Ultrasound as a Screening Tool to Plan Central Neuraxial Blockade for Total Hip Replacement in a Patient with Ankylosing Spondylitis: A Case Report
Patients with Ankylosing Spondylitis present unique challenges to anesthesiologists due to the fusion of their spines, making airway management and central neuraxial blockade difficult. This creates a dilemma during preoperative assessment regarding whether to plan the case in general anesthesia (GA) or regional anesthesia (RA). In our case, GA with endotracheal intubation was anticipated to be difficult due to the absence of neck motion, limited mouth opening, and restricted chest movement. Although central neuraxial blocks offer many advantages over GA, they are known to be difficult in patients with Ankylosing Spondylitis, and have been underutilized in the past. However, the possibility of avoiding GA and awake fiberoptic in an anxious patient, as well as excellent analgesia for both intraoperative and postoperative periods, prompted us to opt for RA. Despite the technical difficulty due to fused spines and obliteration of interspinal spaces, we successfully performed ultrasound-guided central neuraxial blockade for total hip replacement in this case.
Yashoda Khadka* and Basudev Parajuli
Introduction
Ankylosing Spondylitis (AS) is a chronic inflammatory disease that causes stiffening of the joints and ligaments [1]. One of the effective treatment strategies for AS is hip replacement surgery [2], which can help relieve pain and restore functional capabilities. However, AS presents several anesthetic implications that must be considered by anesthesiologists. Patients with AS have an increased risk of vertebral fragility fractures and atlantoaxial subluxation. Moreover, AS can create significant challenges for anesthesiologists due to potential difficulties with airway management, cardiovascular and respiratory complications and consequences of medications used to reduce pain and control the disease [3]. Patients with AS may also experience stiffness of the cervical spine, atlanto-occipital, temporomandibular, and cricoarytenoid joints, which can cause difficult intubation. Adequate and proper planning is essential prior to surgery to manage these challenges during the perioperative period.
Case Report
A 54-year-old male with a known history of severe Ankylosing spondylitis (AS) presented for left total hip replacement (THR). The patient had a Basal metabolic index (BMI) of 32.9 kg/m2, restricted movement in the thoracolumbar and cervical spine, and bilateral uveitis. Airway assessment revealed a difficult airway with limited

mouth opening, Mallampati grade 3, multiple absent teeth, and absence of mobility of cervical joint. Radiological studies showed solid ankylosis of the facet joints between the second and fifth cervical vertebrae, obliteration of most of the lumbar facet joints, bridging syndesmophytes between all lumbar vertebrae, and loss of lordosis (Figure 1). Pulmonary function test revealed a restrictive pattern, and chest X-ray revealed hyperinflated lung fields (Figure 2). The patient was evaluated for both general anesthesia (GA) and regional anesthesia (RA) with written informed consent obtained for both options.

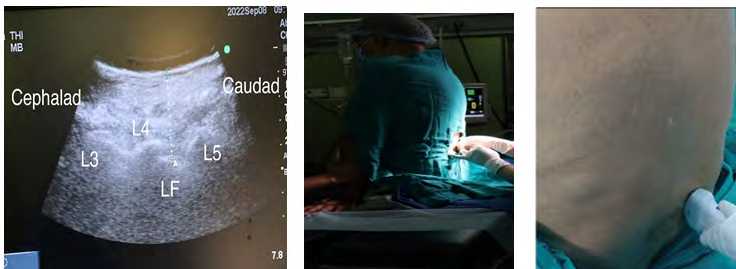
Spinal block was planned with GA as an alternative in case of difficulty or failure. The patient’s lumbar spine was scanned with a portable ultrasound unit in the sitting position with support (Figure 3). A soft tissue window was identified between the L4 and L5 vertebrae (Figure 3). On the day of surgery, dural puncture was successfully achieved with a 25-gauge Quincke’s needle on the second attempt, and 3.2 mL of 0.5% hyperbaric bupivacaine and 20 mcg of Fentanyl was injected intrathecally via a paramedian approach after the free flow of cerebrospinal fluid (CSF). The patient developed a sensory block to the T8 dermatome and motor blockade of modified Bromage grade 3 within 15 min. Surgery lasted for 2 ½ hours with hemodynamic stability throughout the intraoperative period. The patient made an excellent recovery and was comfortable during the postoperative period.
Discussion
In this case we successfully performed spinal anesthesia for a left total hip replacement in a patient with severe AS using ultrasound-guided paramedian approach. The use of ultrasound allowed for accurate identification of the L4-5 intervertebral level, which was marked on the patient’s skin for the paramedian approach. We were able to achieve dural puncture on the second attempt and successfully administered intrathecal anesthesia.
