Frequency, Outcome and Socio-Demographic Factors of Common Unintentional Childhood Poisoning, from a Tertiary Health-Care Teaching Hospital of a Low-Income Setting
Background: Poisoning ranked 2nd among commonest injury and 3rd most common pediatric ED visits. National health survey of Pakistan estimated 4.3% unintentional poising among children <5 years of age. Most studies focus on types of poisoning; only a few highlighted the factors associated with ingestion. We try to document factors behind common pediatric household unintentional poisoning from the largest tertiary care teaching hospital of the country. Methods: Descriptive case series study, with a questionnaire-based non-probability consecutive sampling, conducted at the ED of National Institute of Child Health (NICH), Karachi during 2017-2018. The sample size was 253. Inclusion criteria were children of either gender aged 12 or below with a clear history of unintentional ingestion of poison. Results: We found male predominance (52%) and the common age was below 5 years. Most children were exposed to poison either during the afternoon or by early evening (79.05%), and mother/caregiver was not present around the child in 68% of cases. In 79% of cases mothers either had tenth grade or below education. A joint family system was present in 84 % of cases. Poor family class was found in 49% of cases. The most commonly ingested poisons were drugs (33.78%). The majority of the children were admitted (60.09%). Conclusion: Socio-demographic factors have a significant effect on childhood poisoning and by addressing them we can decrease unintentional poisoning cases in children.
Introduction
Poisoning occurs when people drink, eat, breathe, inject, or touch enough of a hazardous substance (poison) to cause illness or death [1]. Unintentional ingestion/poisoning, continue to be significant injury-related morbidity and mortality across the world [2]. According to WHO (2012) data, 193,460 deaths globally resulted from unintentional poisoning and unfortunately, 84% of those were from low to middle-income countries (1). Poisoning ranked 2nd among commonest injury and 3rd most common pediatric ED visits [3]. Unintentional poisoning is implicated in about 2% of all injury-related deaths among children from developing counties [4].
Around 70% of acute poisoning occurs in the pediatric population, 90% are preventable [5]. Epidemiological properties of poisoning differ in availability, socio-economic status, age, education, large family size, religious and cultural influences etc [6]. Pediatric accidental ingestion are mothballs, flea and tick product, cleaning solutions, nail polish remover, other hydrocarbons, sanitary products and available drugs as candy [7].
Low-middle income countries in the EMRO region count mortality rates of 1.6/100,000 children, whereas for the South Asian region it was 1.7/100,000 children [8]. National health survey of Pakistan estimated 4.3% unintentional poising among children <5 years of age [9]. Children <6 years age group are more prone to poisoning with male predominate, while mortality has been reported to be from 1% to 12.5% in different studies [10]. Most studies focus on types of poisoning, only a few highlighted the factors associated with ingestion. Few epidemiological studies from Pakistan [11] and region around [12, 13] identified some of the factors associated with unintentional poisoning among children <5 years of age like overcrowding, maternal education, socioeconomic of the family, family type (nuclear or joint), number of siblings and few more.
Pakistan lack both centralize poison center and national database resources on pediatric poisoning, there are few small, single or multiple center hospital-based descriptive studies that may not reflect the actual picture of the disease magnitude and the exact nature of the problem is very difficult to ascertain from these local studies.
In this context, we try to document the key factors behind common pediatric household unintentional poisoning from the largest tertiary care teaching hospital on frequency, outcome and socio-demographic factors especially focusing on maternal education, mother on the job when the child had exposure to poison and timing of ingestion was investigated. Furthermore, we will focus on the knowledge gap and aimed to derive independent solutions to the problem.
Methods
This was descriptive case series study from cases visiting the Emergency Department of National Institute of Child Health (NICH), Karachi during 2017-2018. This study was waived for informed consent by the Ethical Review Committee of NICH. The study protocol is performed in accordance with the relevant guidelines. The study center is a public hospital where most patients are either from semi- rural or middle to low socioeconomic class. Data collection was non-probability consecutive sampling on a predesigned, tested and approved. The study center is the largest tertiary care hospital in the town with total ED turnover of >hundred thousand annually and an admission rate of 27-35%.
