Stress Response in Surgery, Anesthetics Role and Effect on Cognition: A Review
The stress response to surgery, critical illness, trauma, and burns is characterized by derangements of metabolic and physiological processes which in turn activate the inflammatory, hormonal (sympathoadrenal), immunological, and genomic responses. The surgery-induced stress response is almost similar to that triggered by traumatic injuries; however the duration of the stress response varies according to the severity of injury. Although the stress response to acute trauma evolved to improve chances of survival following injury, in modern surgical practice the stress response can be detrimental.
Introduction
After surgical or accidental trauma, the nervous system activates the stress response by sending impulses from the injured site to the hypothalamic-pituitary-adrenal axis [1]. Activation of the hypothalamic-pituitary-adrenal (HPA) axis is a critical feature of the coordinated physiological response to surgical trauma [2, 3]. Dysregulation of the HPA axis profoundly affect perioperative response despite that perioperative focus on this neuroendocrine response has largely been restricted to glucocorticoid physiology. Acute and chronic disruption of the HPA axis impairs the ability to rapidly respond to initial and sequential perioperative stressors. Several factors modulate the perioperative stress response, as characterized by changes in cortisol physiology. The aim of this review was to examine the complex interaction between stress response to surgery, anesthetics role and impact on cognition by reviewing available literature on this issue.
Hypothalamic-Pituitary-Adrenal Axis
Surgical trauma activates the sympathetic autonomic nervous system via neurophysiological pathway which stimulates the hypothalamus. Paraventricular nucleus (PVN) of the hypothalamus is central regulator of this axis and is a major relay for afferent information from limbic areas of the CNS that can detect cognitive and emotional stressors, and physiological changes [2]. Corticotrophin-releasing hormone (CRH) is then released into the hypophyseal portal plexus and binds to CRH receptors on corticotropes in the anterior pituitary gland to release the adrenocorticotropic hormone (ACTH). Vasopressin, released from the posterior pituitary and reaching the corticotroph cells in the anterior pituitary also has an endocrine function, as it stimulates secretion of pro-opiomelanocortin from the anterior pituitary gland in conjunction with CRH which is a key component of the stress response to acute stimuli and stimulates the release of ACTH via the vasopressin-3 receptor. ACTH is released via exocytosis into the systemic circulation where it primarily acts on the melanocortin-2 receptors in the zona fasciculata of the adrenal cortex to synthesize glucocorticoids that are then released into the circulation, the most significant of which is cortiso [4].
Carrier proteins, mainly cortisol-binding globulin (CBG) and, up to some extent, albumin, prevent cortisol from diffusing into cells in target tissues, with only ~5% of the circulating cortisol in its active form [5]. Increased free cortisol levels are paralleled by reductions in carrier proteins, and at sites of inflammation, activated neutrophils cleave CBG, which further increases the local active cortisol concentrations [6].
The basic peripheral and neurophysiological pathways underpinnings fostering the neuroendocrine response to surgical tissue trauma is shown in Figure 1. Elevations of cortisol, glucagon, catecholamine, and a host of inflammatory cytokines, exacerbate the stress response to surgery leading to increased sympathetic activity expressed as tachycardia, hypertension, raised cardiac output and increased myocardial contractility.
