Citation: Rabhi I, et al. Isolated Palmaire Luxation of the Base of the Fifth Metacarpian in a Boxer. J Ortho Bone Disord 2017, 1(5): 000126.
*Corresponding author: Rabhi I, Department of Trauma and Orthopedics, CHU Hassan II, 30000 Fez, Morroco, Email: ilyastraumato@gmail.com
The post-traumatic dislocation of the fifth finger is a rare lesion. In the absence of treatment, this lesion results in joint degeneration and instability. This lesion is usually unstable, treated by open, Closed. We report the case of a carpalmetacarpal dislocation isolated palmar pure in a boxer, clinically the patient presented a disturbance of rotation of 15° with a shortening of 5 mm. The standard radio graphy showed a palmar dislocation of the base of the 5th Metacarpal with a diastasis between the 4th and 5th metacarpal. The patient was treated with a parallel insertion of the M5M4M3 after reduction of the dislocation with closed focus and immobilization plastered for 45 days.
Keywords: Carpo-metacarpal dislocation; Palmar; Broaching
Pairedcarpo-metacarpal dislocations are rare lesions, palmar displacements even more rare and presents 6% of the carpometacarpal dislocations [1]. The first palmar carpometacarpal dislocation was described by Rivington [2] in 1968 and Nalebuff [3] Fromthis date, 7 cases have been described in the literature, ouris the 9th (Table 1). These rare lesions often occur in a young person following a high-energy trauma, the lesion may go unnoticed initially, hence the interest of a careful and complete radiographic assessment. The treatment is based on the reduction in closed focus in emergency followed a splint or an embedding according to the stability of the dislocation, sometimes an open-heart reduction is used, combined with an internal fixation.
ObservationA young 28-year-old boxer who presented a wrist stroke during a fight, a trauma closed with his left hand. The hand was painful with significants welling without sensory-motor deficit. The little finger was shortened by 5 mm (Chmell line) and blocked in ulnar inclination. Radiographic images made in emergency show a palmar dislocation carpo-metacarpal of the 5th ray without associated fracture (figure 1).
The patient was operated under loco regional anesthesia, under the control of the shine enhancer, were alized two small first internal channels a few millimeters in front of the ulnar border of the 5th metacarpal, a reduction of the luxation to focus Closed with the sensation of a jump during the maneuver, the reduction was stable. The patient benefited from a double parallel embedding of the last 3 fingers and placement of an antebrachio-palmaranterior for 45 days with a mobilization Active of the fingers and elevation of the limb during the first days (Figure 2).
At 6 months follow-up, the patient was reviewed in painless consultation and hadal most complete functional recovery: the wrist strength was 90% compared to the contra lateral wrist, the fingers and the thumb Kapandji score at 10, flexion extension of the wrist at 90°, normal prognosis and radial inclination at 35°; Ulnar ultra sound at 45° and an excellent DASH score calculated at 0.8. Clinical radio monitoring showed no evidence of early carpal-metacarpal osteoarthritis.
DiscussionCarpo-metacarpal dislocations are rare lesions that present less than 1% of all wrist and carp trauma [1], often resulting from high-energy trauma due to the high stability of the carpometacarpal. Thanks to the intermetacarpal ligaments, palmarcarpo-metacarpals and dorsal carpometacarpals. The diagnosis is based on the realization of dynamic radio graphs [2] because it can go unnoticed on ordinary pictures. A movement of the fifth meta carpal with respect to the hamatum, which can range from the small displacement to the overlap, is then observed. In addition, some authors recommend a complementary computed tomography scan [3,4].
Clinically, there is a deformity of the hand, a hematoma and a functional importance.
Carpometacarpal dislocations are classified according to Costagliola (1966) in complete or partial spatular carpometacarpal dislocations, in palmar luxation, in lateral dislocations particularly interesting in the fifth ray and in divergent luxations [27]. The palmar form of the carpometacarpal dislocations represents 6% of the dislocations [27].
For treatment, there is no consensus in the literature, but surgical treatment is often necessary, including a closed-heart reduction followed by an intermetacarpal or carpo-metacarpal attachment [29].
For us, percutaneous embedding – when closed reduction is possible, but many authors prefer open-pit reduction especially in fractures dislocations to have an anatomical reduction [30,5,31,32]. Postoperative immobilization is generally recommended for four to six weeks.
Several complications have been reported in the literature, such as decreased grip strength, persistence of residual pain, secondary displacement, and subluxation [33]. For our case although there were no complications but this is not justifying.
It can be said that the prognosis of the carpometacarpal dislocations is often good, but there is a risk of persistent pain and limitation of movements.
ConclusionThe palmar carpo-metacarpal dislocations are rare lesions which deserve to be systematically investigated in the closed trauma of the hand. The treatment is surgical with inter-metacarpal or carpo-metacarpal embedding. Subject to urgent and correct treatment, they are generally of good prognosis.

Figure 1: Pre operative imaging.
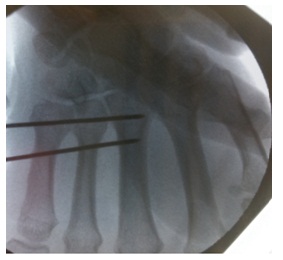
Figure 2: Perioperative imaging.




