Citation: Gharaibeh A, et al. Transient Synovitis of Hip Joint in Childhood. J Ortho Bone Disord 2017, 1(6): 000131.
*Corresponding author: Ahmad Gharaibeh, PhD, MPH, Orthopaedic Surgeon, Department of Orthopaedics and musculoskeletal trauma, UNLP, Kosice, Slovakia. Tel: +421915344317, Email: gharaibeh@seznam.cz
Objective: Transient synovitis the most common cause of acute hip pain in children aged 4-8 years. The aim of the study is to determine the prevalence of hip joint pain in childhood based on a retrospective analysis.
Methodology: This is retrospective study. We’ve analysed patient records with certain diagnosis during 2012 at the UNLP Paediatrics Orthopaedic and trauma Clinics in Kosice, Slovakia. We’ve examined 5523 paediatric patients. 73 patients found with hip pain. Outcomes were measured and analysed over one year. Data analysis of the results was processed using the statistical functions of Microsoft Excel.
Results: During 2012, at the paediatric Orthopedic Clinic in Košice, we examined a total number of 5523 patients with various musculoskeletal problems. 73 patients during one year hip joint pain was found. In 37 cases (51%) were transient synovitis of hip diagnosed, in 13 cases (18%) a soft tissue injury to the hip joint was found, in 9 cases (12%) Legg- Calve-Perthes disease was diagnosed, in 8 patients (11%) septic arthritis of the hip was found, in 5 patients (7%) fracture of the proximal part of Femur was detected and one patient was diagnosed as malignant Tumour (1%). 46 patients were treated as outpatient and 27 patients were hospitalized.
Conclusion: Transient synovitis of the hip joint is the most common cause of hemorrhage and sore throat in childhood, with occurrence between the 3rd and 6th year of age. The patient recovers usually between 7 to 10 days. Treatment of choice is resting and administration of non-steroidal anti-inflammatory drugs. Antibiotics are not indicated.
Keywords: Transient synovitis of hip; Hip pain; Incidence; Septic hip; Ultrasonography scan
Transient synovitis is the most common cause of acute hip joint pain in children four to eight years of age. Definition of transient synovitis is Hip pain due to inflammation of the synovium of the hip [1-3]. Children with this condition typically present with hip pain for one to seven days, accompanied by limping or unable to bear weight due to pain. Male-to-female ratio is 2:1. Transient synovitis of hip has an uncertain ethology and remains a diagnosis of exclusion. First, septic arthritis must be ruled out and osteomyelitis of hip joint as well [3, 4]. Septic arthritis should be suspected in a patient with severe pain or spasm of hip, a fever of temperature above 38.5°C and C-reactive protein higher than 20mg/l, white blood cells higher than 12000 cells/µl, erythrocyte sedimentation rate greater than 40 mm per hour (ESR > 40 mm/h). Differential diagnosis includes Legg-Calve-Perthes disease, developmental dysplasia (late presentation), Slipped Capital Femoral Epiphysis, Multiple Epiphyseal Dysplasia, rheumatoid arthris, bone tumour, testicular disorders, groin pain, Lyme disease and finally soft tissue or bony trauma to the hip joint must be rolled out [1, 4-6].
The transient synovitis of hip has many synonyms such as irritable hip, transitory coxitis, coxitis fugax, acute transient epiphysitis, coxitis serosa seu simplex, phantom hip disease and observation hip [3].
Diagnosis of transient sinovitis of hip in our teaching department and our clinics is confirmed with physical examinations, anteroposterior and frog leg radiological views of the hips. Sometimes we can see medial joint space widening on the x-rays. Ultrasound of both hip joints helps to roll out hip effusion. Full blood counts, Creactive protein, and white blood cells are always within normal range. Erythrocyte sedimentation rate, rheumatoid factor, ASLO, antinuclear antigen, HLA B 27, uric acid in blood serum, procalcitonin, calcium level, and vitamin D level also shows normal values. Magnetic resonance imaging (MRI scan) or skeletal scintigraphy to be done if the symptoms did not disappear after 10-14 days and also
Treatment of transient synovitis of hip is by bed rest and non-steroidal anti-inflammatory drugs like Ibuprofen. Regular observations including temperature checks to exclude the onset of fever to be done. In some cases skin traction is applied to relieve the pressure inside the capsule of the hip joint. If significant pain and limping persist seven to 10 days after the initial presentation, the patient should be re-evaluated. Cause of transient synovitis is unknown, however may be related to bacterial or viral infection, higher interferon concentration, allergic reaction, less valuable trauma [1, 2, 4].
Complications of Transient Synovitis are Coxa Magna or Perthes Disease.