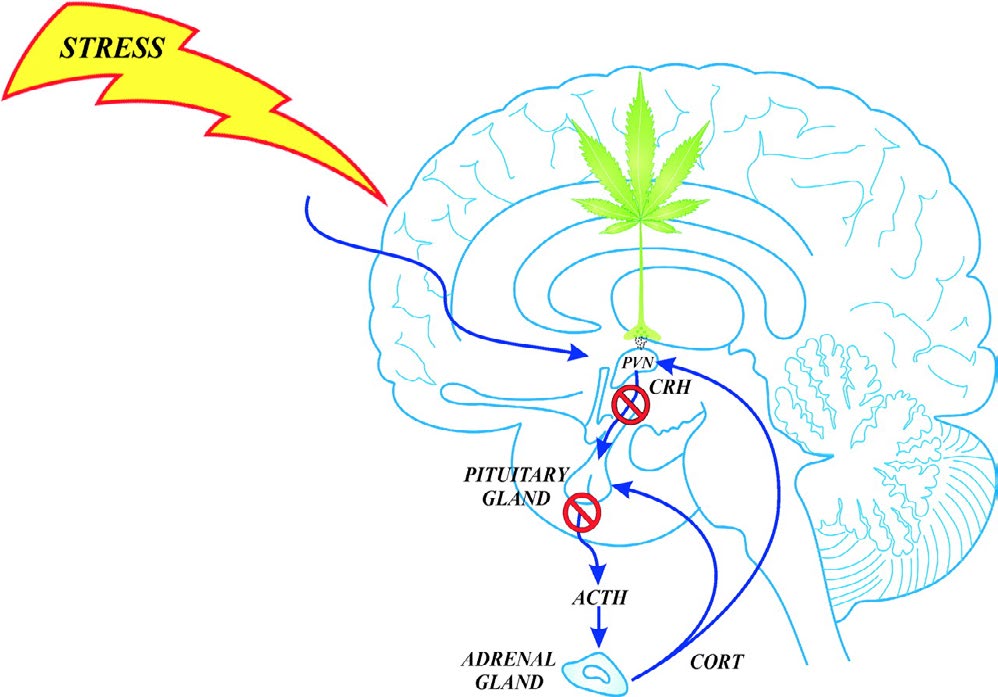
Figure 1: Rapid glucocorticoid feedback inhibition of the HPA axis [7]. Glucocorticoids (CORT) are secreted into the blood from the adrenal glands in response to stress activation of the HPA axis, and the circulating glucocorticoids feed back to the anterior lobe of the pituitary gland, the hypothalamic PVN, and the hippocampus. Glucocorticoids inhibit CRH neuron activity via endocannabinoid release in the PVN and curtail HPA hormone release within minutes of reaching the PVN.
Effect of anesthesia on the stress response to surgery
The response to surgical anaesthesia depends on type of surgery, type of anaesthesia and patient. Anaesthesia can affect or modulate the stress response via afferent blockade, central modulation and peripheral interaction. Anesthesia exerts a variable action on hypothalamic, pituitary and adrenal hormonal secretion although it has little effect on the cytokine response to surgery because it cannot influence tissue trauma [8].
General Anaesthesia
Surgical stress or nociception level is evaluated by blood levels of ACTH, cortisol, epinephrine, norepinephrine and PRL during surgery. Most of drugs used, including neuroleptic drugs, opioids, thiopentone, propofol and sevoflurane have been found to stimulate PRL release during anesthesia [9, 10]. Fentanyl suppressed ACTH and cortisol secretion when administered before surgical incision in patients undergoing pelvic surgery, but not when given after the start of surgery [11]. Complete inhibition of the stress response using high doses of fentanyl resulted in severe postoperative respiratory depression in patients undergoing open cholecystectomy [12]. This shows opioids seem to suppress cortisol production at high dose. Effects of propofol on the synpathoadrenal system are well documented [13, 14]. A single induction dose of propofol can suppress cortisol but it do not block cortisol and aldosterone secretion in response to surgical stress. Continuous infusion of propofol, at deep anesthesia doses, completely abolished circulating cortisol secretion during surgery [13]. In laparoscopic surgery, the type of volatile anesthetic significantly also affects the stress response, sevoflurane when compared to isoflurane significantly decreased plasma concentrations of ACTH, cortisol and GH [15].
Stress hormones and cognition
The long-term memory mainly takes place in the hippocampus and neocortex. Identification of the mechanisms by which stress modulate hippocampal function has been the subject of intense interest. High level of cortisol can modulate the functional status of memory circuit of hippocampus and neocortex16 and have profound inhibitory effect on hippocampal cells activity is predicted. Another neuroendocrine mediator of stress, prolactin (PRL), also involved in modulating memory functions increases the expression of corticotrophin releasing hormone (CRH) which has been shown to enhance learning through hippocampal CRH-R1 regardless of its indirect attenuation of stress- induced hypothalamo-pituitary-adrenal (HPA) axis activity [16, 17]. Inhibition of ACTH-stimulated production of cortisol by anesthetic drugs has been seen variably in many clinical studies while a marked increase in PRL concentrations were observed independently of the anesthetic procedure [18, 19]. Within the central nervous system (CNS), two kinds of receptors are activated by cortisol: so-called glucocorticoid receptors (GRs; type II), and mineralocorticoid receptors (MRs; type I). When a neuron contains receptors of both types, as many within the hippocampus do, cortisol level affects the hippocampal function in an inverted U-shaped fashion [20].