The sample size was calculated by using a W.H.O sample size calculator, taking confidence interval of 95% and incidence of childhood poisoning 4.3% 6 with margin of error of 2.5%, the estimated sample size was n=253. All children aged 12 or below of either gender, who visited the ED with a clear history of unintentional ingestion of any substance identified as poison, were included in the study. Children who were mentally retarded or brought dead in the ED were excluded from the study, as were the children with suicidal/ homicidal poisoning, doubtful ingestion of poison or other types of poisoning like snake or dog bites.
A patient who fulfilled the inclusion criteria was selected from a tertiary health care hospital. Confidentiality of the parents (guardian)/patients was ensured. The patient was followed till the outcome is determined. The outcome was determined in the end of 24 hours. In the end the researcher evaluated the results of the study i.e. outcome and socio- demographic factors.
Data were analyzed by using SPSS version 22. Age of patient and duration of ingestion of poison was presented as mean ± SD. Frequency and percentage were presented for the type of poisoning, absence of parent/primary caregiver, maternal education status, maternal age, maternal job, family type, family income and outcome of poisoning. The total number of family members taking medications, number of children, route of exposure to the poison, place of storage of poison, any procedure done at the hospital, and any treatment given were controlled through stratification. The study outcome was performed using Analysis of the data was done using descriptive statistics like frequencies, proportions, means, median and standard deviations, Chi- square test for categorical variables and p-value ≤ 0.05 was considered as statistically significant.
Results
Out of total ED visits we observed 253 cases with a confirmed history of poisoning and who gave consent to be enrolled in the study. There were 132 (52%) male and 121 (48%) female cases. Regarding age distribution, most were <5 years of age with a mean age of 4.41±3.31 (CI of 4.00- 4.81). Male predominate, however, females outnumber male among the age group of >10 years Table 1.
| Morning [n=21] | Afternoon [n=123] | Evening [n=77] | Night [32] | Total [n=253] | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Male | Female | Male | Female | Male | Female | Male | Female | Male | Female | |
| [n=12 | [n=0] | [n=70 | [n=53 | [n=43 | [n=24 | [n=43 | [n=24 | [n=13] | [n=11] | |
| <5 Years | 8 [66.7] | 7 [77.8] | 64 [91.4] | 48 [90.6] | 14 [32.6% | 2 [8.3%] | 14 [32.6% | 2 [8.3%] | 89 [66.4% | 70 [58.8% |
| 6-10 Years | 2 [16.7%] | 0 [0%] | 4 [5.7%] | 1 [1.9%] | 20 [46.5%] | 11 [45.8%] | 20 [46.5%] | 11 [45.8%] | 31 [23.1%] | 18 [15.1%] |
| >10 Years | 2 [16.7%] | 2 [22.2%] | 2 [2.9%] | 4 [7.5%] | 9 [20.9%] | 11 [45.8%] | 9 [20.9%] | 11 [45.8%] | 14 [10.4%] | 31 [26.1%] |
| Total | 12 [100%] | 9 [100%] | 70 [100%] | 53 [100%] | 43 [100%] | 24 [100%] | 43 [100%] | 24 [100%] | 134 [100%] | 119 [100%] |
| P-value | 0.433 | 0.294 | 0.030* | 0.039* | 0.004* |
Table 1: Age and Gender Correlation with Time of Ingestion. (P value 0.0001).
