Citation: Kandakure VT, et al. Effect of Functional Endoscopic Sinus Surgery on the Symptom Profile in Patients with Chronic Rhino-Sinusitis: Our Experience. Otolaryngol Open Access J 2016, 1(4): 000121.
*Corresponding author: Vinod T kandakure, Associate Professor, Department of ENT, Government Medical College, Opposite mamta hospital, Mitra Nagar, Latur, Maharastra, India, Email: vinodkandakure@gmail.com
Introduction: Chronic rhino-sinusitis defined as inflammation of the nose and paranasal sinuses. Functional endoscopic sinus surgery (FESS) has now become a well-established strategy for chronic rhinosinusitis refractory to medical treatment.
Aims: To study surgical technique of Functional Endoscopic Sinus Surgery, assess success rate of surgery, assess efficacy on long term basis, assess patients experience of procedure following endoscopic sinus surgery and confirm FESS as a standard modality of treatment in patients with refractory CRS.
Materials and methods: Prospective study of 33 patients of chronic rhino-sinusitis managed by FESS in period between December 2012 to December 2013. Patients underwent detailed history, ENT examination, X-ray PNS, diagnostic nasal endoscopy and CT PNS. FESS was performed and patients were followed at 1st and 3rd week, 3rd and 6 month.
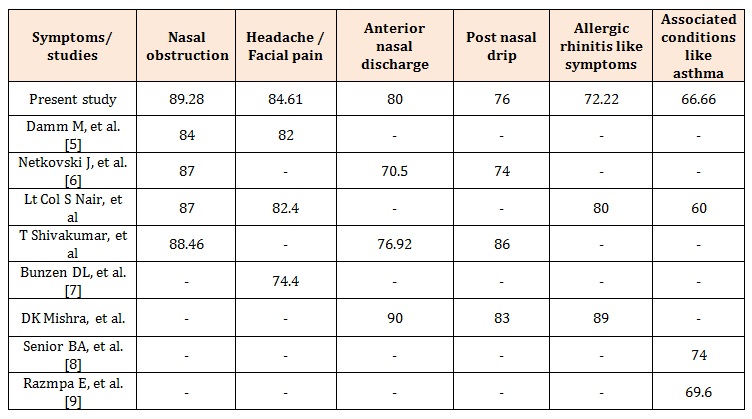
Results: Study concluded that 3 patients experienced relieving of symptoms by end of 3 weeks, 12 by 3 months and 28 patients by end of 6 months. On assessing post-operative symptom profile score 6 months after surgery; 89.28% patients showed improvement in nasal obstruction, 80% in anterior nasal discharge, 84.61% in headache/facial pain, 76.19% in post nasal drip, 72.22% in allergic rhinitis like symptoms and 66.66% in associated conditions like asthma.
Conclusion: It was observed that overall improvement was 84.84% in our study, hence we concluded that FESS is excellent method of treatment for CRS with minimal to mild discomfort to patient and minimal complications when performed by experienced surgeon.
Keywords: Chronic rhinosinusitis; Functional endoscopic sinus surgery; CT- PNS; Diagnostic nasal endoscopy
Chronic rhino sinusitis is one of the most commonly diagnosed chronic medical conditions in present time due to change in life style. The European Position Paper on rhinosinusitis and nasal polyps 2012 defines rhinosinusitis as inflammation of the nose and paranasal sinuses characterized by two or more symptoms, like nasal obstruction / blockage / congestion or nasal discharge (anterior or posterior nasal drip) and / or facial pain / pressure and / or reduction or loss of smell [1]. Sinusitis is a common problem that leads to a significant amount of health care expenditure and psychological impact on the patients by standing as a social stigma due to runny nose and foul smell. Treatment of sinusitis includes medical and surgical management. A course of medical management comprises antibiotics, antihistaminic, antiallergics, decongestants and topical and systemic steroids. If refractory to three courses of antibiotics then send patient to surgeon. Functional endoscopic sinus surgery (FESS) has now become a wellestablished strategy for chronic rhino-sinusitis refractory to medical treatment [2,3]. It is based on principle that diseased mucosa get reverted if ventilation and drainage are improved, thus restoring mucociliary clearance [4]. The present study is an attempt to study the effect of FESS on symptom profile of patients with chronic rhinosinusitis before and after surgery.
Aims and Objectives1. To study the surgical technique of Functional
Endoscopic Sinus Surgery (FESS).
2. To assess the success rate of surgery.
3. To assess the efficacy on long term basis.
4. To assess patients’ experience of procedure following
endoscopic sinus surgery.
