Citation: Gyebre YMC, et al. Chronic laryngitis in CHU Yalgado Ouedraogo: Epidemiological and Diagnostic Aspects. Otolaryngol Open Access J 2016, 1(8): 000145.
*Corresponding author: Yvette Marie Chantal Gyebre, MCA En ORL/CCF, Service d'ORL et de CC-F, CHU-YO, Ouagadougou, Burkina Faso, West Africa, Tel: +226 70 10 88 93; Email: ycgyebre@gmail.com
Introduction: The chronic laryngitis is a persistent inflammation evolving since more than 2 weeks of the laryngeal mucosa. The possible degeneration of the white forms constitutes the haunting of the practitioner. The objective is to study epidemiological profile and diagnosis of the chronic laryngitis in the ENT department and CCF Yalgado Ouedraogo.
Methods: This is acted retrospective descriptive study from the files of patients admitted for chronic laryngitis in the ENT and CCF department of CHU Yalgado Ouedraogo of Ouagadougou from January 2010 to December 2014.
Results: In 5 years, 56 cases of chronic laryngitis were collected with an annual average of 11.2 cases. The female sex was predominant in 62.5% of cases. The average age was 41.7 years. The professionals of the voice were the most concerned in 25.5% of cases. Risk factors are frequently found and varied, dominated by atopy 23, 2% of cases. The master symptom was dysphonia in 94.7% of patients. The average time of consultation was 1.01 year. We found 96.4% of cases of nonspecific chronic laryngitis with a predominance of red laryngitis in 85.7% of cases. The lessons likely to degenerate (dysplasia) were found in 7.1% of cases. The specific chronic laryngitis were noted in 3.6% of cases.
Conclusion: The chronic laryngitis are the fact of the adult, the most often professional of the voice. They are frequently related with risk factors that should always be sought. Their early diagnosis the education of populations and the raising of the technical plat.
Keywords: Computerized Tomography; Temporal bone; Cholesteatoma; Ossicular integrity; Granulations; Facial canal dehiscence
The chronic laryngitis corresponds to the persistent inflammation of the laryngeal mucosa [1]. This is a relatively common condition. According to Babin, et al. [1] in Francea pharyngolaryngeal complaint in five is associated with chronic laryngitis, noting the importance of this disease in daily practice [1]. There are at etiopathogenic plan, two (02) leading chronic laryngitis groups: specific chronic laryngitis and non-specific chronic laryngitis often multi factorial. They are red or white certain white laryngitis are associated with variables developments whose a possible malignant transformation [1,2]. The aim of this work was to study the profile epidemiology and diagnosis of this disease in the CCF and ENT department of CHU Yalgado Ouedraogo of Ouagadougou.
Materials and MethodsWe conducted a retrospective study out of 5 years from January 2010 to December 2014 in the ENT department of Yalgado Ouedraogo. It concerned all patients in whom the diagnosis of chronic laryngitis was laid during this period. Only patients with a exploitable clinical file were retained for the study. We are interested at the following parameters: - Epidemiological including the age, sex, occupation, history, the consultation delai-Clinics and paraclinics: the diagnosis is suspected or established by after a full clinical examination including indirect laryngoscopy and / or nasal endoscopy. The direct laryngoscopy followed by a resection of suspicious lessons was required in some of our patients. Other tests have been practiced according to the context: the prick test, radiography of the paranasal sinuses (incidence Blondeau), searching for acid-fast bacillus and gastroscopy.
ResultIn 5 years, 56 cases of chronic laryngitis were recorded in the service or a hospital frequency of 11.2 cases / year. The average age of patients was 41.7 years with of extremes from 7 and 79 years. The modal class was that of 40 to 50 years with a frequency of 26.8%. We noted a female predominance 62.5% with a sex ratio of06. The voice professionals have constituted the socioprofessional group the most representative, or 25.5% of the cases as indicated in the (Table 1).
The teachers account for 65% (09 cases) of voice professionals. The (Figure1) shows the distribution of voice professionals.
The most frequent risk factors were atopy 23.2% followed of gastro-oesophageal reflux (GERD) 16.1%. The (Figure 2) presents the factors of risk of chronic laryngitis.
