Study of Rhinoconjunctivitis Quality of Life (RCQOL) in Children with Asthma and Allergic Rhinitis
Allergic Rhinitis (AR) is a non-infectious epidemic which can be prevented and controlled effectively with good quality of life in compliant children following the conventional inhalational therapies diligently. Paediatric Rhino-conjunctivitis Quality of Life Questionnaire (PRQLQ), devised by Professor Elizabeth Juniper is a validated questionnaire consisting of 23 parameters in 5domains. It is one of the best possible ways to judge the clinical severity and improvement in the affected children.
Introduction
Asthma and Allergic Rhinitis is considered as one airway one disease. Allergic manifestations in the form of Asthma and Allergic Rhinitis (AR) is a non-infectious epidemic which can be prevented and controlled effectively with good quality of life in compliant children following the conventional inhalational therapies diligently. The prevalence of Allergic Rhino-conjunctivitis has approximately doubled over the past 20years. Children with AR have been found to be at a greater risk of developing Asthma, Sinusitis, Behavioural & Sleep disturbances which can largely impact the child’s quality of life, cognitive function and school performance [1, 2]. PRQLQ was devised by Juniper EF, et al. to measure the quality of life in children with Allergic Rhinitis (AR) [3]. The PRQLQ (Paediatric Rhino-conjunctivitis Quality of Life) Questionnaire has 23questions in 5domains (Nose symptoms, Eye symptoms, Practical problems, Activity limitations and Other symptoms) [4]. The overall PRQLQ score is the mean of all 23responses and the individual scores is the mean of the items within those domains [5, 6, 7].
Aims & Objectives
- To study the clinical profile in childhood Asthma and Allergic Rhinitis.
- To evaluate the comorbidities of Asthma and Allergic Rhinitis.
- To study the association of rhino-conjunctivitis quality of life in childhood asthma and allergic rhinitis
Materials and Methods
This was a prospective study conducted over a 2-year period in a tertiary care hospital in Navi Mumbai. The study included 30patients between the age group of 6to12years having symptoms and signs of Allergic Rhinitis. Patient data was recorded in a pre-designed Proforma which included demographic details, history and examination findings. Rhino-conjunctivitis Quality of Life (RCQOL) scoring was done using PRQLQ Questionnaire as devised by Juniper EF, et al. for all the children with Allergic Rhinitis, satisfying the inclusion criteria. The study was approved by Institutional Ethics Committee (IEC) and an informed consent was obtained from parents/guardians of the participants. Children were asked to recall how they have been during the previous week and respond to each question on a 7-point scale. The overall PRQLQ score was calculated as a mean of all 23responses and the individual domain scores as a mean of the items within those domains. The quality of life affected in these children was then correlated with the severity of illness.
Inclusion Criteria
1. Children between 6-12yrs of age with asthma and allergic rhinitis satisfying the GINA (Global Initiative for Asthma) and ARIA (Allergic Rhinitis and its Impact on Asthma) guidelines. 2. Informed Consent given by the parents/guardians.
Exclusion Criteria
- <6years and >12years of age.
- Children with rhinitis of infective aetiology.
- Children unable to complete the RCQOL questionnaire.
- Parents and children who have not consented for the study.
Statistical Analysis
After data collection, entry was done in Microsoft Excel. Data analysis was done with the help of SPSS software v.23.0. All characteristics were summarized descriptively. For continuous variables, the summary statistics of mean ± standard deviation (SD) were used. For categorical data, the number and percentage were used in the data summaries and diagrammatic presentation. Chi-square (χ2) test was used for association between two categorical variables.
Results
In the present study, 30patients of Allergic Rhinitis (AR) between the age group of 6-12years were enrolled. 4 of 10(40%) children with family history of both allergic rhinitis and asthma, had moderate-severe persistent type of allergic rhinitis and 6 of 12(50%) without any family history had mild intermittent type of allergic rhinitis (Table 1).
| Family History | Classification of Allergic Rhinitis | |||||||
|---|---|---|---|---|---|---|---|---|
| Mild Intermittent | Mod-Severe Intermittent | Mild Persistent | Mod-Severe Persistent | |||||
| N | % | N | % | N | % | N | % | |
| Allergic Rhinitis | 0 | 0% | 1 | 33.3% | 0 | 0% | 2 | 66.67% |
| Asthma | 1 | 20% | 2 | 40% | 1 | 20% | 1 | 20% |
| AR + Asthma | 2 | 20% | 2 | 20% | 2 | 20% | 4 | 40% |
| Nil | 6 | 50% | 2 | 16.6% | 1 | 8.3% | 3 | 25% |
Table 1: Association Severity of Allergic Rhinitis and Family History.
