
Citation: Reeta Mandal. Studies on Phytochemical Screening, Antimicrobial, Antioxidant and Cytotoxic Activities of Caragana Jubata of Nepal. Adv Pharmacol Clin Trials 2016, 1(1): 000104.Juan G Robledo Avendaño, et al. Reconstruction of Endodontically Treated Teeth Using Anatomic Fiber Posts: A Case Report. J Dental Sci 2016, 1(2): 000111.
*Corresponding author: Juan Gaston Robledo, DDS, Endodontist, University of Buenos Aires, Buenos Aires, Argentina, Email: jgrobledo@gmail.com
A clinical case is presented in which the prosthetic restoration of two anterior teeth, esthetically compromised was required. Quartz fiber posts were used in wide non rounded root canals. A relining technique with composite resin was used to accomplish a better adaptation of the tooth posts to the internal walls of the tooth, thus reducing the required quantity of adhesive resin cement and achieve a best friction to favor fixation. In this research it is emphasized the importance of communication, teamwork and integration of prosthetic as well as endodontic concepts to confront the challenge of a better adaptation of the posts to non rounded root canals.
Keywords: Anatomic fiber quartz posts; Endodontically treated teeth; Integration of prosthetics and endodontics concepts
At present there is a high demand of restoration in endodontically treated teeth (ETT) [1]. Recent scientific information emphasizes that ETT undergo different alterations like humidity loss, resistance alterations and biomechanical behavior under stress, dentin resistance and change in the nature of collagen [2]. It is necessary to emphasize the importance of the integration of prosthetic and endodontic concepts. The aim of restoration is to return shape, function and prevention of root fracture [3,4]. It has been demonstrated and recognized that the sealing obtained through a crown restoration is vital in the prognosis of the root canal treatment of teeth as well as in the apical sealing [5,6]. Dentistry therapeutics is today aimed at treatments of conservation of tooth structure and minimum invasion. There exist multiple reconstruction options, from former cast tooth posts, metallic prefabricated cast posts, to first generation carbon fiber and resin tooth posts. However, it should be discussed if there is a more adequate option. Different factors are to be considered: type of teeth and root, occlusion and disocclusion strength, biological conditions of the teeth, root anatomy, dental infrastructure, etc. Endodontic tooth posts have mainly two functions: to increase the retention of a restoration material in the dental remaining and to distribute stress uniformly along the root. Several studies show that the implementation of posts can produce stress and a predisposition to fracture, the resistance of endodontically treated teeth is directly related to the remaining internal tooth structure [7,8]. Some research was also performed on mechanical stress analysis using removed teeth, restored teeth and natural teeth through load increase until fracture was achieved. Teeth keeping natural crowns resulted to be the most resistant [9].
It is already known that endodontic treatment not only make tooth lose strength, but also there is loss of humidity and changes in the collagen. Tooth suffer significant differences from physical as well as mechanical point of view when being compared to a vital teeth, increasing its fracture potential [3,10-13]. With the advent of esthetic needs, quartz fiber posts are preferred over other systems, especially considering that anterior teeth will be restored with ceramic crowns. There are different posts designs that can be adapted somehow to the inner dentin walls, trying to minimize the dentin wear to avoid weakening the tooth and achieve a better anchoring and adaptation, thanks to the new luting materials and techniques for bonding [8,14-16]. The ideal shape of a post should be cylindrical with an apical conic portion and a crown portion compatible with bonding techniques for restoration. In channels previously prepared there is structural loss and weakness is increased and consequently the risk of fracture [17,18]. It is mentioned that the modulus of elasticity of the tooth post should be similar to the dentine root in order to distribute strength along the post [7]. It was also reported that the modulus of elasticity of the post should be similar to the dentine to reduce stress concentration and transmit strength effectively [19]. The advantage of anatomic tooth posts is that after submitting to a resin rebasing technique; the whole combination may fit closely to the duct walls, achieve more friction and thus reduce the volume of cement necessary for the fixation; as a result achieving less possibilities of dental cement removal. The design, adaptation and adjustment are mentioned in different research articles [14,20]. This research article presents a case of two anterior pieces restored with individualized prefabricated posts and ceramic restoration.
Case StudyAdult patient presented at the consultation for the aesthetic need of the anterior area restoration. After performing vital pulp tests, tooth 8 presented previous restorations, loss of substance and a need of endodontic therapy. Tooth 9 showed previous restorations with filtration, discoloration, loss of substance, and an unsatisfactory previous endodontic treatment after a radiographic view (Figure 1).
An endodontic therapy was performed in tooth number 8 and an endodontic revision in tooth9. After local anesthesia and positioning of rubber dam, both teeth were treated and tooth 9 was dismantled. The guttapercha was removed with Gates Glidden bur#2 and #3 (Dentsply Maillefer, Ballaigues, Switzerland) and limes Hedstroem #30 (Dentsply Maillefer, Ballaigues, Switzerland). Channels were shaped and remodeled with Pro Taper Universal rotary system and channels 8 and 9 were filled. (Figure 2) shows the complete sequence.
After evaluating the root anatomy and throughout the evaluation of the coronary remaining it was decided to use a quartz fiber post system (Macro-Lock, RTD, France) for an intraradicular anchor; in order to achieve a better adaptation within the channel, follow the anatomy and achieve greater friction. Ducts were de-filled with Gates Glidden #2 and #3 (Dentsply Maillefer, Ballaigues, Switzerland), after that, Peeso #1 and the complete drilling sequence corresponding to the post system employed (Figure 3).
Selected posts were checked according to depth and were adapted using composite (Z100, 3M ESPE, St. Paul MN, USA) by taking the root canal impression with manual pressure and polymerization (Figure 4).
Then, the concrete poles cementing was made with dual resin (Paracore, Coltene Whaledent) together with the radiographic check. Both pieces were rationally prepared with moderate chamfer termination. Soft tissues were prepared for impression using wire separation and the final impression was taken with silicone addition in one step (Zhermack Elite HD). Pure porcelain restorations (e.max, Ivoclar Vivadent) using resin cement were installed. Figure 5 shows the complete sequence Figure 6 shows an enlarged view of the final picture.
DiscussionAs previously formulated, the current trend in dentistry is to preserve tooth structure to a greater degree with minimum invasion. Thus, tendency has changed starting from the use of cast tooth posts to prefabricated cast posts currently available that allow a minimum dental preparation with quick resolution. Certainly, all this is considered conforming to the initial diagnosis. One of the main characteristics of this type or restorations is the possibility of dispersion forces, although some literature illustrates the opposite effect [7,8]. It is unquestionable that no system reinforces tooth structure and in any case, a healthy structure is the one that provides greater mechanical strength [9]. Along the same lines, antique publications have already demonstrated that the root canal treatment produces a tooth weakness that no treatment can restore completely [3,10-13]. Other point to consider is the shape of the post, which theoretically should correspond to the shape of the root canal. At this state of the proceedings is where the anatomy of the root canal can be a determining factor in the adaptation process. It could be argued that there are different post designs possible to adapt some way to the internal dentine structure, trying to minimize the dentine wear to avoid weakening the tooth and achieving a better tooth anchor and adaptation, with the help of new cementing materials and adhesion techniques [8,14-16]. The ideal shape of a post should be cylindrical with a conical-apical portion and a crown portion compatible with the systems of adhesion for restoration. In ribbon shaped canals previously prepared there is loss of the tooth structure, weakening increase, what makes it more susceptible to fracture [17,18,21]. It is worth mentioning that the modulus of elasticity of a post should be similar to the dentine root to distribute forces applied on the length of the post [7]. It was also reported that the modulus of elasticity of the post should be similar to dentine to reduce stress concentration and effectively transmit forces [19,22,23]. Anatomic posts have the advantage that, after a resin reline technique, the whole combination may closely adapt to the root walls, achieve more friction thus reducing the amount of cement necessary to fixation; as a result having less possibilities of dental cement removal. The design, adaptation and adjustment is mentioned in various research articles [14,20].