5. To confirm FESS as a standard modality of treatment
in patients with refractory CRS.
Prospective study of 33 patients presenting with
complaints suggestive of chronic rhino-sinusitis managed
by FESS in period between December 2012 to December
2013. Maximum number (N= 12) of patients were
presented in age group 31-40 years. Patients less than 12
years were not included in the study. Mean age of
presentation was 38 years. Female patients outnumbered
the male patients with ratio being 1.35:1 Inclusion criteria
includes diagnosed patients of chronic rhino-sinusitis
by health professional, patient with sinusitis symptoms
for more than 12 weeks, endoscopic evidence of sinusitis,
radiological evidence of sinusitis. Exclusion criteria
patients under 12 years of age, immune-compromised
patients, cystic fibrosis, Wegener’s disease, previous sinus
surgery, sino-nasal malignancy, uncooperative patients,
terminally ill patient, pregnant and lactating female
patient. The selected patients were subjected to a detailed
history and complete ENT examination. X ray PNS
(water’s view ), diagnostic nasal endoscopy and NCCT
PNS were done to assess the extent of disease, condition
of nasal septum, mucosa, turbinates, Osteomeatal unit,
eustachian tube openings and coexisting anatomical
variations of lateral wall of nose. Patients were followed
at 1st week, 3rd week, 3rd month and 6th month.
During the postoperative follow up period, the symptoms
were assessed using the following grades-
0. No improvement
1. Mild improvement
2. Moderate improvement
3. Much better improvement
Naso-endoscopic suction toilet was also performed during which the healing of the cavities and patency of the ostia were monitored. Recurrence of the disease and presence of crusts, synechiae and mucopus were also observed. Grading of symptoms and naso-endoscopic suction toilet was done at the end of third week, third month and at the end of six months.
Observations and ResultsIn our study, 33 patients of chronic rhino-sinusitis
were included. All patients were subjected to FESS under
general anaesthesia. Patients follow up were done at 3rd
week, 3rd month and 6th month and various parameters
were observed which are discussed below.
In all patients, preoperatively symptoms were graded as:
1. No symptoms
2. (Mild) -symptoms not disturbing sleep or day to day
activity
3. (Moderate) -symptoms disturbing day to day
activities, with occasional absence from work or
disturbed sleep
4. (Severe) -symptoms disturbing day to day activities,
with absence from work and disturbed sleep.
The commonest symptom was nasal obstruction (84.84%) followed by head ache or facial pain (78.78%). Symptoms of all patients were assessed and graded preoperatively (Table 1). Maximum number of patients (N = 16) had duration of symptoms ranged from 1 year to 5 years. Average duration of symptoms was 3 years and 4 months, the range being 3 months to 20 years. In our study, Anterior rhinoscopy revealed polyp in 13 patients, mucopus in 12 patients, ITH in 8 patients, mild DNS in 5 patients, middle turbinate hypertrophy in 3 patients whereas congested mucosa in 2 patients (Figure 1). Posterior rhinoscopy revealed posterior extent of the polyps at the choanae in 6 patients. X- Ray PNS (water’s view) done to assess nasal septum. X- Ray of PNS showed mild DNS in 5 patients (3 patients with left sided DNS whereas 2 patients with right sided DNS) and central septum in 28 patients. We performed preoperative diagnostic nasal endoscopy in all patients which revealed mucopus in 17 patients, polyp in 15 patients, ITH in 8 patients, congested mucosa in 6 patients, mild DNS in 5 patients, Bulbous middle turbinate in 3 patients whereas accessory ostium in 1 patient.
NCCT nose and paranasal sinuses done in all patients preoperatively which revealed polyposis in 15 patients out of which 6 were bilateral and 9 were unilateral cases. In our study, post-operative follow up naso-endoscopy was done at interval of 3rd weeks, 3rd months and 6th months. At the end of 3 weeks, 15 patients were having normal, healthy nasal cavity. 17 patients were having crusting, 4 patients were having synechiae whereas 4 were having mucopus. No patient had recurrence of polyp at the end of 3 weeks. At the end of 3 months, number of patients were having normal, healthy nasal cavity raised to 23. 6 patients had crusting, 4 patients were having mucopus, and 2 patients had synechiae. No patient had recurrence of polyp at the end of 3 months. At the end of 6 months, 27 patients had normal healthy nasal cavity, 3 patients were having mucous whereas 2 patients had recurrence of polyp (Figures 2 & 3). In our study, postoperative symptom profile score is assessed based upon the improvement in symptoms after surgery (Table 2). At the end of 6th months, 89.28 % patients showed improvement in nasal obstruction, 80 % in anterior nasal discharge, 84.61 % in headache / facial pain, 76.19 % in post nasal drip, 72.22 % in allergic rhinitis like symptoms and 66.66% in associated conditions like asthma. Patients’ experience to surgical procedure (FESS) in our study were assessed and results were; 2 patients experienced the procedure without any discomfort, 23 with mild discomfort, 7 with moderate discomfort whereas only 1 patient with severe discomfort. In our study, 3 patients experienced relieving of symptoms by the end of 3rd weeks, 12 patients experienced by the end of 3rd months whereas 28 patients experienced relieving of the symptoms by the end of 6 months.