Cough was the major presenting symptom in 29(96.7%) children, followed by rhinorrhoea 26(86.7%) and sneezing 21(70%) respectively. Wheeze, rapid breathing and headache were seen in 22(73.3%), 19(63.3%) and 14(46.7%) cases respectively day time sleep and snoring in 13(43.3%) each (Graph 1).
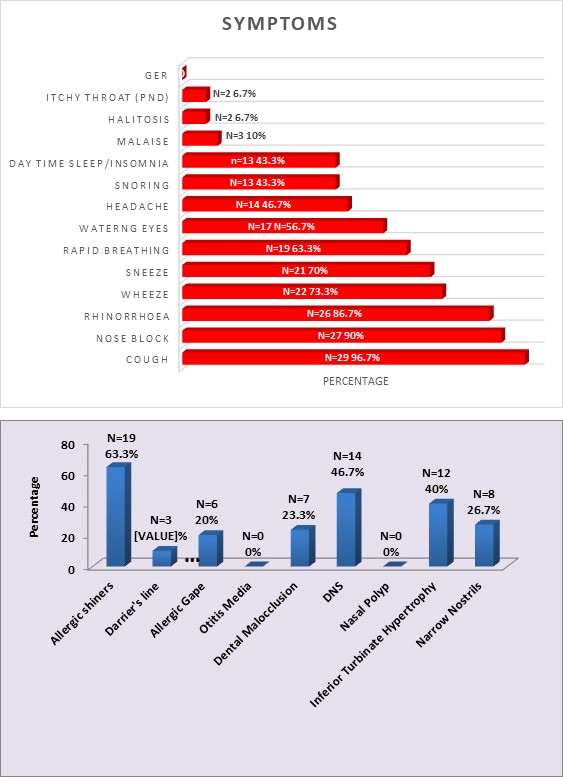
Graph 1: Distribution of Cases According to Symptoms.
In our study, allergic shiners was a common examination finding noticed in nearly 19(63%) children followed by DNS and inferior turbinate hypertrophy in 14(46.7%) and 12(40%) children respectively (Graph 2).
Graph 2: Distribution of Cases According to Examination Findings.
Highest number of children 27(90%) had asthma as a comorbidity. Post nasal drip was seen in 22(73.3%), Pharyngotonsillitis in 12(40%), Speech and behavioural abnormalities in 5(16.7%) children. Allergic conjunctivitis and dermatitis in 6(20%) each, Malnutrition featured in 10(33.3%) cases (Table 2).
| Comorbidities | N | % |
|---|---|---|
| Asthma | 27 | 90 |
| Post Nasal drip | 22 | 73.3 |
| Pharyngo-tonsillitis | 12 | 40 |
| Undernourished | 10 | 33.3 |
| Allergic Dermatitis (Eczema) | 6 | 20 |
| Allergic Conjunctivitis | 6 | 20 |
| Behavioural Abnormalities | 5 | 16.7 |
| Speech Abnormalities | 5 | 16.7 |
| Hypernasality | 1 | 3.3 |
| Otitis Media | 1 | 3.3 |
Table 2: Distribution of Cases According to Comorbidities.
Cases were distributed according to the 5domains of PRQLQ into Nose symptoms 30(100%), Eye symptoms 19(63.3%), other symptoms 24(80%), Practical problems
25(83.3%), and Activity limitations 21(70%) respectively (Graph 3).
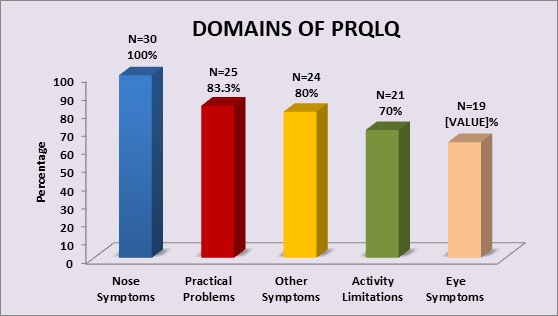
Graph 3: Distribution of Cases According to Domains of PRQLQ.
