Advanced Cognitive Emotional Regulation Therapy (ACERT) for Addiction Treatment
The last decades have shown relevant improvement in the therapeutic strategies aimed at psychiatric symptoms; however, addiction treatment remains unclear and controversial. Although there are specific medications approved for treating alcohol and opioid abusers, the consumption of these and other drugs is still high along with their severe consequences.
Editorial
The last decades have shown relevant improvement in the therapeutic strategies aimed at psychiatric symptoms; however, addiction treatment remains unclear and controversial. Although there are specific medications approved for treating alcohol and opioid abusers, the consumption of these and other drugs is still high along with their severe consequences [1]. Pharmacological therapies for other substance use disorders are still in need, while their prevalence increases in many countries, as well as its burden of disease [2]. Currently, the ideal treatment for addiction involves a multidisciplinary team and combines pharmacological strategies, psychotherapy and contingency management aimed at reinforcing more adaptive behaviors. Considering pharmacological strategies for drug abuse, they are usually focused on symptoms such as craving - a subjective cognitive (desire thoughts) and emotional (arousal feelings) that is hard to validate. There is no consensus on how to define, measure and treat craving, since substance abusers are a heterogeneous population with different psychiatric comorbidities and personality disorders. Nevertheless, treatment of psychiatric symptoms (e.g.. anxiety and depression) with medications reduces drug use in clinical trials with samples composed of alcohol or drug addicts [3, 4, 5, 6].
Several hypotheses about the development of addiction have been studied in the last years. Among others, the Self-Medication Hypothesis gained considerable traction by the time of its initial publications. It was grounded on the assumption that drugs could relieve pre-existing psychological suffering and that there is some specificity in a person’s drug of choice [7]. Although this hypothesis derives mainly from clinical observation and subsequent studies raised questions about its validity, it turned into a relevant paradigm in the field of addictions [8].
Other theoretical models have documented a strong connection between emotional dysregulation, addictive behaviors and psychopathology among general and clinical samples. Emotional regulation strategies can be portrayed as automated or controlled methods used to cope with or modify the external expression and/or internal experiences. They are utilized when emotional states have unwanted impact on a desired outcome, and can be broadly described as aiming at adaptive or maladaptive strategies [9]. Research suggests that emotional dysregulation can act as a moderator between environmental factors - such as stressful events, and problematic substance use. However, longitudinal studies are needed to determine causality, as the use of drugs can also impact the ability to cope with negative affects [10]. Alexithymia has already been cited as a possible risk factor for substance use disorders [11], which shows the importance of evaluating cognitive aspects in addiction; since alexithymia may complicate subjective emotional states investigation using only questionnaires.
Most psychopharmacological studies in the addiction field focus their aims at specific systems, receptors or brain regions related to seeking behavior and self-control; they usually fall short in the real world due to the existence of stressful events and cue eliciting craving situations, which directly affect the regulation of emotional states, and are rarely reproducible in such studies. Currently, most clinical trials use objective outcomes – such as the amount of substance use and frequency of consumption in order to evaluate treatment improvement and medication efficacy.
Thus, although there are different classification systems in psychiatry - categorical and dimensional ones [12, 13], there is still a need for a logical framework that could help clinicians and pharmacotherapists project the evaluation and treatment of addicted patients using Emotional Regulation theories. In this sense, this Brief Communication aims to propose a model to organize, measure and treat addictions from the perspective of regulation of emotional and cognitive aspects of the mind with pharmacological and psychotherapeutic strategies.
Advanced Cognitive Emotional Regulation Therapy (ACERT)
The treatment framework proposed here originates from symptomatological dimensions commonly used in pharmacological and psychotherapeutic treatment in psychiatry [14]. The development of this model was based on the clinical experience of the authors in the addiction field along with a literature review, and took into consideration the main neurobiological systems that support the theoretical rationale for psychopharmacological therapeutic plans and algorithms used for psychiatric disorders.