DiscussionChronic rhino-sinusitis is one of the most common health care problem for which an individual seeks medical care resulting in high direct medical costs, including costs of an office visit, diagnostic tests, antibiotics or other pharmaceuticals, procedures or surgeries, hospitalization and/or complications of treatment. CRS not only causes significant physical symptoms but also results in substantial functional and emotional impairment. By definition CRS is a group of disorders characterized by inflammation of the mucosa of the nose and the PNS of at least 12 consecutive weeks duration. Histopathologically, CRS is divided into two broad categories:
1. Polypoidal mucosal changes with eosinophilia,
representing more severe damage.
2. Submucosal serous gland hyperplasia
Pathophysiology of Chronic Rhinosinusitis
Allergies and CRS: The causal relationship of AR to CRS is conflicting, although there is no question that there is an increase in association of AR in patients with CRS. Mechanism by which AR can cause CRS include swelling of the sinonasal mucosa produced from nasal allergic inflammation initiated by cytokines and other allergy mediators, causing obstruction of the sinus ostia which could lead to secondary bacterial infection. Hence allergic patients with CRS respond poorly to medical management.
Bacteria and CRS: Role of bacteria in CRS remains elusive. They may play a direct or indirect role in the development or perpetuation of CRS. The presence of bacteria within the nose and PNS might initiate CRS and cause persistence of disease or exacerbate a noninfectious inflammatory process through bacterial colonization. Bacteria found in association with CRS are peptostreptococus, propionibacterium spp, prevotella, streptococcal variants, cornybacterium spp, Haemophilus influenzae, pseudomonas spp, enterobacter spp.Fungi in CRS: Fungal colonization of the nose and PNS may be a common finding in both normal and diseased states because of the ubiquitous nature of the fungi. Under certain circumstances, however, clinically apparent forms of fungal proliferation occur. This leads to the formation of fungal balls or saprophytic growth of fungus. In these cases, fungal mycelia accumulate and occupy available spaces within the nose and PNS in the absence of significant mucosal inflammation. Treatment is directed to extirpation of the offending fungal growth. In other forms, however, it is the inflammatory response to the fungus that is the primary manifestation of the disease. In these forms, a small amount of fungi results in clinically significant disease, demonstrating the ability of the fungal exposure to initiate a cascade of inflammatory events.
At present, it appears that multiple conditions may play a direct or contributory role in the pathogenesis.
Bernoulli’s Principle
Pressure drop next to a constriction causes a suction effect pulling the sinus mucosa into nose. Diagnosis of CRS requires the presence of at least two major factors, or one major and two minor factors. The signs and symptoms must persist for at least 12 consecutive weeks to qualify for CRS.
Sinus Symptom
The present study aims to analyze the effect of FESS on symptom profile of patients with chronic rhino-sinusitis before and after surgery. Various parameters were assessed and were compared with various other studies. Preoperative symptom profile score of our study were compared with that of other studies (Table 3). All patients were subjected to FESS under general anaesthesia. Hypotensive general anesthesia has an advantage of controlled ventilation, reduced bleeding and pain. The sites of infiltration of the local anesthetic agent (2% lignocaine with adrenaline 1: 80,000) are uncinate process, bulla ethmoidalis, and root, head and posterior end of the middle turbinate. In cases of nasal polyps, the polyps too are infiltrated. It is important to wait for 10 min after infiltration before surgery is commenced 5, 27.
Surgical Techniques
The basic steps of the anterior to posterior Messerklingler’s technique include the following:
Uncinectomy
After medializing the middle turbinate using a Freer’s elevator, the uncinate process is identified and its free margin is palpated with a ball probe. Incision is given in the shallow groove between the uncinate process and the lacrimal crest, starting superiorly at the level of the insertion of the middle turbinate to just above the inferior turbinate. Using Blakesley forceps the uncinate process is grasped and removed with a twisting motion.
