
Citation: Baptista MJ, et al. Elderly Suicide: A 5-Year Forensic Autopsy Analysis in the North of Portugal. Int J Forens Sci 2016, 1(1): 000106.
*Corresponding author: Maria Joao Baptista, Faculty of Medicine of the University of Porto, Portugal, Tel: +351 225 513 600; Email: mjpbaptista@hotmail.com
Elderly suicide is a well known worldwide health problem, and suicides rates, in this age range, vary considerably. However, there are still few studies published based on information collected from forensic autopsy. The aim of our study was to, through forensic autopsy analysis, investigate the sociodemographic characteristics, mental and physical health status, as well as the suicide methods of the elderly population from the North of Portugal, emphasizing the role of Forensic Medicine in suicide prevention. Between January 2010 and December 2014, a total of 11 642 forensic autopsies were performed at the North Branch of the Portuguese National Institute of Legal Medicine and Forensic Sciences, 449cases corresponding to suicides of elderly people (65 years or older). The gender ratio male/female was 3:1. Hanging was the most frequent suicide method (48.6%) regardless gender or residence area. A positive psychiatric history was present in 71.2% of the elderly, being this group more likely to commit suicide at younger ages (p=0.000).The results of this study pointed the highly lethal nature of suicidal behavior in elderly and the intensity of their intent to die. Therefore, these data can constitute an important guide to have in account to establish strategies for suicide prevention in elderly population, proving that the contribution of Forensic Medicine in suicide prevention is important and necessary, and it shouldn’t be neglected, considering the eminently social character of this medical discipline.
Keywords: Suicide; Elderly; Prevention; Epidemiology; Forensic autopsy
Elderly Suicide is a worldwide public health problem. According to the World Health Organization, adults aged 70 years or older have the highest suicide rates in the majority of regions, independently on the gender [1]. Suicide in this particular population is a challenge to clinicians because older adults are less likely to report depressive symptoms and suicidal thoughts; in counterpart, they are more likely to use highly lethal methods and to succeed on a first attempt [2]. In the United States of America, although older adults attempt suicide less often than younger groups, they have a higher consummation rate. It’s estimated that 1 in every 4 attempts leads to fatal outcome in the adults aged 65 or older [3]. However, suicides are preventable. The contributions of Forensic Medicine can be part of the suicide prevention equation, reporting the circumstances of the death (method, location, time of the year) and also the victims’ features (sociodemographic, mental and physical health), therefore contributing to the understanding of suicidal behavior, which is essential to implement suicide prevention strategies. Policies to restrict suicide manners are an important prevention strategy, like, for example, restriction of firearm ownership licensing. In many countries, including Australia, Canada, New Zealand, and the United Kingdom, this policy has been associated with a reduction in rates of firearm associated suicides [1]. Suicide prevention is part of “The Mental Health Action Plan” of the World Health Organization, with the goal of reducing the suicide rate by 10% by 2020 [1]. Portugal is a country with a high percentage of elderly population, accounting for 20.1% of total residents (n=10 401 100) [4]. In 2012, the suicide rate for adults aged 70 years or above, of both sexes, was 34.8 per 100 000 [1]. However, suicide in old people is a neglected topic of research, with only a few studies conducted in the Portuguese territory. The aim of our study was to, through forensic autopsy analysis; investigate the sociodemographic characteristics, mental and physical health status, as well as the suicide methods of the elderly population from the North of Portugal, emphasizing the role of Forensic Medicine in suicide prevention.
Materials and MethodsAmong a total of 11 642 forensic autopsies performed at the North Branch of the National Institute of Legal Medicine and Forensic Sciences (INMLCF, IP) of Portugal and its offices, between January 2010 and December 2014, this study reviewed data of 449 cases. Inclusion criteria included the medico legal etiology of death (suicide) and the age at time of death (65 years or older). The data collected to the analysis were the following:
- Sociodemographic information: age, gender, race, nationality, area of residence, marital status and residential status.
- Suicide behavior: year, month, day of the week, place of the suicide act, method (including some specific characteristics further described), suicide note, survival time (if any), toxicological analysis and its results.