The average time for consultation specialized in ENT was 1 year with extremes of 1 month and 3 years.
We have listed several motives of consultation among which dysphonia in 94.6% of cases, cough (12.5%), dysphagia (10.7%), the hemmage (5.4%), dyspnea (1.8%), foreign body sensation (1.8%). In the plan physical, the indirect laryngoscopy, performed in 25 cases (44.6%) has allowed to see the inflammation of the larynx (laryngitis catarrhal in 14 cases, laryngitis pseudomyxoematous in 1 case and was not contributory in 9 cases). The nasal endoscopy was performed in 41 cases (73.2%) and allowed to visualize the inflammatory lesions of the larynx (laryngitis catarrhal laryngitis pseudomyxoematous, hypertrophic laryngitis) in all cases and 02 cases of laryngitis leukoplakic.
The direct laryngoscopy was conducted in 11 cases (19.6%). It allowed confirm inflammation of the larynx and make biopsies. The pathological examination found three (03) cases of moderate dysplasia, (01) cases of severe dysplasia and (01) of mycelial filaments. The prick test performed in 5 patients (8.9%) helped to objectify an allergy or sensitization to pollens, dust mites and mildew in 4 cases. A radiograph of the face of sinus showed the bilateral maxillary sinusitis in 3 cases. The sputum examination looking for acid-fast bacillus (AFB), performed in a patient with dysphonia, cough, and dysphagia dragged with that on indirect laryngoscopy a "dirty" aspect of the larynx, proved positive. It was laryngeal tuberculosis associated with pulmonary tuberculosis. The gastroscopy performed in a patient has allowed objectifying an esophageal-gastric ulcer. After the clinical and Paraclinical examinations, the both types anatomical and clinical classical of non-specific and specific chronic laryngitis were found as shown in the (Table 2).
CommentsThe chronic laryngitis are relatively frequent in our practice, a hospital rate of 11.2 cases / year. Our results are lower than those observed by several authors [3,4]. This finding could be explained by under reporting of cases. Infact patients do not always consult in health services for a single voice disorder (main sign of chronic laryngitis). More practical deficiency of certain examinations of the larynx (nasofibroscopy, direct laryngoscopy) is another explanation.
The average age was 41.7 years with a female predominance of 62.5%. Our results are comparable to conventional data. Indeed, chronic laryngitis especially nonspecific can occur at any age but preferably between 45 and 65 years with a female predominance [1]. The professionals of the voice were most affected by chronic laryngitis with 25.4% of cases. The teachers predominated in 64.3% of cases or 16.4% of all occupations in our series. This could be linked to overwork and / or vocal consecutive malmenage at the use of voice main way work in this sector [5,6]. The contributing factors of chronic laryngitis are numerous whose classically the tobacco and alcohol poisoning. Note also the atopy, GERD. In our series, the atopy was the leading contributing factors with 23.2%. The role of allergy in the development of chronic laryngitis was mentioned by some authors [1,7].
But we believe that this role is unclear. Indeed if the allergic rhinitis is known, it is not the same with laryngitis or pharyngeal allergic laryngitis. But the uniqueness anatomophysiological airway explains the reactions of allergic type in the larynx. When the need to seek potential allergens or irritants a view to their eviction. The GERD was found in 16.1% of cases. Our results are lower than those of some authors [4,8] who found themselves respectively 59% and 79% of GERD in their study. Our results could be partly explained by the existence of asymptomatic GERD. On the other hand the absence of esophageal pH metry and esophageal scintigraphy in our context constitutes a diagnostic limit of GERD. In fact number of studies have demonstrated by simultaneous recording of esophageal and pharyngeal pH than stomach acid could date back in GORD to the larynx causing of this fact a chronic laryngitis [4,8,9]. For our part, we believe that the GERD should be systematically sought in the chronic laryngitis. The mean delay to consultation of chronic laryngitis in our series was about 12 months. Several reasons could explain this long duration evolution. First the ignorance of the population about the disease, on the other hand financial inaccessibility002EIndeed there do not exist third party payer for health. Furthermore the importance of selfmedication and weight of traditional treatment are still not negligible in our context. The dysphonia constituted the main motive for consulting in 94.6% of cases. We agree with the literature that the vocal cords are preferentially affected in chronic laryngitis [1,2].