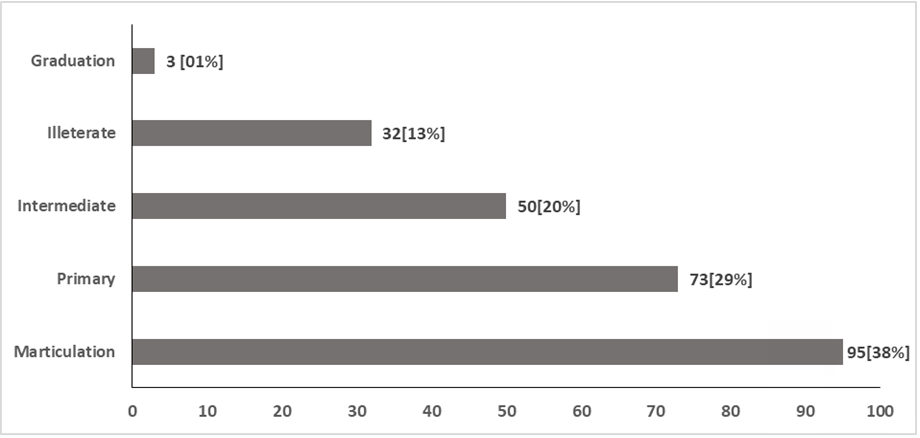
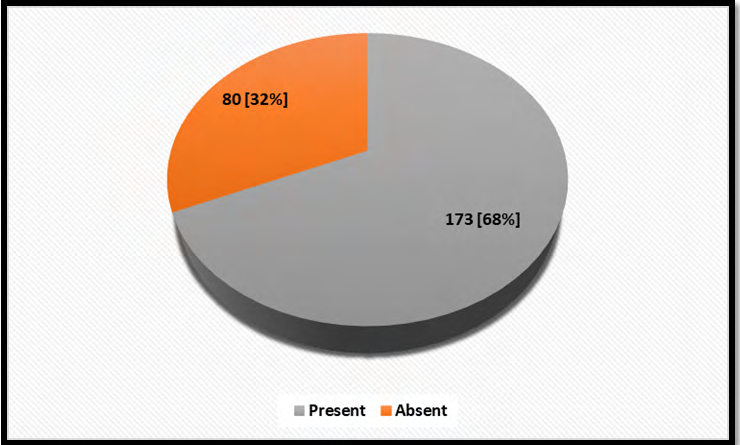
Regarding the timing of ingestion, we observe most children (<5 years) exposed during the afternoon followed by evening as in Table 1 and most of the time mother or caregiver was not present while the child exposed to poison. We found 173 (68%) children, mostly during afternoon and early evening time, whose mother was absent while the child exposed to poison, Figure 1. Maternal age directly correlates with exposure of ingestion, we found 150 (59%) mothers with age >30 years, similarly maternal educational status has a strong relationship with the exposure and we found 200 (79%) mothers either had tenth grade or minimal educational experience Figure 2.
The joint family system, number of siblings or number of family members in a house all correlates with an increased chance of exposure to poison. In our study, out of 253 children, 213 (84%) were living in a joint family system; with more than five adult member living together mostly in a small house and at least one of them was on some medications in 190 (75%) cases.
The number of children (>3) living together also impact the chance of exposure, as in our study, we found 101(40%) such children, of which 83 (82%) were when mother was on job Table 2.
| Family System | Number of Children <3 [n=152] | Number of Children >3 [n=101] | Total [n=304] | ||
|---|---|---|---|---|---|
| Mother on Job | Mother not on job | Mother on Job | Mother not on job | ||
| [n=122] | [n=30] | [n=83] | [n=18] | ||
| Joint Family System | 105 [86.1%] | 21 [70%] | 72 [86.7%] | 15 [83.3%] | 213 [79.1%] |
| Nuclear Family System | 17 [13.9%] | 9 [30%] | 11 [13.3%] | 3 [16.7%] | 40 [20.9%] |
| Total | 122 [100%] | 30 [100%] | 83 [100%] | 18 [100%] | 253 [100%] |
| P-value | 0.036* | 0.704 |
Table 2: Correlation of Family System, Working Mom and Number of Children in Family, P value 0.0001.