- Physical and mental status: medical pathology (differentiated between chronic illness and malign disease, as chronic illness was a considered a non immediate life-threatening condition (i.e. arterial blood hypertension, or diabetes mellitus), psychiatric disorders, suicide ideation, suicide motivation and previous suicide attempts.
Suicide method was classified into: firearm shooting, running against a moving train, drowning, jumping from a high place, intoxication, hanging, sharp object, immolation, suffocation, and association of any of these methods. In cases of firearm related suicides, the type of firearm, number and location of wounds, the bullet pathway, short distance shot signs on the skin, and if relatives knew there was a firearm in the household, were studied. In the cases of drowning and jumping from a high place, the features of the location of the suicide act were evaluated, whereas in intoxication cases, the type and the manner of taking the substances were studied. In cases of hanging, the neck groove characteristics and the gear of the loop were analyzed, while in suicides using a sharp object the location and number of lesions were studied. The data was statistically processed through the IBM SPSS Statistics 20® program. Statistical analyses were made with one-way ANOVA and chi-square tests, considering results as significant when the value of p was inferior to 0.05. The present study was approved by the National Institute of Legal Medicine and Forensic Sciences (INMLCF, IP) investigation committee.
ResultsSociodemographic information
Between January 2010 and December 2014, a total of 11 642 forensic autopsies were performed at the North Branch of the INMLCF, IP, 449cases (3.86%) corresponding to suicides of elderly people (65 years or older). Among the cases of elderly suicide, 322 were males (71.7%), accounting for a gender ratio male/female of 3:1. Approximately half of the cases were from individuals aged between 65 and 74 years old (52.1%) (Table 1).
The vast majority of the victims were Caucasian (n=448) and of Portuguese nationality (n=447), living in the metropolitan area of Porto (39.0%) (Table 1). The marital status was registered in 427 cases, of which 259 were married (60.7%), 135 were widowers (31.6%), 16 (3.7%) were divorced and 17 (4.0%) were single. Analyzing the age at the time of death within the marital status (p=0.000), it was noted that more than half of the married victims (n=259) committed suicide in the age range of 65 and 74 years old (32.0% - “65-69 years”; 28.2% - “70-74 years”). However, it was from that age range on that the number of suicide cases among the widowed (n=175) started increasing (16.3% - “70-74 years” versus 20.0% - “75-79 years”; 25.9% - “80-84 years”). No significant statistical difference was found between males and females.
Suicidal behaviorIn the total of suicide cases reviewed, 68 of them took place in 2010 (15.1%), 80 in 2011 (17.8%), 102 in 2012 (22.7%), 99 in 2013 (22.0%) and 100 in 2014 (22.3%).
Considering the official statistics from the National Institute of Statistics (INE) of Portugal concerning the elderly population (≥65 years old) living in the North Region of Portugal, the lowest percentage of suicide was registered in 2011 (0.013%), while the highest occurred in 2012 (0.017%). Within the whole of suicide cases among every age, 2012 (n=263) registered the highest percentage of elderly suicides in all the 5 years (38.8%). During this period, September was the month with more events (n=48; 10.7%), while November was the month with fewer ones (n=27; 6.0%) (Graph 1). The distribution of elderly suicide cases through the days of the week was consistent, as shown in the graph 2.
In a total of 308 cases (missing values in 141 cases), it was noted that 249 victims lived accompanied (80.8%), from which 175 lived at their own houses (75.9%) and 42 were living at a relative’s house (18.4%). In 11 cases the victims were living at a care institution (i.e. nursing home). The suicide act was most frequently carried out at the victims’ home (81.6%), regularly (62.2%) in an attachment of the main house (Table 2).
The most recurrent suicide method used was hanging (48.6%), for both genders, while in males (n=322) the second method of choice was firearm shooting (18.9%), although there were no registered cases in females (p=0.000). Drowning (25.2%) and intoxication (14.2%) were, respectively, the second and third most common methods chosen by females (n=127) (p=0.000). Small territorial differences were registered (p=0.005), for example in Chaves (n=19) hanging and shooting were equal (42.1%) and in Viana do Castelo (n=38) hanging (36.8%) and drowning (34.2%) were similar. In firearmrelated suicides (n=61), the most used type of firearm was a handgun (63.0%), while long-barreled weapons were used in 37.0% of cases. No significant statistical difference was found between residence areas regarding the type of firearm. Most firearm related suicide victims presented only with one entrance wound at autopsy (93.4%), mostly in the head (87.7%) (Table 3).