First, it is relevant to mention that patients undergoing cognitive emotional interventions cannot be intoxicated in order to avoid confounding their withdrawal symptoms with psychiatric disorders. The main rationale of the model is that craving and addictive seeking behaviors are respectively internalized and externalized responses of the brain-mind complex in order to regulate cognitive and emotional signs. They are usually associated with stress, with the goal of reaching homeostasis or Wellness [15, 16]. As shown in Figure 1.
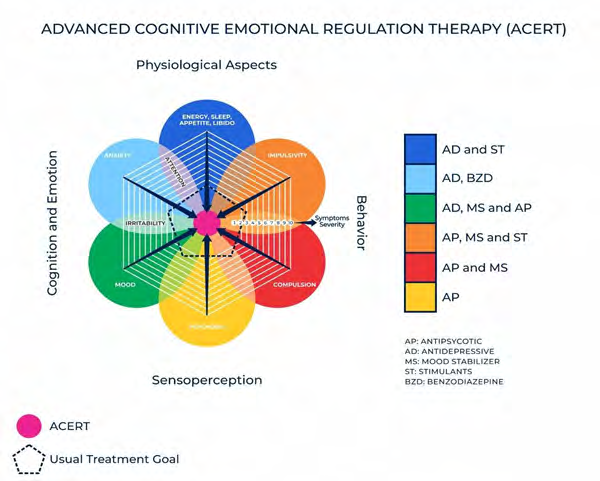
Our idea is that clinicians should assess symptomatology in the four poles in order to reduce craving and addictive symptoms, aiming at the “core” of the diagram (in pink). For each of these dimensions and poles, there are specific psychopharmacological options, commonly divided in categories as antipsychotics, antidepressants, mood stabilizers, benzodiazepines and stimulants. Some medications may be in more than one category and many patients will need more than two or three to achieve a good cognitive emotional regulation. For example, depression can be treated with antidepressant and additional agents such as mood stabilizers and atypical antipsychotics. The model infers intersections between dimensions which represent symptoms presented in different disorders (eg. irritability) that could be treated with similar medications. In order to organize pharmacotherapy and psychotherapy options, each dimension or intersection (represented by different colors) may correspond to different classes of psychotropic drugs, such as antipsychotics, antidepressants, mood stabilizers and stimulants.
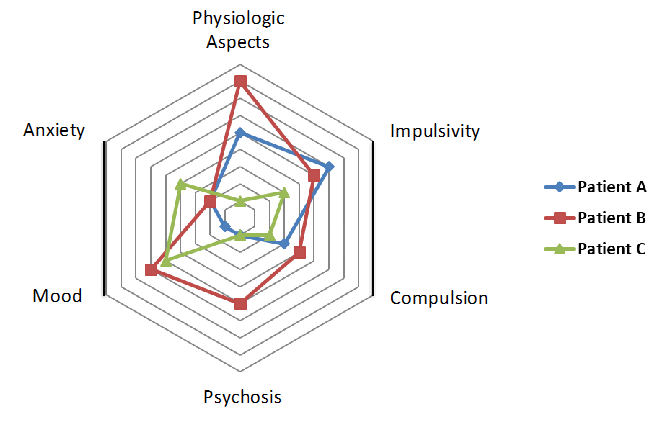
As shown in Figure 2, a spider graph portrays the varying degrees of symptoms in each group on a scale from 0 to 10; we present 3 case examples of different dimension dysregulation according to the patients’ psychiatric and personality characteristics. These would guide a more efficacious pharmacological and psychotherapeutic treatment plan. This new paradigm suggests that a more complex combination of medications could help achieve a higher cognitive emotional regulation impacting on drug- seeking behavior. We suggest that during treatment initiation symptom regulation should target more than 70% of improvement, which is the usual goal of psychiatric studies.