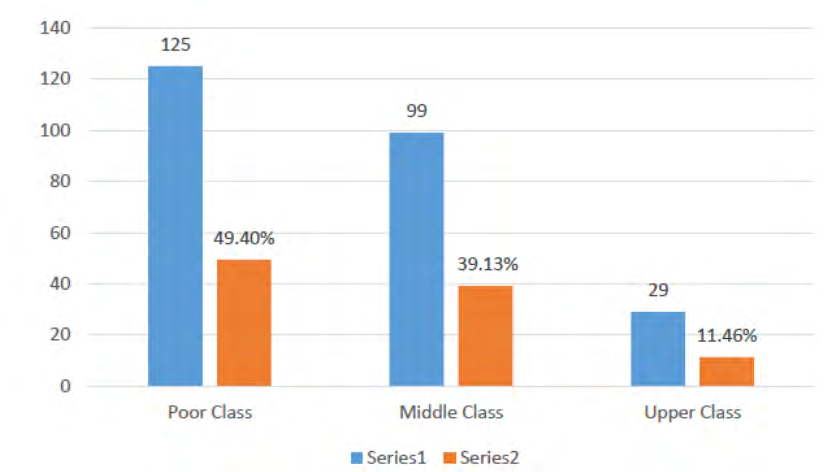
Family income and socioeconomic status, as elaborated in Figure 3, shows a considerable number of children i.e. 125 out of 253 (49%) belong to a poor family class, who earn less than ten thousand a month, though a majority of these mothers use to do some jobs 205 (81%) either at the home or outside.
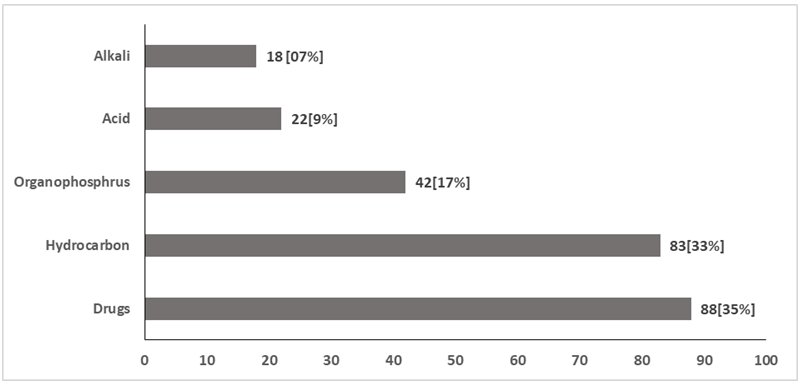
Types of common poison ingested is described in Figure 5. Commonly ingested poisons were drugs and hydrocarbon followed by organophosphorus exposure, while oral administration was the most common route with 166 cases,
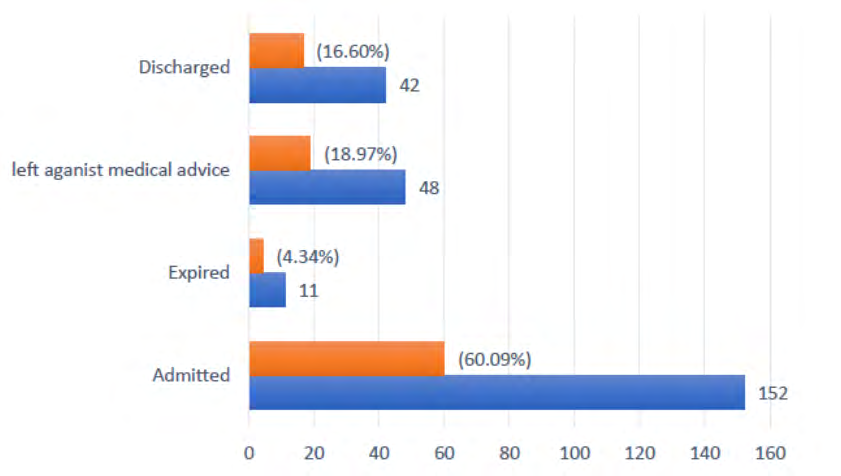
11 (4.3%) children expired, 03 (1.1%) died in ED and 152 (60%) admitted Figure 4. Almost all exposed children got these poisons kept within their reach. Lavage was carried out in 40 cases, however, induced vomiting already practiced by parents at home in 82 children.