The pathway taken by the bullet inside the body, in 25.6% of cases, had a direction from front to back, upwards and from right to left. A close range (contact) shot was noticed in 44 cases (72.1%). Most of the drowning suicide cases (n=54) took place at the victim’s home, like a swimming pool, a tank or a water well (61.0%) (Table 3). Among the suicides committed by jumping from high place (n=36), the majority (67.7%) happened again at the victims’ homes, whereas only a small percentage of elderly chose a bridge (19.4%) (Table 3). Pesticides were the favored toxic substance (68.1%) among intoxication cases (n=47), with the organophosphates class being more frequently used (48.4%) (Table 4).
Corrosive substances were used in a smaller percentage (19.1%), with chemical bases (62.5%) being the most frequent among them. Intoxication by prescription drugs and carbon monoxide poisoning accounted for 8.5% and 4.3% of cases, respectively. No significant statistical difference was found between the residence area and the type of substance used in intoxication cases. Victims chose the oral administration to commit suicide by intoxication in 93.3% of cases. Among the victims that used hanging method (n=218), 82.5% demonstrated, at autopsy, a single ligature abrasion extending upwards (97.3%), resting immediately above the thyroid cartilage prominence (87.3%) (Table 3). In 169 autopsies it was possible to have access to the ligature involved, and in 47.9% of them a nylon rope was used (Table 3). No significant statistical differences were found between males and females regarding the ligature material. From a total of 9 suicide cases using a sharp object, in 5 of them self-inflicted incised wounds in the neck were found at autopsy, while 4 presented stab wounds in thorax, 3 in the abdomen and 1 in an arm.
Most of the victims had no known survival time (83.5%). From those that received medical assistance, 50.8% survived less than 24 hours and 30.5% survived from 1 to a maximum of 7 days. When survival was analyzed within suicide method (p=0.000), it was noticed that intoxication suicide victims (n=45) were more likely to die at the hospital (68.9%), within 7 days (80%), along with victims that used a sharp object (n=9) to commit suicide (44.4%), surviving less than 24 hours (75%) at the hospital. The evaluation of blood alcohol concentration (BAC) at autopsy was carried out in 374 cases, being negative in 329 of them (88.0%). The higher and lower values found were 5.00 g/dL and 0.10 g/dL, respectively (Table 4).Regarding the relation between gender and suicide method, no significant statistical difference was registered. A blood analysis for prescription drugs was required in 314 (71.2%) autopsies. The most frequent class was the benzodiazepine class drug (52.4%), although just in a few cases they had toxic concentrations (3.2%) (Table 4). No significant statistical difference was found between suicide method or gender and prescription drugs detected. All of the 64 cases where illicit drug analysis was required were negative.
Physical and Mental StatusAmong the 312 suicide cases where the victims’ medical history was known, 81.7% of them had a known history of chronic disease, and 9.6% of malign illness. No significant statistical difference was found between medical history regarding age range. Psychiatric disorders were found in most of the cases, accounting for 71.2% of which this information was available (n=281). According to the information provided by the victims’ relatives, depression was the most referred psychiatric disorder (n=135). It was found that victims with a known history of psychiatric illness (n=200) were more likely to commit suicide at younger ages (35.0% in “65-69 years” and 30.5% in “70-74 years”) (p=0.000). Previous suicide ideation was reported by victim’s relatives in 133 cases (50.6%). A significant statistical difference was found between males and females (p=0.006), with females (n=75) being more likely to verbalize this suicide ideation to relatives or acquaintances (64.0% versus 45.2% males). In 298 cases, a presumed suicide motivation was reported by the relatives, the most frequent being a known psychiatric disorder (46.3%) (Table 5).
