarily participate in the study and sign the respective informed consent.
ResultsBefore the presentation of the psychometric validation of the results, we present some characterising sample data and of the descriptive study about the knowledge of the users surveyed (Table 1).
The sample consisted of 292 users aged 26 to 88 years (mean = 68.0, SD = 9.7), mostly men (50.5%), most users were married (74 3%), with low education levels (84% 4 years of schooling or less), most retirees / pensioners (73.4%).
Relatively to the clinical situation, users have the disease diabetes type 2 mellitus for an average of 9.7 years and most take oral antidiabetics (92.7%), 2.4% insulin and 2.9% both treatments. Most of them do not report complications related to diabetes (74.2%) nor admissions related to diabetes (94.2%). Most of them report have no comorbidities (55.2%)
a. Regarding the results of the methodological study revalidation of the data collection instrument, following the methodology proposed by the author of validation for Portuguese, (Table 2) presents the results of the scale fidelity of the study. Presents the corrected correlations of each item with the total scale, ranging between 0.232 and 0.556, revealing appropriate values of correlation [15].
The fidelity, we obtained a total amount of α (0.863), revealing a good internal consistency [15]. The total values without the item also proved to be suitable, since none of α values obtained after removal item was superior the initial total α, so there was no removal of any item.
Considering the performed statistical validation, following the methodology of the author about the validation for the Portuguese population, remained the instrument initially presented. After assessed its psychometric characteristics, the instrument meets the conditions necessary for its implementation in order to assess the knowledge that users with diabetes have about the disease.
b. With regard to the study on the knowledge of users with diabetes, in (Table 3) are highlighted the results according to the response to each item in which we can find most of the respondents .
Considering the data in Table 3 about the causality of diabetes, the results indicate that the majority of users shows Wrong answer in the item that refers to sugar and sweet foods as a cause of diabetes (86.6%); On the other hand, most of the users has correct knowledge in the item that presents the causality related to the lack or insulin resistance. In the item that links the causality of the disease to the difficulty of the kidneys in keeping the urine without sugar, most of the users revealed ignorance.
Regarding the production of insulin, the majority (43.1%) do not known whether this is produced by the kidneys, as do not known whether the best way to evaluate diabetes is doing urine tests (41%); however, the majority (73%) know that diabetes can damage the kidneys. Most users that make up the sample is unaware or has wrong knowledge about the signs of hypo- and hyperglycemia. The consequences of diabetes is an area where most respondents has right answers on the evaluated items.In the item about the knowledge of the heritability of the disease, most have correct answer. Most users know the existence of two main types of diabetes and know the prognosis of the disease about the cure. In the aspects related to the management of the therapeutic regimen and glycemic control, most of the users that make up the sample, knows about the suitability of the value of 210mg / dl fasting glucose, knows the relationship between food intake and the change in blood glucose and knows the degree of relative importance and effect of diet, exercise and medication on glycemic control. About the selfmanagement of associated disease and care, most users had correct answers to the items assessed, particularly regarding the use of elastic stockings, as is a diabetic diet, the importance of the way the food is prepared, the need of special care when they cut the nails; however, most of them do not know how to perform the treatment of a wound.
Results, Discussion and ConclusionIt is relevant to know the sociodemographic characteristics of users that make up the sample because in the case of users with diabetes, they can influence several results, including knowledge related to diabetes, the ability to adhere to the recommended medication, exercise, dietary recommendations and other therapeutic options [13].
a. The DKQ-24 kept the structure of the Portuguese version of Bastos (2004) [13], have been evaluated through the internal consistency of the value of α as the said author and the authors of the reduced version in which was applied [13] Was not carried out the factor analysis considering the procedures adopted by the authors of the referenced validations, taking into account the comparability of results.
We obtained a total amount of 0.863 α, revealing being reliable, with a good internal consistency [15] value relatively higher than that found by Bastos (2004) [13], of 0.67; also, the identified correlation values of the items were suitable (all greater than 0.20), while 10 of the total of 24 items in the study of the identified items correlation value was less than 0.2, showing that for this sample the correlation between these items and the total scale is very low [15], this fact may be associated with the relatively small sample size (n = 103).
The identified studies that performed the validation of DKQ, the one of Chilton et al. (2006) [18] was in which was obtained a higher value of α (0.87), although this study presents methodological limitations to the size of the sample (n = 40) and has been used a version with only 17 items, because of that the authors considered that some items should not appear to be evaluated by another scale applied in this study. The study by Garcia (2008) [19] also presents a reasonable value of α (0.74), and once again, results induce some reservations by the sample size (n = 87).