Ultrasound-guided neuraxial anesthesia has been increasingly used in recent years due to its ability to improve success rates and decrease complication rates [4, 5]. It allows for real-time visualization of the spine and surrounding structures, facilitating accurate identification of the midline and target level for needle placement. In patients with AS, where traditional landmarks may be distorted or inaccessible, ultrasound can be particularly useful in identifying the best approach for regional anesthesia [6].
While regional anesthesia may be technically challenging in patients with AS, it offers several advantages over general anesthesia, including reduced risk of airway complications and improved postoperative pain control. However, each patient must be evaluated individually, and the anesthesia plan should be tailored to their specific needs and risks.
In summary, ultrasound-guided paramedian approach for spinal anesthesia may be a safe and effective option for patients with severe AS undergoing hip replacement surgery [7, 8, 9]. It allows for accurate identification of the midline and target level, which can be particularly challenging in patients with AS. The use of regional anesthesia in these patients should be carefully evaluated based on individual risk factors and surgical requirements [10, 11].
Conclusion and Recommendation
In conclusion, patients with Ankylosing spondylitis present unique challenges for anesthesia due to their spinal column deformity, costochondral rigidity, and potential airway involvement. However, the use of ultrasound can assist in identifying the intervertebral space and help plan the mode of anesthesia, potentially decreasing the need for general anesthesia. Anesthesiologists should also be aware of the potential for difficult airway management and spinal cord injury during anesthesia in these patients. Therefore, careful preoperative assessment, planning, and intraoperative monitoring are essential. Further research may be necessary to assess the feasibility and effectiveness of ultrasound-guided techniques in these patients.
Declaration of Patient Consent
Authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/ their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
References
-
Sivrikaya GU, Hanci A, Dobrucali H, Yalcinkaya A (2010) Cesarean section under spinal anesthesia in a patient with ankylosing spondylitis. Middle East J Anesthesiol 20(6): 865-968.
-
Cesur M, Alici HA, Erdem AF (2005) An unusual cause of difficult intubation in a patient with a large cervical anterior osteophyte: a case report. Acta Anaesthesiol Scand 49(2): 264-266.
-
Guan M, Wang J, Zhao L, Xiao J, Li Z, et al. (2013) Management of hip involvement in ankylosing spondylitis. Clin Rheumatol 32(8): 1115-1120.
-
Woodward LJ, Kam PC (2009) Ankylosing spondylitis: recent developments and anaesthetic implications. Anaesthesia 64(5): 540-548.
-
Nalini K, Nagalakshmi NV, Gururaj, Mujeeb R (2007) A Case of Severe Ankylosing Spondylitis Posted for Hip Replacement Surgery. Indian Journal of Anaesthesia 51(6): 546-549.
-
Furness G, Reilly MP, Kuchi S (2002) An evaluation of ultrasound imaging for identification of lumbar intervertebral level. Anaesthesia 57(3): 277-280.
-
Chin KJ, Chan V (2010) Ultrasonography as a preoperative assessment Tool: Predicting the feasibility of Central Neuraxial Blockade. Anesth Analg 110(1): 252-253.
-
Karmakar MK, Li X, Ho AM, Kwok WH, Chui PT, et al. (2009) Real-time ultrasound-guided paramedian epidural access: Evaluation of a novel in-plane technique. Br J Anaesth 102(6): 845-854.
-
Jindal P, Chopra G, Chaudhary A, Rizvi AA, Sharma JP, et al. (2009) Taylor’s approach in an ankylosing spondylitis patient posted for percutaneous nephrolithotomy: A challenge for anaesthesiologists. Saudi J Anaesth 3(2): 87-90.
-
Goyal R, Singh S, Shukla RN, Singhal A (2013) Management of a case of ankylosing spondylitis for total hip replacement surgery with the use of ultrasound- assisted central neuraxial blockade. Indian J Anaesth 57(1): 69-71.
-
Woodward LJ, Kam PC (2009) Ankylosing spondylitis: Recent developments and anaesthetic implications. Anaesthesia 64(5): 540-548.
- Editorial on Multimodal Analgesia
- Surgical Incision Site Local Anaesthetic Infiltration and Superior Hypogastric Plexus Block in Total Abdominal Hysterectomy Under General Anaesthesia- A Placebo-Controlled, Randomized Clinical Trial
- Supraglottic Airway Insertion in Semi Fowler Position Due to Severe Thoracic Hyperkyphosis: A Case Report
- Anaesthetic Management of Cardiac Myxoma Patient with Systemic Involvement: A Case Report
- Current Problems in Pulmonary Respiratory Distress Syndrome (Literature Review)
- Evolution of Perioperative Hemodynamic Monitoring from the Hand on Pulse to Hypotension Prediction Index