Discussion
Accidental ingestion of a substance, injurious to health is still a common health problem among children from the developing world; however, literature is spare from South Asia including Pakistan.14 Most unintentional pediatric poisoning are preventable with little education, intervention and modification of risk factors. The study center is the largest children teaching hospital in the province which caters for patients from the whole of the city and around.
Age and Gender
Available literature from Pakistan identify that majority of children with unintentional ingestion were under 5years of age [2, 15] studies have shown that age < 5 are adventurous and need to explore the world around them and use to participate in reckless actions if unsupervised and expose to injurious substances [10]. Considering gender distribution we observed the same as was in most studies, males predominate female ratio of 1.3:1 in all age group, as mentioned in few studies range from 1.1-1.8:1 [2], however, children aged 10 and above we found an inverse ratio of 1:2 as female out numbers, the reason behind was not investigated, interestingly most of these girls was exposed during night time this may be accidental or unintentional but suspicious of intentional may not be completely excluded because of age, level of understanding regarding poison and fear of the family.
Timing of Ingestion and Number of Siblings
This was also observed that timing of ingestion plays an important role in exposure, and we found most children during afternoon hours interestingly around 50% of them were age five or less. It is difficult to point the reason, however, as mention in the previous study10, the long afternoon with a warm and humid climate of Karachi mothers and other caregivers use to take some rest (nap) and children use to be unattended and feel free to explore things and hazardous substances. This was not investigated in the past and need to be further evaluated. Unsupervised child during the afternoon hours lead to poison exposure either mother was out for a job or the caregiver was reckless. Petridou E, et al. [16] describe that the absence of one parent was associated with an increased risk of unintentional poisoning. The absence of mother during the daytime due to maternal employment and lack of family support was the two most deleterious risk factors recognized in his study [12, 17]. The literature identified that the number of siblings relates to the chance of poisoning exposure, we observed 40% of our children exposed to unintentional ingestion of hazardous things with >3 siblings, literature do support this [2].
Age of Mother and Education of Mother
Education in health also means prevention. To reduce pediatric poisoning, a prevention program may be practiced in clinics, ED or in-ward. Parents need counseling, however, maternal educational status and level of understanding count a lot in perceiving and practicing the knowledge [18]. Maternal education plays an important role in ingestion prevention as described by Bilal, A. et al. who identified a PAR (population attributable risk) score of 15% if maternal education level was of 10 years while it rose to 38% among mother with no formal education [2, 12, 14]. A multi-variant study demonstrates children of young mothers [19] with tenth-grade education were prone to poisonous exposure. Somehow similar findings we observed in our study.
Large family size seems to be protective with more available observing eyes on child, literature support with evidence, however in this study, we found a reveres pattern and more children belong to the joint family system with 5 or more adult members, however, if there is lack of family support the risk remain high, one reason may be that our catchment area is of low socioeconomic category [20] adult members may be on employment while children remain at home, this need to be evaluated further and it was missed in our study. Similarly, number of children within a family is directly related to the risk of ingestion which doesn’t favor our study [12].