Middle Meatal Antrostomy
After uncinectomy the natural ostium of the maxillary sinus can be approached. The ostium lies at the junction of the anterior and inferior walls of the ethmoidal bulla. If the ostium is incompletely seen, then it is widened with a curette. Posterior fontanelle is examined for any accessory ostium. If present, the natural and the accessory ostia are connected using a backbiting forceps. Otherwise, a scissors is used to cut and widen the natural ostium.
Anterior Ethmoidectomy
The anterior wall of the ethmoidal bulla is entered with the tip of a straight forceps. The inferior and medial wall is completely removed while maintaining the posterior wall intact, the lamina papyracea forms the lateral boundary and skull base the superior boundary of dissection. The posterior wall is most of the time fused with the ground lamella.
Posterior ethmoidectomy
The posterior ethmoidal cells are entered through the postero-infero-medial part of the ground lamella. The septae of the posterior ethmoidal cells are removed carefully. The boundaries of dissection are posteriorly the anterior sphenoid wall, laterally the lamina papyracea, superiorly the skull base and the superior turbinate medially.
Sphenoidotomy
After posterior ethmoidectomy, the sphenoid sinus is entered postero-inferomedially using a suction tip/forceps. The anterior wall of the sphenoid sinus can be ossified in some making it difficult to enter. Up to 5% of the sphenoid sinuses may not be pneumatized. After entering the sphenoid sinus the bony anterior wall is gently removed with the Kerrison’s punch upto the level of skull base and medial orbital wall. The intersinus septum is later released and the sinus examined.
Frontal Recess Surgery.
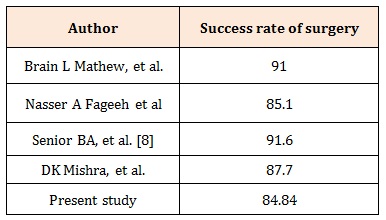
The frontal sinus opening can be visualized by dissecting upwards between the middle turbinate medially and the residual uncinate process laterally. The agger nasi cells have to be completely removed. After identifying the frontal opening the, cells around the frontal recess are removed completely. The mucous membrane is preserved as much as possible, otherwise stenosis may occur. Postoperative evaluation was done at 3rd week, 3rd months and 6th month. Postoperative success rate of present study was compared with other studies (Table 4).
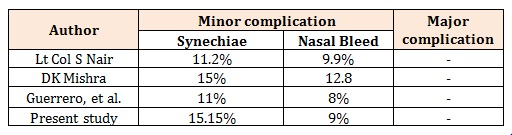
The complications of FESS are limited and classified as nasal, orbital and intracranial with intranasal synechiae as the most common complication encountered in various studies. In our series we did not have major complications and postoperative synechiae was the most common problem, encountered in 5 (15.15%) patients. These were easily cleared by systematic postoperative meticulous cleaning of the nasal cavity under endoscopic guidance. Minor complications like nasal bleeding were occasionally encountered in 3 (9.09%) patients who were treated conservatively with packing and did not require blood transfusion. This is comparable with other studies (Table 5).
Although success rates for treating sinus disease with endoscopic sinus surgery are generally high, some procedures fail and require additional management. Failure is best managed by trying to determine the cause. It should first be determined whether the sinus problem was caused by polyposis, infection, or both; the possible reasons for failure should then be considered. The possible reasons for failure in the patient with polyposis include inadequate removal, postoperative infection, or systemic disease. The possible reasons for failure in the patient with chronic infection include retained infection, adhesions, ostial obstruction, ciliary dysfunction, an unusual infectious agent, chronic rhinitis, deviated septum, systemic disease, or environmental causes such as work or life-style. In the literature, revision rate of 3 to 14 % have been documented. Our study had revision rate of 15.15% with 2 cases of polyp recurrence and 3 cases of persistent anterior nasal discharge. This is comparable with other studies; Lt Col S Nair, et al. - 8.7%, Senior BA, et al. [8] 18%, T Shiva kumar, et al. – 13.33%. In our study 84.84 % of patients were symptom free with very good relief at the end of 6 months follow up, requiring no medical treatment after the initial postoperative period. The overall improvement of present study is compared with other studies (Table 6).
Conclusion1. The pre-operative NCCT of the nose and paranasal
sinuses not only showed extent of disease involved
but was also used as road map to surgery.
2. Overall improvement was 84.84 % in our study. Thus
we concluded that FESS is an excellent method of
treatment for CRS.
3. We concluded that complications of FESS are minimal
when performed by experienced surgeon.
4. We concluded that FESS is the procedure with
minimal to mild discomfort to patient.