In future research, measurement instruments can be developed to investigate patients’ symptoms severity in each of the six dimensions. Therefore, interventions targeting reduction of specific symptomatology can be properly tested. We postulate that reducing symptoms related to anxiety, mood dysregulation, psychosis, impulsivity and physiologic dysregulation will consequently decrease craving, which is associated with drug-seeking behavior and other symptoms of compulsive addiction disorders. Besides pharmacological interventions focused on signs and symptoms, this treatment model may include psychotherapy techniques such as Motivational Interviewing, Cognitive Behavioral Therapy (CBT), Relapse Prevention, Emotional Regulation Training and Mindfulness, for example. They are usually effective to regulate emotional and behavioral responses, with fewer side effects, especially in long-term treatments. Psychotherapies play an essential role in addiction treatment. The choice of a specific psychotherapy is in line with scientific evidence about addiction treatment, which supports CBT and neuropsychological interventions for improving decision- making deficits and altering response to drug-related cues [17]. However, recent literature also proposes a more integrative approach to addiction psychotherapy, adding new concepts to the theory of self-medication [18].
Besides emotional and cognitive regulation - which may reduce craving and drug-seeking behavior, most substance abusers and other types of addicted patients usually present past and current stressful events (socioeconomic, relationships, work) that should be also evaluated and addressed in order to decrease the source of dysregulation and maladaptive responses. One of the most useful instruments for this purpose is the Addiction Severity Index [19, 20]. Thus, this proposed model could be a complementary tool to help organize, evaluate and define the best pharmacological and psychotherapeutic practices aimed at addicted patients.
Conclusion
This Brief Communication emphasized the need for new paradigms in the field of addictions to cover the inherent complexities that occur in treatment modalities. We described a model with both biological and psychological aspects of substance use disorders and proposed an integrative intervention. Especially in this field, drug users can be extremely heterogeneous in terms of psychiatric comorbidities and socio demographic profile. Therefore, clinical trials with broad interventions combining multiple medications and different psychotherapeutic techniques can be quite expensive and difficult to develop, since it is hard to define which intervention led to an expected outcome or to an adverse effect. Moreover, clinical trials have been targeting medications related to the Reward System instead of interventions that could reduce psychological (cognition and emotion) suffering that could be designed regardless of the underlying specific mechanism of action since medications achieve different results and adverse effects in this population.
It is time to evolve in the direction of more complex studies with multiple assessments and tailored strategies and interventions centered in cognitive emotional regulation that seem to be useful and intelligible for most health professionals by helping improve behavioral control. Future research with adequate methodology must analyze and validate these propositions - which could be a game changer - and enhance strategies to evaluate and treat addiction. The authors also seek international collaboration in order to keep developing this innovative, transdiagnostic and user- friendly treatment model.
References
-
Peacock A, Leung J, Larney S, Colledge S, Hickman M, et al. (2018) Global statistics on alcohol, tobacco and illicit drug use: 2017 status report. Addiction 113(10): 1905- 1926.
-
Charlson FJ, Baxter AJ, Cheng HG, Shidhaye R, Whiteford HA (2016) The burden of mental, neurological, and substance use disorders in China and India: A systematic analysis of community representative epidemiological studies. Lancet 388(10042): 376-389.
-
Han DH, Kim SM, Choi JE, Min KJ, Renshaw PF (2013) Adjunctive aripiprazole therapy with escitalopram in patients with co-morbid major depressive disorder and alcohol dependence: Clinical and neuroimaging evidence. Journal of Psychopharmacology 27(3): 282- 291.
-
Martinotti G, Andreoli S, Di Nicola M, Di Giannantonio M, Sarchiapone M, et al. (2008) Quetiapine decreases alcohol consumption, craving, and psychiatric symptoms in dually diagnosed alcoholics. Hum Psychopharmacol 23(5): 417-424.
-
McGrath PJ (1996) Imipramine Treatment of Alcoholics with Primary Depression: A Placebo-Controlled Clinical Trial. Arch Gen Psychiatry 53(3): 232-240.