Types of Poison Ingestion
Kerosene oil, as a single agent, is almost the most common hydrocarbon ingested in liquid form, different categories of medicines remain on top of the list [2, 10, 21, 22]. Kerosene oil is readily available in most houses and are still in use in stoves for cooking purposes among low-income families, we use it for few other purposes, hence present in most houses. Accidental ingestion of hydrocarbons (especially kerosene) is common among children under five, especially, if they are kept in some familiar container like cups, cans, mineral water bottles or attractive beverages bottles. Regarding another common ingestion of poison i.e. medicines; children use to take readily available medicines that look like candies and their curious nature of habit to follow what adults do. In this study we didn’t focus on which medicine children are exposed to most, this entirely depends on the availability of drugs. Some of the rare ingestions like plants products, pesticides, and detergents etc were not discussed in this study.
Outcome
We observed mortality of 4%, this seems to be a huge number however similar findings was observed by Manzar N, et al [2]. This is may be partially dependent on age, amount and time of ingestion, delay in seeking medical treatment, and how and what treatment were executed and socioeconomic status of the family. Mortality of 11.6% was observed from India, whereas 2.5% to 13.6% was observed [2, 15, 22] Inadequate supervision either by mother or other caregivers is one of the key factor associated with unintentional ingestion.
Limitation and Strength
This was a hospital based study which is the main limitation of our study. We need to conduct a community based or multicenter study with a more elaborated methodology to highlight the actual magnitude of the disease and to identify underlying risk factors. Though the study hospital is a referral center, this didn’t have a toxicology department, poison center or a toxicologist. The questionnaire was designed based on the variable available in the literature and was tested by study participants and institutional review board, expert review and epidemiologist input was not opted. Data collection was not a must from all cases, only those who gave consent were enrolled, hence a good number either didn’t gave consent or had a doubtful history of ingestion and were excluded. Under-reporting of cases who do not seek treatment at health care facility may be one factor of limited cases.
Conclusion
There are few generic factors as evident from the literature that may lead to increased risk of unintentional exposure to poison among our children this includes low parental education and socioeconomic status, larger family size or children in the family, unsafe storage of medicines and household chemicals, history of the previous poisoning.
Kerosene ingestion and easily available drugs remain the most common ingestions; younger age and male predominate from most literature.
Ethics Approval
This study was exempted for informed consent by ethical review committee of National Institute of Child Health Karachi.
Consent for Publication
Not applicable.
Availability of Data and Materials
Most of the data generated or analyzed during this study are included in this article. Limited data can be provided in person on request to the main author.
Competing Interests
The authors declare that they have no competing interests.
Funding
This study was not funded by any institution or organization.
Authors’ Contributions
AJ was the main author who collected data from children’s parents/guardian regarding poisoning with its socio-demographic factors and analyzed and interpreted that data. SF helped in collecting and analyzing data. ES was a major contributor in writing the manuscript along with some help in data analysis. All authors read and approved the final manuscript.
Acknowledgements
Not applicable.
References
-
(2020) Environmental health in emergencies. Poisoning.
-
Manzar N, Ali Saad SM, Manzar B, Fatima SS (2010) The study of etiological and demographic characteristics of acute household accidental poisoning in children-a consecutive case series study from Pakistan. BMC Pediatrics 10(28): 2-6.
-
Steele P, Spyker DA (1985) Poisonings**.** Paediatrics clinics of North America 32(1): 77-86.
-
London L, Baillie R (2001) Challenges for improving surveillance for pesticide poisoning: policy implications for developing countries. Int J Epidemiol 30(3): 64-70.
-
(2019) Poison prevention and management. International program on chemical safety: WHO.
-
Satish KV, Shivakumar P, Mandar RS (2015) Socio- demographic profile of paediatric poisoning cases in Bangalore, India. Indian J Community Med 2(4): 225- 228.
-
Ahuja H, Mathai AS, Pannu A, Arora R (2015) Acute poisonings admitted to a tertiary level intensive care unit in northern India: patient profile and outcomes. J Clin Diagn Res 9(10): UC01-4.
-
Peden MM, Oyebite K, Ozanne-Smith J (2008) World report on child injury prevention. World Health Organization.