It is well known that there are no direct methods to measure stress level during general anaesthesia. The common measured signs of autonomic reactions, such as blood pressure or heart rate, have been used for assessing stress level during anaesthesia, accepting their low specificity. Some electroencephalographic (EEG-) derived variables, such as entropy22 and bispectral index23, are useful for monitoring depth of anaesthesia and preventing conscious recall but they do not always indicate inadequate analgesia and should be interpreted carefully during anaesthesia. The so-called surgical pleth index (SPI), a novel multivariate index using two continuous derived cardiovascular variables, has been proposed as a method to evaluate intraoperative stress level during general anaesthesia and a moderate correlation to the stress hormones (ACTH, cortisol, epinephrine, and norepinephrine) has been found during general anaesthesia in a recent study [21, 22, 23, 24].
Regional Anaesthesia
In lower abdominal and lower limb surgeries perioperative stress response is blocked by epidural as well as spinal anaesthesia. Afferent impulses from the site of surgery travel to the hypothalamic- pituitary axis and efferent impulses to the liver and adrenal medulla get blocked. Patients undergoing hysterectomy, epidural block dermatome level T4 to S5 before the start of surgery and thus prevent increase in cortisol level [25, 26]. However in thoracic or upper abdominal surgeries even an extensive epidural blockade cannot prevent the neurohormonal stress response to surgery.
Conclusion
Anaesthetic drugs exert a variable action on response of HPA axis to surgical trauma and only little effects on cytokine production linked to tissue trauma. This review of literature of cortisol response during surgery demonstrated significant differences of cortisol response in relation to the surgery and anaesthetic technique. It is essential to blunt the stress hormones secretion in order to prevent postoperative complications, such as PTSD, POCD and delirium. For perioperative stress response currently cortisol measurements are based mainly on robust assay techniques that represent biologically relevant cortisol levels. The gold standard technique for measurement of free cortisol, liquid chromatography/tandem mass spectrometry (LC/MS), Taylor AE, et al. [25] has been used in only two of
71 perioperative studies. Large prospective studies, entailing rigorous patient selection, stratification and standardized outcome measurement by LC-MS/ MS, are needed to clarify how the adrenal gland responds to surgery and which factors shape this response. Up to date, there is not a safe method to discriminate if response to stress is suppressed under anaesthesia; however, the use of drug at dose known to produce adequate anaesthesia and the support of neuro- monitoring may help to prevent an excessive HPA axis activation. There is need of a refined, stratified approach for understanding the stress response to surgery at the molecular and organ levels and to modify therapeutic in response to physiological response to surgery.
References
-
Desborough JP (2000) The stress response to trauma and surgery. Br J Anaesth 85(1): 109-117.
-
Miller T, Gibbison B, Russell GM (2017) Hypothalamic- pituitary-adrenal function during health, major surgery, and critical illness. BJA Educ 17(1): 16-21.
-
Gibbison B, Angelini GD, Lightman SL (2013) Dynamic output and control of the hypothalamic-pituitary- adrenal axis in critical illness and major surgery. Br J Anaesth 111(3): 347-360.
-
Herman JP, McKlveen JM, Ghosal S, Kopp B, Wulsin A, et al. (2016) Regulation of the hypothalamic-pituitary- adrenocortical stress response. Hoboken, NJ: John Wiley & Sons 6(2): 603-621.
-
Lewis JG, Bagley CJ, Elder PA, Bachmann AW, Torpy DJ (2005) Plasma free cortisol fraction reflects levels of functioning corticosteroid-binding globulin. Clin Chim Acta 359(1): 189-194.
-
Henley DE, Lightman SL (2011) New insights into corticosteroid-binding globulin and glucocorticoid delivery. Neuroscience 180: 1-8.
-
Tasker JG, Di S, Malcher-Lopes R (2006) Minireview: rapid glucocorticoid signaling via membrane-associated receptors. Endocrinology 147(12): 5549-5556.
-
Kahveci K, Ornek D, Doger C, Aydin GB, Aksoy M, et al. (2014) The effect of anesthesia type on stress hormone response: comparison of general versus epidural anesthesia. Niger J Clin Pract 17(4): 523-527.
-
Mujagic Z, Cicko E, Verag-Brozovic V, Prašo M (2008) Serum level of cortisol and prolactin in patients treated under total intravenous anesthesia with propofol- fentanyl and under balanced anesthesia with isoflurane- fentanyl. Cent Eur J Med 3: 459-463.