The statistical relation between age range and suicide motivation showed that victims with loss of autonomy or incurable diseases committed suicide at younger ages (almost 50% and 70% of cases, respectively, from 65 to 79 years old) (p=0.026). The data showed that females (n=86) were more likely to present a psychiatric illness as suicide motivation (68.6% versus 37.3% males), whereas male’s (n=212) motivations were related to any incurable disease (14.2 % versus 4.7% females), loss of autonomy (9.4% versus 1.2% females) or a recent relationship disruption (6.1% versus 1.2% females) (p=0.000). No significant statistical difference was found between marital or residential status regarding suicide motivation. In the 275 cases where victims’ relatives reported on previous suicide attempts, 37.8% had actually previously tried it. A significant difference was found between males and females (p=0.001), being males (n=194) more likely to not have a previous suicide attempt (68.6%) than females (n=81) (46.9%). Regarding the number of previous suicide attempts, 37 attempted once and 16 had two previous attempts (these last mostly through intoxication and non-fatal hanging).
DiscussionElderly suicide is a well known worldwide health problem, and suicides rates, in this age range, vary considerably. However, there are still few studies published based on information collected from forensic autopsy.
Sociodemographic informationPortugal has a high percentage of elderly population (20.1% of the total population) [4] and the suicide rate at this age range is 34.8 per 100 000 [1]. Data from this study revealed a male predominance, consistent with other publications [5-9]. The higher number of cases was observed in the age range between 65 and 74 years old, in accordance with Shields et al. [9] (48.3% 65-74 years), and in agreement with the mean age found by Paraschakis et al [8] (73.6 years). Contrarily to what was observed in study by Shah et al. [5], our data revealed a steady decrease in the number of suicides with increasing age range. Regarding the residual number of foreign individuals in this age group living in the north of Portugal, the vast majority of elderly victims had Portuguese nationality and lived in a metropolitan area (Porto), facing the decrement of population observed in the countryside, as a result of socio-economic and demographic changes, that have been more outstanding in the last decades [10]. The great majority of victims were married, which was also registered by Shelef et al. [7]. The analysis within age range showed that a minor percentage of widowed were more likely to commit suicide at an older age (>75years), as observed by Paraschakis et al. [8]. Contrarily to what would be expected, most victims were living with someone else in their own house. The reason for this was already explained by Fassberg et al. [11], who stated that living alone does not reflect lack of social relationships. Paraschakis et al [8]also registered a higher percentage of victims that lived accompanied (70.8%), also in accordance with our data.
Suicidal behaviorIn our study, the most cases of elderly suicide happened in the months of June, August and September, different to what Shields et al found in Kentucky, being the highest percentage of in May and July [9]. This could be due to the fact that studies were conducted in different socio-cultural contexts. Meanwhile, like Shields et al. [9], we noticed in our study that months like November and December had less suicide cases. This phenomenon may be explained by the fact people are more connected to others in this time of the year, because of the holidays. The distribution of cases throughout the days of the week was uniform; this could reflect the idea “all days are being the same” to elderly people, as most of them are retired and engaged in similar routines all week long.
In our study, as in other research works [7-9], the victims’ home was the location most commonly chosen to commit suicide. Frequency of suicide methods varies between studies, which may be related to socio-cultural context differences, and also to how easy older people can access a certain suicide method. Nevertheless, available literature highlights the predominance of highly lethal suicide methods in the elderly [12]. Shelef et al [7] in Israel and Sturgiss [13] in Australia appointed hanging as the preferred method to commit suicide in this age range, as observed in our study, while Paraschakis et al in Greece reported jumping from a high place as the most common method [8]. On the other hand, Shields et al assigns firearms as the most frequent suicide method in Kentucky [9].