In the original version of the short version of Garcia et al. (2001) [12] was obtained a value of α = 0.78, showing an internal reasonable/ high consistency, revealing a value of the scale fidelity considering also the sample size of 492 users. Also here, the correlation values of all items were above 0.2 and mostly higher than 0.25.
Compared to the figures presented in the original version and also obtained in this study, it can be concluded that the scale is reliable and an appropriate tool to evaluate the knowledge of users with diabetes. The DKQ-24 evaluates the knowledge about diabetes and is verified that it is valid, consisting of 24 items grouped in a single dimension.
b. As for the descriptive study about the knowledge that users with diabetes have about the disease, the item where was obtained a higher number of correct answers (84.5%) was on the issue "a blood sugar level of 210, in a Test fasting, is very high, "as in the study of Hu et al. (2013) [5]that also resorted to the same scale for assessing knowledge in a population of Chinese, it was also this item with a higher percentage of correct answers (87.6%). Then the item that had the best quote was "Diabetics should take special care when cutting the nails of the toes" with 83.8% of correct answers and in third place the item "The way you prepare the food is as important as the food you eat "(83%). The item " cuts and wounds heal more slowly in diabetics" was placed second in the study by Hu et al. (2013) [5] with 83.8% of correct answers and in this study was also well positioned in fourth place with 81.7% of correct answers, a very close value of this study. The sample of Bastos study (2004) [13] also had higher percentages of correct answers in these items, ranging between 83.5% and 92.2%.
The items on which it has identified a smaller number of correct answers were "Eating too much sugar and sweet foods is a cause of Diabetes" (7.9% of correct answers), followed by the item "Diabetes is caused by the kidneys' difficulty in keeping the urine without sugar."(20% correct answers) and" Shivering and sweating are signs of high blood sugar "(24.6%). Interestingly, the study of Bastos (2004) [13] these were also the three items with the lowest quote and in the same order, which is justified since people are very close culturally and have very similar characteristics since this study was also performed on Portugal, although in the northern region of the country. In the study of Hu et al. (2013) [5] the item "In the study by Hu et al. (2013) [5] the item "Diabetes is caused by the kidneys' difficulty in keeping the urine without sugar." was also those in which was obtained a lower percentage of correct answers (the third lowest), but with higher percentages (30, 2%) than those identified in the present study."
It should be noted that the sample users know the consequences of diabetes. Most of people responded correctly to the questions "Diabetes can damage the kidneys," "Diabetes can cause decreased sensitivity of the hands, fingers and feet," "Cuts and wounds heal more slowly in diabetics," "Diabetes often causes poor circulation".
In this study are identified, as reported in the study of Hu et al. (2013) [5], deficits at the level of knowledge of users about diabetes.
The results indicate that the majority of users in the sample, shows deficit of knowledge about the causes of the disease and the signs of hypo- and hyperglycemia, very relevant aspects towards self-management required for proper control of diabetes.
Hu et al. (2013) [5] identified also lack of knowledge in more than half of the users about the causes of diabetes and about the physiology of diabetes (evaluated through the item "The kidneys produce insulin"), on this last item, also the sample of this study revealed unsatisfactory results (only 39.7% of users responded correctly).
Low knowledge levels may be associated with lower literacy levels associated with older ages identified in users with diabetes type 2 [5,18]. Nevertheless, it is interesting and it follows the need to understand the fact that in the 3 studies analyzed the results are almost overlapping, although the realities are culturally distant, especially between China and Portugal.
It is recognized that few users have been helped to manage or take responsibility for their treatment [20] and there is no evidence about the "best" program or approach, but programs incorporating behavioral and psychosocial strategies demonstrate best results [21]. In fact, specific training for professionals in this area is crucial for an effective education [22].
Users, in general, know the consequences of their disease status, however, have difficulty identifying key aspects for preventing these complications (including hypo and hyperglycemia management, treat wounds, the effect of exercise on blood glucose, food choices), a situation which refers to the need to develop studies on effective educational strategies for this population and to implement programs structured in order to minimize the critical gaps in users knowledge [23].
Hu et al. (2013) [5] additionally suggest that care providers can address this situation through educational programs appropriate to the age and literacy levels of users with diabetes through family involvement. They also suggest changing the focus to the benefits of behavioral change rather than the negative consequences of inappropriate behavior.