Follow-up care of Transient Synovitis repeat X- Rays in 6-12 months to evaluate Perthes disease [3].
The study which done by Ragab et al. on 72 patients with none traumatic paediatric hip pain shows that, 40.2% of children had transient synovitis of hip [7]. Hart JJ. In 1996 found that transient synovitis of the hip is most common and it is diagnosis of exclusion and after 10 day patient must be revaluated [8]. Do TT. Confirmed in 2000 that transient synovitis of the hip is the most common case for hip pain and limping in young children [9]. Between 1979 and 1996 kocher et al. they used blood tests, USG scan to differentiate between septic hip and transient synovitis of hip [10]. Eich et al found that the best way to evaluate the hip pain and limping is by ultrasonography scan, blood tests and body temperature checks [11]. The retrospective study which was done between 1992 and 2000 on 163 patients with hip pain and limping shows that 71% had transient synovitis of hip [12].
The study by Naranje et al shows that Transient synovitis is the most common diagnosis Blood tests, physical examinations and body temperature is essential for differential diagnosis [13].
On 2007, Kwack et al. presented the results of a study with twenty patients, which evaluated the useful of MRI for differential diagnosis between septic hip and transient synovitis of hip [14].
MethodologyThe aim of study to determine the incidence of hip joint pain in childhood based on a retrospective analysis; find the cause of hip joint pain in childhood. Make a database for further research to increase the effectiveness of investigation and differential diagnosis. In this retrospective study, we analysed the records of patient with certain diagnosis during 2012, at the UNLP paediatric Orthopaedic and trauma Clinics in Kosice, Slovakia. We examined 5523 paediatric patients, 73 patients with hip pain. Outcomes were measured and analysed over one year. Data analysis of the results was processed using the statistical functions of Microsoft Excel.
ResultsThe total number of children demonstrated in our clinics with hip pain was 73 patients during one year, in 37 cases (51%) were transient synovitis of hip diagnosed, in 13 cases (18%) a soft tissue injury to the hip joint was found, in 9 cases (12%) Legg- Calve-Perthes disease was diagnosed, in 8 patients (11%) septic arthritis of the hip was found, in 5 patients (7%) fracture of the proximal part of Femur was detected and one patient was diagnosed as malignant Tumour (1%). 46 patients were treated as outpatient and 27 patients were hospitalized.
DiscussionTransient synovitis of the hip joint (coxitis fugax) is a non-specific inflammatory reaction affecting the hip joint [1, 3, 4]. It is usually preceded by an inflammatory process at a different site, most commonly viral upper respiratory tract inflammation or inflammatory disease of the gastrointestinal tract [2, 3]. In clinical examinations we find limping children, limited abduction and internal rotation in the hip joint. Pain can be localized in the groin, thigh or knee [3, 13]. The baby is in a good overall condition without a fever. Within the differential diagnosis, a basic laboratory examination (blood count, CRP, erythrocyte sedimentation to eliminate bacterial infection), ultrasonography examination (joint effusion confirmation) and x-ray examination (exclusion of Perthes disease, trauma, osteomyelitis, femoral proximal epiphysis) as reported by Eich and Kocher [10, 11].
ConclusionHip pain in childhood is a common problem. Transient synovitis of the hip joint is the most common cause of hip pain in childhood. Usually occurs in children between 3 and 6 year of age. Transient synovitis of the hip joint is the most common complication of sore throat in childhood. The illness usually stops within 7 to 10 days. Treatment consists of resting and administration of nonsteroidal anti-inflammatory drugs. Antibiotics are not indicated.
The investigation of painful hips in children, based on physical examinations, hip ultrasound, body temperature, and CRP, may reduce the number of radiographs, MRI and hospital admissions.
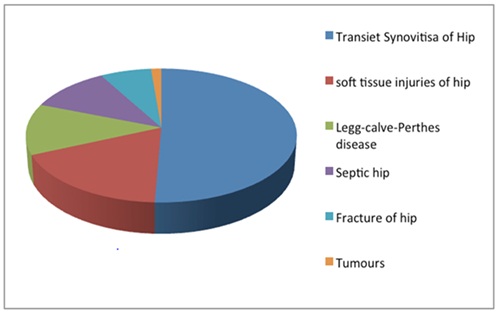
Graf No 1 incidence of cases
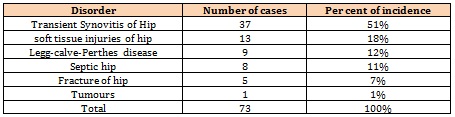
Table 1: Number of cases and per cent of incidence





Chat with us on WhatsApp