In the present study, males were more likely than females to use firearms to commit suicide, corroborating that males usually use more lethal methods [14]. On the other hand, females were more likely to recur to intoxication, a phenomenon also observed by Shelef et al. [7] in Israel. When the suicide method was analyzed within area of residence, rural areas (e.g. Chaves) had a significant higher percentage of firearm suicide cases, which can be explained by its easy access, probably due to the common practice of hunting in these rural areas, so a large number of people own a firearm. In addition, Viana do Castelo, a coastal area, registered a higher significant percentage of drowning cases. Once again, it was found that an easier accessibility to a certain method is an essential determinant of risk to commit suicide. Handgun was the most used type of firearm, which can be due to the fact that is easier to purchase. Surprisingly, we did not found a significant difference between residence zones. It would be expected in rural areas where hunting is frequent that long-barreled guns would be more commonly used, but no statistical significance was found. The information on firearm ownership and if relatives of the victim knew about it, considered an important risk factor in literature [15,16], was unfortunately lacking in our study, due to poor registry of this data. This can emphasize the need for implementing more safety standards regarding storage of firearms and bullets, which could minimize the suicide risk in these cases. For future researches, it would be essential to register this type of information in the autopsy file during social interview with the victims’ relatives. Suicidal people try to reach for vital sites of the body when trying to kill themselves, like the head, mouth and over the heart [17]. Our results show that the head was the most frequent location for the entrance wound of the bullet. According to other authors, in the majority of cases, the bullet pathway in the head described a front to back, upwards and right to left, with a close range contact shot [18].
Drowning suicides occurring in rivers or in the sea are usually more publicized on social media. However, we found that, among the elderly, it is happening more frequently at their own home. This can be explained by the higher difficulty of older in moving around. This is also true for suicide cases of jumping from a high place, in which the victims’ residence was also the preferred location.
In intoxication suicides, it was expected to find an association between the residence area and the type of substance used, as in rural areas pesticides are more frequently used [19], but no significant statistical difference was found. In Portugal, new legislation (Law 26/2013 11th April) [20] recently imposed the obligation for people to take a specific workshop when trying to buy this type of products; however, outcomes of this measure are still to be found at the moment. Regarding corrosive substances, bases were more frequently used, and it can be due to being easier to purchase, like in common drugstores. In most hanging cases, males and females used the same type of the ligature material, most commonly a nylon (laid fiber) rope, an electric wire or a simple leather belt, which is easy to be found in their own home. Self-inflicted incised wounds that have a fatal outcome tend to be more commonly produced on the wrists and arms or in the inner surface of the throat [17]. The most frequent locations for the wounds were the neck, thorax and abdomen, which means that victims mostly try to reach places with vital organs and vascular structures, and being therefore succeeded. Paraschakis el al. [8] in Greece and Shields et al. [9] in Kentucky observed that a suicide note was left by the victim in 27.8% and 12.4% of elderly suicides, respectively. Unfortunately, in the present study this information lacked on most of the files. Having access to the suicide note could help understand the suicide motivation and the mental status of the victim, and it should be included with more detail in further studies.
The great majority of victims from our study had no documented survival time at the suicide scene. This can be due to the use of more lethal methods, to the fragility or even the victims’ age. Conwell stated that this greater lethality can be explained by the vulnerability of this age range that are more susceptible to bodily damage, and by their social isolation, which makes them more difficult to rescue [12]. In our study, in 68 cases where death occurred at the hospital, half of them happened in a short time span (less than 24 hours), which reflects this lethality. Victims who committed suicide by intoxication were more likely to have a longer surviving time (up to 7 days) than those who used a sharped object. This could be explained by the lesser lethality of these methods, associated to not knowing the lethal dose of a certain drug, by ignoring the accurate location of vital structures and by the inappropriate use of the instrument, producing less serious injuries. In matters of toxicological exams, like Shields et al. [9] found Kentucky, the majority of ethanol analysis was negative. It can be assumed that the intent of dying is so strong that there is no need of an “extra help” to give courage for committing it. The positivity of that blood analysis, either toxic or nontoxic concentration, was frequently for benzodiazepines, which can be explained by the widespread use of these types of drugs in this age range. The same was observed by Dias et al [21]. Antidepressants were also found in blood analysis in an important percentage (20.8% in nontoxic concentration), which could reflect the need for treating the prevalence of depression among this population [12].