-
Hall GM, Young C, Holdcroft A, Alaghband-Zadeh J (1978) Substrate mobilisation during surgery. A comparison between halothane and fentanyl anaesthesia. Anaesthesia 33(10): 924-930.
-
Bent JM, Paterson JL, Mashiter K, Hall GM (1984) Effects of high-dose fentanyl anaesthesia on the established metabolic and endocrine response to surgery. Anaesthesia 39(1): 19-23.
-
Klingstedt C, Giesecke K, Hamberger B, Järnberg PO (1987) High- and low-dose fentanyl anaesthesia: circulatory and plasma catecholamine responses during cholecystectomy. Br J Anaesth 59(2): 184-188.
-
Jung SM, Cho CK (2015) The effects of deep and light propofol anesthesia on stress response in patients undergoing open lung surgery: a randomized controlled trial. Korean J Anesthesiol 68(3): 224-231.
-
Kaushal RP, Vatal A, Pathak R (015) Effect of etomidate and propofol induction on hemodynamic and endocrine response in patients undergoing coronary artery bypass grafting/mitral valve and aortic valve replacement surgery on cardiopulmonary bypass. Ann Card Anaesth 18(2): 172-178.
-
Marana E, Colicci S, Meo F, Marana R, Proietti R (2010) Neuroendocrine stress response in gynecological laparoscopy: TIVA with propofol versus sevoflurane anesthesia. J Clin Anesth 22(4): 250-255.
-
Payne JD, Nadel L (2004) Sleep, dreams, and memory consolidation: the role of the stress hormone cortisol. Learn Mem 11(6): 671-678.
-
Radulovic J, Rühmann A, Liepold T, Spiess J (1999) Modulation of learning and anxiety by corticotropin- releasing factor (CRF) and stress: differential roles of CRF receptors 1 and 2. J Neurosci 19(12): 5016-5025.
-
Croiset G, Nijsen MJ, Kamphuis PJ (2000) Role of corticotropin-releasing factor, vasopressin and the autonomic nervous system in learning and memory. Eur J Pharmacol 405(1-5): 225-234.
-
Donner N, Bredewold R, Maloumby R, Neumann ID (2007) Chronic intracerebral prolactin attenuates neuronal stress circuitries in virgin rats. Eur J Neurosci 25(6): 1804-1814.
-
Pavlides C, McEwen BS (1999) Effects of mineralocorticoid and glucocorticoid receptors on long-term potentiation in the CA3 hippocampal field. Brain Res 851(1-2): 204- 214.
-
Takamatsu I, Ozaki M, Kazama T (2006) Entropy indices vs the bispectral index for estimating nociception during sevoflurane anaesthesia. Br J Anaesth 96(5): 620-626.
-
Chen X, Thee C, Gruenewald M, Ilies C, Höcker J, et al. (2012) Correlation of surgical pleth index with stress hormones during propofol-remifentanil anaesthesia. Scientific World J 879158.
-
Aceto P, Perilli V, Lai C, Sacco T, Ancona P, et al. (2013) Update on posttraumatic stress syndrome after anesthesia. Eur Rev Med Pharmacol Sci 17: 1730-1737.
-
Bruhn J, Myles PS, Sneyd R, Struys MM (2006) Depth of anaesthesia monitoring: what’s available, what’s validated and what’s next? Br J Anaesth 97(1): 85-94.
-
Taylor AE, Keevil B, Huhtaniemi IT (2015) Mass spectrometry and immunoassay: how to measure steroid hormones today and tomorrow. Eur J Endocrinol 173(2): D1-12.
-
Enquist A, Brandt MR, Fernandes A, Kehlet H (1977) The blocking effect of epidural analgesia on the adrenocortical and hyperglycaemic responses to surgery. Acta Anesthesiol Scand 21(4): 330-335.
- Editorial on Multimodal Analgesia
- Surgical Incision Site Local Anaesthetic Infiltration and Superior Hypogastric Plexus Block in Total Abdominal Hysterectomy Under General Anaesthesia- A Placebo-Controlled, Randomized Clinical Trial
- Supraglottic Airway Insertion in Semi Fowler Position Due to Severe Thoracic Hyperkyphosis: A Case Report
- Anaesthetic Management of Cardiac Myxoma Patient with Systemic Involvement: A Case Report
- Current Problems in Pulmonary Respiratory Distress Syndrome (Literature Review)
- Evolution of Perioperative Hemodynamic Monitoring from the Hand on Pulse to Hypotension Prediction Index