Figure 1: A: Pre op image. B: Pre op radiograph.
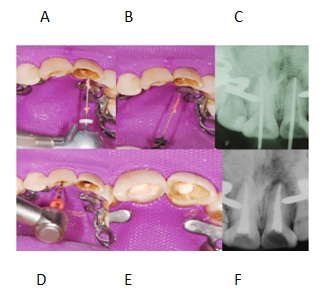
Figure 2: A and B: Removing guttapercha using Gates Glidden and Hedstroem files. D: Master GP adjustment. C: Canal instrumentation. E and F: Final obturation.
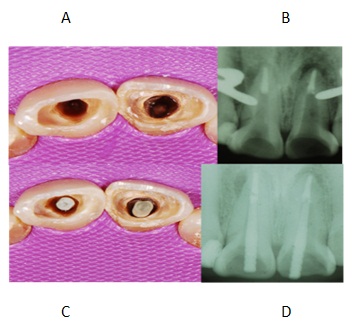
Figure 3: A and B: Posts spaces. C and D: Checking post adjustment and length.
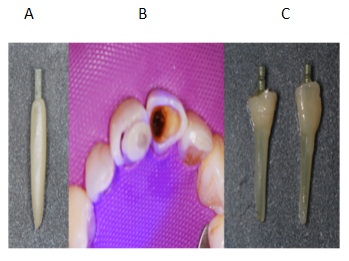
Figure 4: A and B: Adapting composite. C: After polimerization.

Figure 5: A and B: Cemented posts. C and D: Crowns preparation and impression using pvs material. E: Cemented crowns.

Figure 6: A: Post op image.