-
Salloum IM, Cornelius JR, Daley DC, Kirisci L, Himmelhoch JM, et al. (2005) Efficacy of Valproate Maintenance in Patients With Bipolar Disorder and Alcoholism. Arch Gen Psychiatry 62: 37-45.
-
Khantzian J (1985) Focus on Heroin and Cocaine Dependence. Am J Psychiatry 6.
-
Khantzian EJ (1997) The Self-Medication Hypothesis of Substance Use Disorders: A Reconsideration and Recent Applications. Harv Rev _Psychiatry_ 4(5): 231-244.
-
Leppanen J, Brown D, McLinden H, Tchanturia K, Williams S (2021) The role of emotion regulation in eating disorders: A network meta-analysis approach. Front Psychiatry 13: 793094.
-
Cavalli JM, Cservenka A (2021) Emotion Dysregulation Moderates the Association Between Stress and Problematic Cannabis Use. Front Psychiatry 11: 597789.
-
Orsolini L (2020) Unable to Describe My Feelings and Emotions without an Addiction: The Interdependency between Alexithymia and Addictions. Front Psychiatry 11: 543346.
-
Goldberg LR (1993) The Structure of Phenotypic Personality Traits. American Psychologist, pp: 9.
-
Watson D, Levin‑Aspenson HF, Waszczuk MA, Conway CC, Dalgleish T, et al. (2022) Validity and utility of Hierarchical Taxonomy of Psychopathology (HiTOP): III. Emotional dysfunction superspectrum. World Psychiatry 21(1): 26-54.
-
Kessler FHP, Marchi N, Ornell F, Scherer JN, Sordi AO, et al. (2019) Advanced Cognitive Emotional Regulation Therapy (ACERT) for Addiction Treatment. 14th World Congress of Biological Psychiatry, Vancouver, Canada.
-
Alexander AC, Waring JJC, Olurotimi O, Kurien J, Noble B, et al. (2022) The relations between discrimination, stressful life events, and substance use among adults experiencing homelessness. Stress Health 38(1): 79-89.
-
Garke MA, Isacsson NH, Sörman K, Bjureberg J, Hellner C, et al. (2021) Emotion dysregulation across levels of substance use. Psychiatry Res 296: 113662.
-
Verdejo-García A, Alcázar-Córcoles MA, Albein-Urios N (2019) Neuropsychological Interventions for Decision- Making in Addiction: A Systematic Review. Neuropsychol Rev 29(1): 79-92.
-
Feingold D, Tzur Bitan D (2022) Addiction Psychotherapy: Going Beyond Self-Medication. Front Psychiatry 13: 820660.
-
McLellan TA, Cacciola JC, Alterman AI, Rikoon SH, Carise D (2006) The Addiction Severity Index at 25: Origins, Contributions and Transitions. Am J Addict 15(2): 113- 124.
-
Kessler F, Cacciola J, Alterman A, Faller S, Souza‑Formigoni ML, et al. (2012) Psychometric properties of the sixth version of the Addiction Severity Index (ASI-6) in Brazil. Braz J Psychiatry 34(1): 24-33.
- Pattern of Gonadal Hormones in Oral Testosterone-Supplimented Male Wistar Rats with Diabetes-Induced Hypogonadism
- Re-Evaluation of the Genotoxicity of Currently Used Food Dyes in Mouse Multiple Organs Via Continuous Administration by Drinking Using the Comet Assay
- Pharmacogenetics of Type 2 Diabetes Mellitus: Linking Genetic Variability to Drug Efficacy and its Cardiovascular Outcomes
- Exploratory Proteomic Profiling of SARS-CoV-2 Infected THP-1 Macrophages Reveals Alterations in Inflammatory Response and Cellular Metabolism
- Study of Genotoxicity of Hepatocarcinogens in Multiple Organs in Mice by Feeding and Drinking Using the Comet Assay
- Spirulina Polypeptides Inhibit the Growth of Human Lung Tumor (H460) Cells