Physical and Mental StatusA review from Conwell stated that medical conditions like chronic pain syndromes, malignancies and diseases of the cardiovascular, pulmonary, and central nervous systems are associated with increased risk of suicide in elderly [12]. A medical condition was present in the majority of cases from the present study, which is normal in this age range. These findings are consistent with those that Shelef et al obtained in Israel [7], however the same authors noted that individuals with physical illness committed suicide at an older age, which wasn’t found in our study. Conwell et al observed that psychiatric disorders are present in the majority of elderly suicides, particularly major depression which is the most consistently associated [22]. From our sample, approximately 70% had a known psychiatric disorder, a result similar to what was obtained by Paraschakis et al in Greece (62.5%) [8]. Many cases were diagnosed with depression, which is in accordance with evidences from previous reviews [12,22-24] and similar research publications [6-8]. In addition, we noticed that elderly victims with history of psychiatric disease were more likely to commit suicide at younger ages, phenomenon also observed by Shelef et al in Israel [7]. The percentage of elderly with suicide ideation was similar to the percentage of those without it. This reflects the conclusions of Conwell et al that older adults express their suicide ideation less frequently, compared to younger adults [25]. They also concluded that females are more likely to have suicide ideation, even though the suicide rate for males is much higher than females [25], which was what we observed in our study. This finding can draw the attention of families and health care providers to the problem of communication, especially concerning elderly men, as they tend to communicate less their thoughts or intentions.
Concerning suicide motivation, Fassberg et al stated that illnesses and disabilities are thoughts experienced as suicidogenic by elderly, when they play as a threat to one’s independence, sense of usefulness, value, dignity and pleasure with life [26]. Conwell, after reviewing several studies about suicide motivation, concluded that all share the common motifs of social and psychological disconnectedness [12]. The present study observed that psychiatric disorder was the most frequent suicide motivation reported by the victims’ relatives, which, based on the anterior evidence from Fassberg et al, can be considered suicidogenic in manner that it could be a threat to the individual’s independence. Based on the previous evidence from Conwell, it is also a source of psychological disconnectedness. We also observed that elderly that had lost their autonomy, or had an incurable disease, were more likely to commit suicide at younger ages, which can be explained by the unsolvable character of these conditions, resulting in hopelessness. Males were more likely than females to have as suicide motivation a loss of autonomy or a relationship breakup, that is, dependent on the relationships with others. Minayo et al concluded that social isolation and loneliness affects mainly men, aspects that also depend on the relationship with others [24]. Bereavement is frequently reported as being associated with suicide in older adults [23], however, in our study, only a small percentage of individuals reported such suicide motivation.
The majority of elderly in our study didn’t have a known previous suicide attempt. This fact usually reflects a strong intent to die, meaning that victims’ mainly succeed at their first suicide attempt. The same was observed by Paraschakis et al in Greece [8]. Females were more likely to have a previous suicide attempt than males, which is consistent with a review from Minayo et al. [24]. Usually this means a stronger intent of males to die, and their use of highly lethal methods. In cases where there were two previous suicide attempts, it was found that the final attempt was made through a more lethal method than the first (e.g. intoxication versus hanging).
ConclusionIn Portugal, according to data from INE, elderly population increased in the past decades, a consequence of the sociodemographic aging process. In parallel, an absolute and also a relative increase of suicide cases among that age group was registered. The analysis of forensic autopsy data allows for a more detailed characterization of this public health problem. By knowing one’s reality, it can help those responsible for defining appropriate health policies to implement more effective measures for suicide prevention in the elderly. The contribution of Forensic Medicine in suicide prevention is important and necessary, and it shouldn’t be neglected, considering the eminently social character of this medical discipline. It is well know that successful suicide prevention is very difficult to achieve because of the complexity associated to suicide behavior. In the specific case of elderly population, it can be helpful elaborating specific guides aimed for the relatives, containing explanatory measures in how to restrict access to the more lethal methods, which can be a rather easy prevention strategy to implement. This should include awareness programs that can be helpful in avoiding social isolation of older people, which can lead to more efficient health programs and more frequent visits to or by the doctor, mainly for the purpose of early diagnosing and treating psychiatric disorders, one of the main risk factors associated to this type of behavior.