1. Ethical approval: This article does not contain any
studies with animals performed by any of the authors.
2. Informed consent: Informed consent was obtained
from all individual participants included in the study
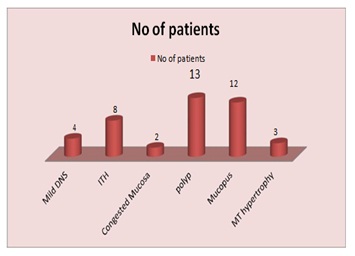
Figure 1: Anterior rhinoscopy finding.
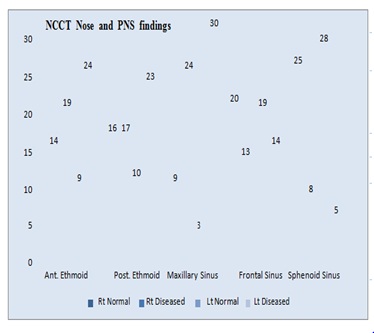
Figure 2: NCCT nose and PNS findings.
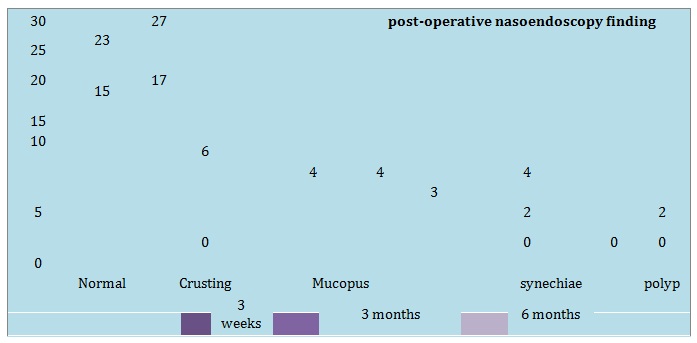
Figure 3: Post-operative naso-endoscopic findings.
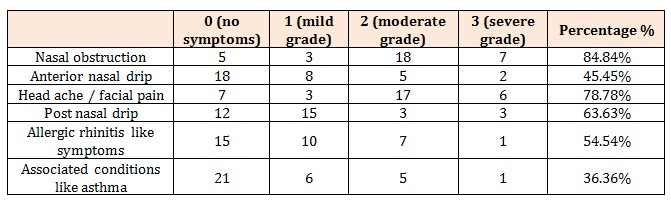
Table 1: Pre operative symptoms profile score.
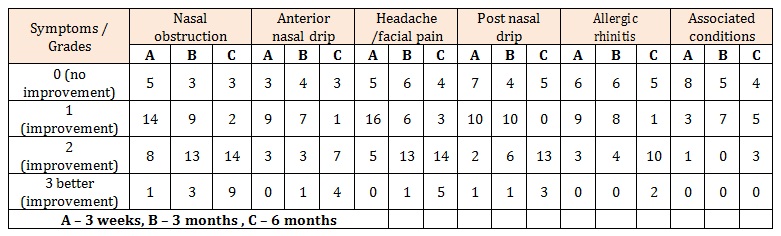
Table 2: Post operative symptom profile score.
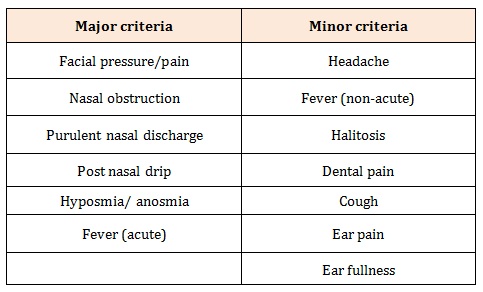
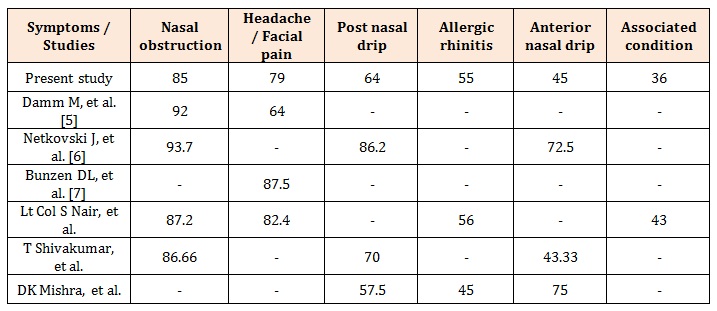
Table 3: Comparison of preoperative symptoms profile score





Chat with us on WhatsApp