The indirect laryngoscopy (LI) made in 44.6% of cases, should be systematic. His practice has to be mastered by any ENT practitioner in our context in medicalized. The nasal endoscopy was effected for 73, 2% of cases. It therefore complete the LI [10,11]. It should be available in the service because it is an important tool in the exploration of chronic laryngitis. The direct laryngoscopy (LDS) was practiced in only 12 cases (21.4%). Several authors [4,12] relate the importance of this examination in the diagnosis and treatment of chronic laryngitis. This feeble attainment of the LDS with biopsy in our context could be explained by the high frequency of chronic laryngitis catarrhal in our series whose evolution is generally favorable with adequate medical treatment [12]. Among the results of histological examination, we found 03 cases of moderate dysplasia and 01 cases of severe dysplasia. These results attest to the importance of biopsy before of the suspicious lesions dysplastic and monitoring of cases of chronic laryngitis that are at potential of malignant degeneration. The chronic nonspecific laryngitis were majority in 96.4% of cases, with a predominance of red catarrhal laryngitis 60.7%. This finding could be explained by the frequent irritation of the mucous membranes of the upper aero digestive tract by dry, dusty harmattan winds that characterize the climate of our country.
ConclusionThe Chronic laryngitis is relatively frequent in our practice. It is the fact of the adult, professional of the voice in particular teacher. It is frequently linked with many risk factors which must be known to search. Its early diagnosis involves therapeutic education and the raising of the technical plateau.
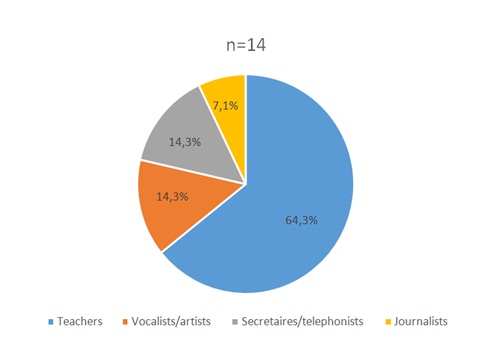
Figure 1: Distribution of Voice Profession.
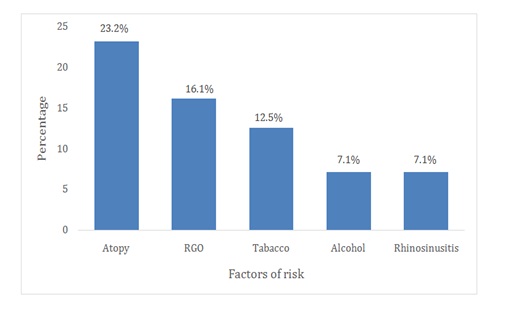
Figure 2: Risk factors of chronic laryngitis.
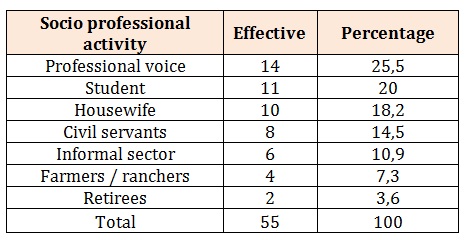
Table 1: Distribution of patients according the profession (n = 55).
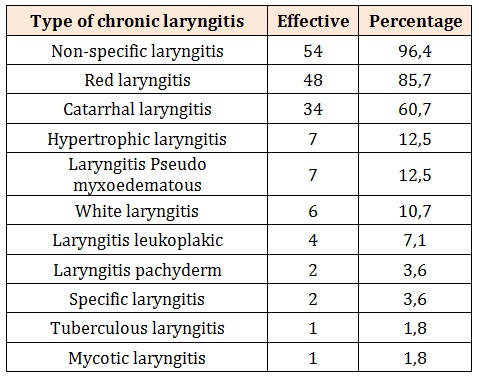
Table 2: Distribution of patients according to the type of chronic laryngitis.




