Citation: Caravaca GA, et al. Glossal Abscess Secondary to a Fish Bone. Otolaryngol Open Access J 2016, 1(5): 000125.
*Corresponding author: A Caravaca García, Clínica De ORL Dr. Caravaca, C/. Radio Algeciras 5-1º E, 11201 Algeciras, Cádiz, Spain, Email: acaravacag@gmail.com
We present a case of glossal abscess following an accidental injury with a fish bone. The incidence of glossal abscesses is low. This pathology is usually the consequence of a direct trauma, and the most common location is in the anterior tongue.
Keywords: Tongue; Abscess; Organic foreign bodies
The rareness of glossal abscesses became apparent as the lack of clinical descriptions in a specialised search of the literature [1-7]. Organic foreign bodies are commonly found by ENT surgeons into the emergency room. A fish bone was found in the tongue of a patient, which was easily removed. The unusual location and course of the patient, lead us to perform a review of glossal abscesses secondary to organic foreign bodies, recommend an adequate management of these, and other related pathologies.
Case ReportA thirty-year-old male without any previous medical history came to the accident and emergency department, at the General Hospital of the main city of this area. He complained of mouth pain. There was a large tuna fish bone on the mid right dorsal border of the tongue, which was removed. A few days later, he represented with a painful swelling of the tongue. A glossal abscess was aspirated with a large bore needle. An oral wide spectrum antibiotic and a non-steroidal anti inflammatory drug were prescribed. Two weeks later he returned with an increased tongue swelling without compromising the airway which showed a deep lesion in the lingual muscle (Figure 1&2) to the left of the midline Under general anaesthesia a wide incision of the lesion on the ventral tongue the direction of Wharton’s and further dissection of the former abscess opening. A silicone drain was left in place and the incision closed by three stitches. The patient improved a few hours after, and the episode resolved completely without any further complications (Figure 3&4).
DiscussionGlossal abscesses are not usual infections [1-7] and the unilateral presentation is especially rare [4]. This type of pathology may occur at any age [1,2,4], but is more frequent when affecting middle-age-male smokers without a good dental care [5,6]. It may also be the result of a previous trauma [4], bites foreign bodies including piercing [4], dental caries, stomatitits of the lingual tonsil, thyroglossal duct, and secondary to other unknown aetiology [1,3,4]. In our case, the evident relationship with a foreign body was stated from the beginning of the process. Nevertheless, the big size of the fish bone piece was not taken into account until the appearance of the abscess signs. Bacteria are usually involved in this process [1,7] being the most frequent the streptococcus viridians, anaerobic streptococcus, staphylococcus aureus, anaerobic bacterioides and klebsiella pneumoniae. In this case, there was no positive growth on the microbiological cultures. Clinically speaking, the course of the glossal abscesses might be dramatic, starting with unspecific discomfort that may progress to odynophagia dysphagia, syalorrea and glossodynia. Changes in glossal size and lingual protrusion may also appear, compromising the air way until becoming a vital emergency [1,2,4,5]. The clinical examination may display a wide spectrum of signs, such as inflammation, indurations, edema, with or without general increase of body temperature and/or blood changes (leucocytosis) [1]. The differential diagnosis includes vascular processes, tumours, cysts and amyloidosis [7]. Investigations in the management of these and other related processes include: ultrasonography [6], CT scan [1-4,7], NMR [1,4], and aspiration and sample culturing [1-3,7].
Either, surgical treatment by incision and drainage to the proximal lesion edge or punctioning with a large bore needle (much more in cases of abscesses located anterior to the circumvallate papillae could satisfactorily solve the process. In addition, airway control is essential, including tracheostomy when required [1-4]. Antibiotic prophylaxis, covering the most common pathogens may be recommended until the specific culturing results can be obtained. It has to be emphasized that sampling methods and the local flora may easily lead to contamination where the process takes place, leading to a more severe clinical manifestations of the initial ones.
ConclusionWe have decribed a case of glossal abscess with recurrence, probably due to a gap between the first approach to the diagnosis and the second clinical examination. The large size of the fish bone was not taken into account.
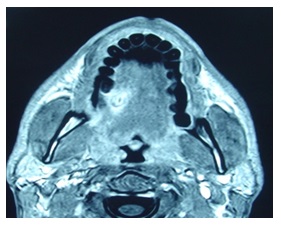
Figure 1: Nuclear Magnetic resonance of the lesion in the right sided tongue.
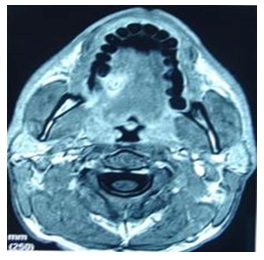
Figure 2: More posterior imagine of the lesion.

Figure 3: Intraoperatorie view of the fish bone (arrow).

Figure 4: The fish bone near to a forceps.





Chat with us on WhatsApp