The limitations of this study indicate that the results obtained in the study require support through further studies with larger samples and characteristics of randomness, do not exist for this study, conditions for generalization.
For continuity of this study we suggest the application of the measuring instrument in other geographical and cultural contexts, since this study was limited to a Health Centers grouping, in order to know and characterize the results with regard to knowledge in a more full and less contextual way, with integration of other realities and comparing the data obtained with even more valid and reliable instruments.
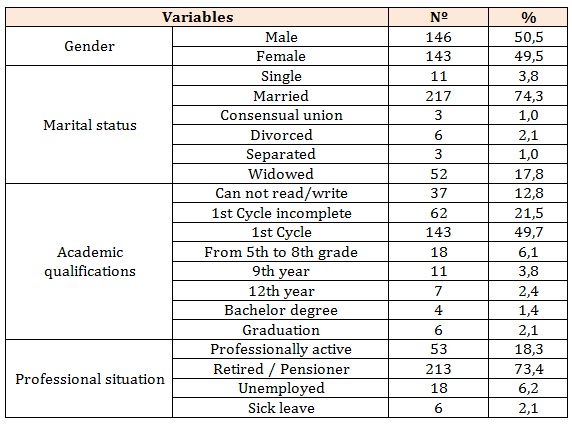
Table 1: Sample distribution regarding sociodemographic characteristics.
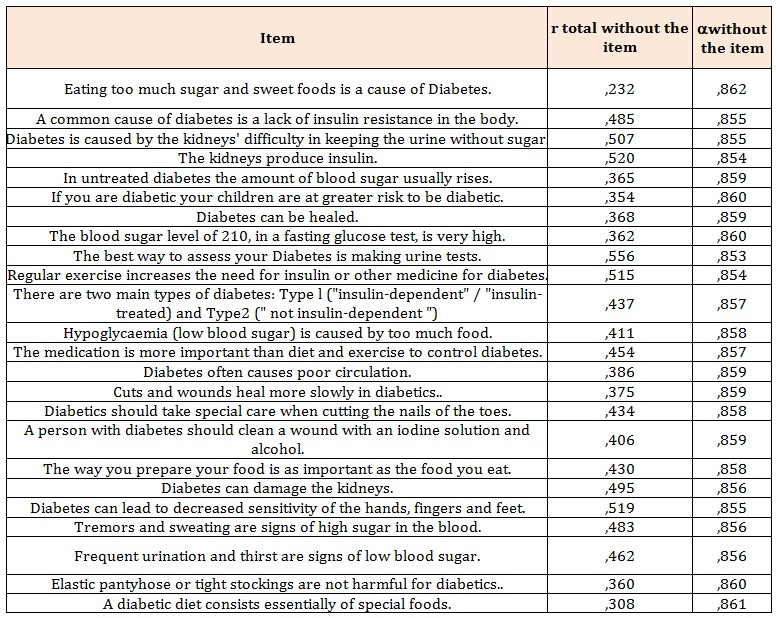
Table 2: Pearson correlation and Cronbach's alpha of the items with the total without the item from the scale DKQ.
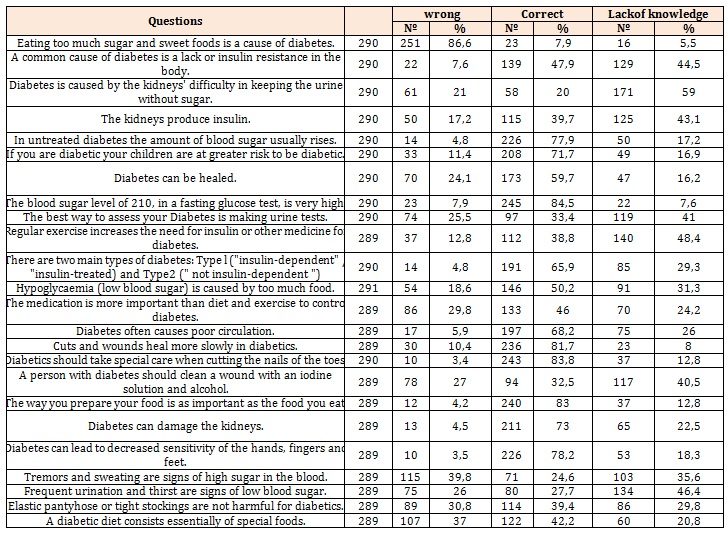
Table 3: Distribution of wrong answers, correct and lack of knowledge