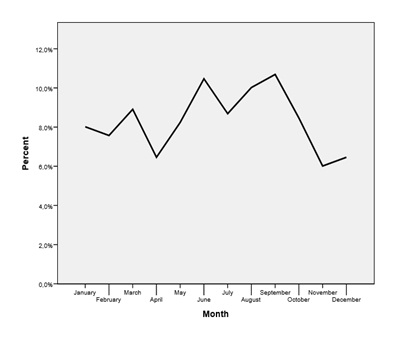
Graph 1: Distribution of suicides by month.
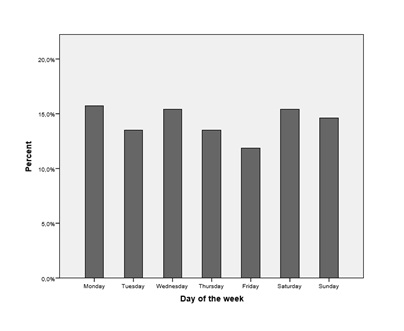
Graph 2: Distribution of suicides by day of the week.
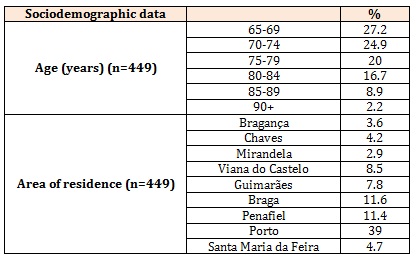
Table 1: Sociodemographic data.
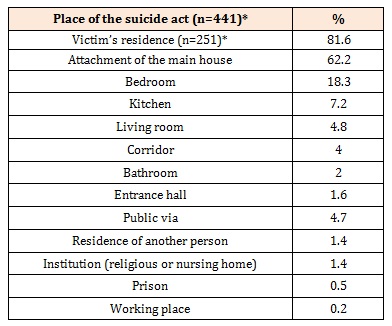
Table 2: Place of the suicide act.
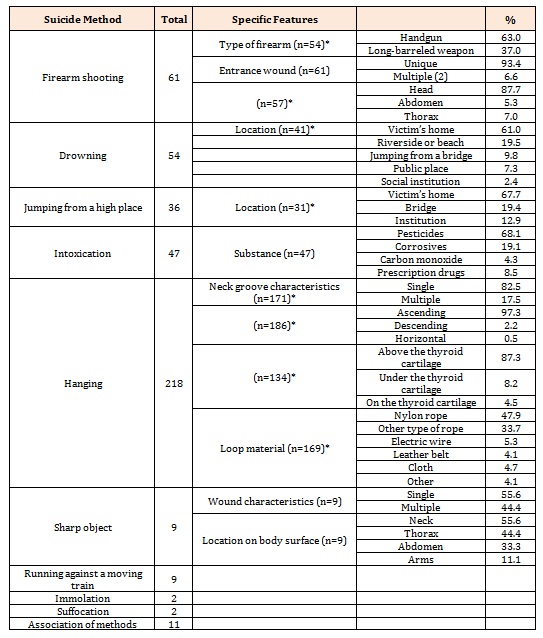
Table 3: Specific features about the different suicide methods.
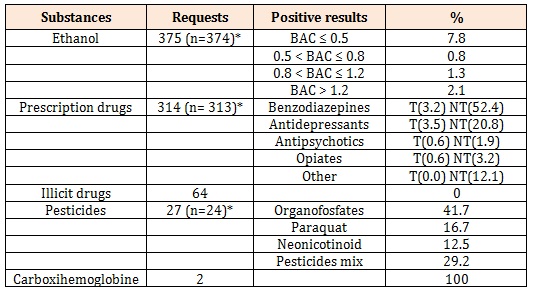
Table 4: Toxicological requests.
BAC = Blood Alcohol Concentration (g/dL)
T = Toxic concentration NT = Non toxic concentration
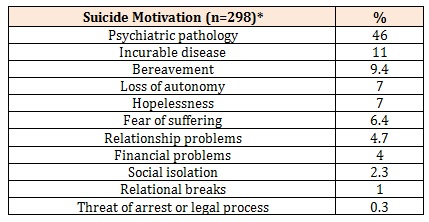
Table 5: Suicide motivation.





Chat with us on WhatsApp