-
Fatmi Z, Kazi A, Hadden WC, Bhutta ZA, Razzak JA, et al. (2009) Incidence and pattern of unintentional injuries and resulting disability among children under 5 years of age: results of the National Health Survey of Pakistan. Paediatric and Perinatal Epidemiology 23(3): 229-238.
-
Siddiqui EU, Razzak JA, Naz F, Khan SJ (2008) Factors associated with hydrocarbon ingestion in children. J Pak Med Assoc 58(11): 608-612.
-
Ahmed B, Fatmi Z, Siddiqui AR, Sheikh AL (2011) Predictors of unintentional poisoning among children under 5 years of age in Karachi: a matched case control study. InJ Prev 17(1): 27-32.
-
Chandimal MBK, Jayamanne SF, Chamilka Y, Jayasinghe CK (2017) Risk Factors for Acute Unintentional Poisoning among Children Aged 1-5 Years in the Rural Community of Sri Lanka. International Journal of Pediatrics.
-
Singh S, Singhi S, Sood NK, Kumar L, Walia BN (1995) Changing pattern of childhood poisoning (1970-1989): experience of a large north Indian hospital. Indian pediatr 32(3): 331-336.
-
Ahmed B, Fatmi Z, Siddiqui AR (2011) Population attributable risk of unintentional childhood poisoning in Karachi Pakistan. PLoS ONE 6(10).
-
Hamid MH, Butt T, Baloch GR, Maqbool S (2005) Acute poisoning in children. J Coll Physicians Surg Pak 15: 805- 808.
-
Petridou E, Kouri N, Polychronopoulou A, Siafas K, Stoikidou M, et al. (1996) Risk factors for childhood poisoning: a case-control study in Greece. Injury Prevention 2(3): 208-211.
-
Mansori K, Soori H, Farnaghi F, Khodakarim S, Mansouri S, et al. (2016) A case-control study on risk factors for unintentional childhood poisoning in Tehran. Journal of the Islamic Republic of Iran, pp: 330-355.
-
Hassan OU, Qadri H, Mir U, Ahmed B (2013) Unintentional childhood poisoning, epidemiology and strategies for the prevention and policy change in Pakistan. J Ayub med coll Abbottabad 25(3-4): 90-93.
-
Beautrais AL, Fergusson DM, Shannon FT (2008) Accidental poisoning in the first three years of life**.** Journal of Paediatrics and Child Health 17(2): 104-109.
-
Baqir H, Baig MA, Brown N, Mian AI (2017) Accidental poisoning in young children: an emergency medicine perspective for Pakistan and other low-and middle- income countries and a call for action. Eurasian J Emerg Med 16(4): 140-143.
-
Ahmad B, Shirazi IH, Naeemullah S, Tahir M, Shabbir A, et al. (2014) Accidental Childhood Poisoning. Journal of Rawalpindi Medical College (JRMC) 18(2): 216-218.
-
Aqeel M, Munir A, Khan A (2009) Pattern and frequency of acute poisoning in children. Pak J Med Sci 25(3): 479- 483.
- Pattern of Gonadal Hormones in Oral Testosterone-Supplimented Male Wistar Rats with Diabetes-Induced Hypogonadism
- Re-Evaluation of the Genotoxicity of Currently Used Food Dyes in Mouse Multiple Organs Via Continuous Administration by Drinking Using the Comet Assay
- Pharmacogenetics of Type 2 Diabetes Mellitus: Linking Genetic Variability to Drug Efficacy and its Cardiovascular Outcomes
- Exploratory Proteomic Profiling of SARS-CoV-2 Infected THP-1 Macrophages Reveals Alterations in Inflammatory Response and Cellular Metabolism
- Study of Genotoxicity of Hepatocarcinogens in Multiple Organs in Mice by Feeding and Drinking Using the Comet Assay
- Spirulina Polypeptides Inhibit the Growth of Human Lung Tumor (H460) Cells