Mean range of nose symptoms was between 3.3-3.5, eye symptoms was 1.2-2.1, practical problems was 0.5-3.3, other symptoms was 0.9-2.3 and activity limitations was 1.2-1.5 (Table 3).
| Descriptive Statistics | Range | Mean | SD | ||
|---|---|---|---|---|---|
| Nose Symptoms | Stuffy/Blocked Nose | 0-6 | 3.5 | 1.9 | |
| Nose Symptoms | Sneezing | 0-6 | 2.8 | 2.1 | |
| Nose Symptoms | Runny Nose | 0-6 | 3.3 | 2 | |
| Nose Symptoms | Itchy Nose | 0-6 | 3.3 | 2.2 | |
| Eye Symptoms | Itchy Eyes | 0-6 | 2.2 | 2.4 | |
| Eye Symptoms | Watery Eyes | 0-6 | 2.1 | 2.3 | |
| Eye Symptoms | Swollen/Puffy Eyes | 0-6 | 1.4 | 2.2 | |
| Eye Symptoms | Sore Eyes | 0-6 | 1.2 | 2.2 | |
| Practical Problems | Rub your Eye/Nose | 0-6 | 2.4 | 2.2 | |
| Practical Problems | Blow your nose | 0-6 | 3.3 | 2 | |
| Practical Problems | Carry Kleenex | 0-6 | 2.6 | 1.9 | |
| Practical Problems | Take Medication | 0-6 | 1.9 | 1.4 | |
| Practical Problems | Embarrassed | 0-6 | 0.5 | 1 | |
| Practical Problems | Other Symptoms | Thirst | 0-6 | 1.4 | 1.3 |
| Scratchy and Itchy Throat | Other Symptoms | 0-6 | 0.9 | 1.3 | |
| Headache | Other Symptoms | 0-6 | 1.3 | 1.8 | |
| Tired | Other Symptoms | 0-6 | 2.3 | 1.4 | |
| Not well all over | Other Symptoms | 0-6 | 2.3 | 1.4 | |
| Irritable | Other Symptoms | 0-6 | 1.3 | 1.4 | |
| Activity Limitations | Playing Outdoors | 0-6 | 1.5 | 1.4 | |
| Activity Limitations | Hard to get to sleep | 0-6 | 1.5 | 1.7 | |
| Activity Limitations | Wake up during the night | 0-6 | 1.5 | 1.7 | |
| Activity Limitations | Hard to pay attention | 0-6 | 1.2 | 1.5 |
Table 3: Descriptive Statistics of Domains of PRQLQ.
The descriptive statistics of domains of PRQLQ has been shown in Graph 4.
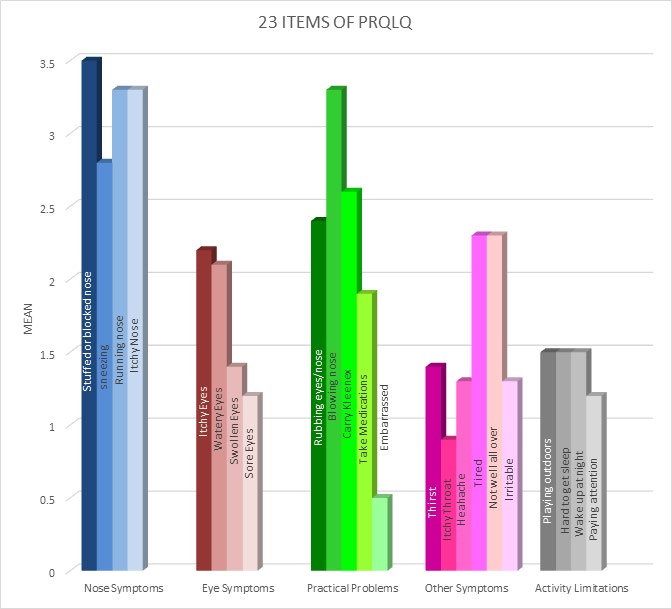
Graph 4: Descriptive Statistics of Domains of PRQLQ.
Children were classified according to severity of PRQLQ; 20(66.7%) cases were in the mild category, 6(20%) and 4(13.3%) were in the moderate and severe category respectively (Graph 5).
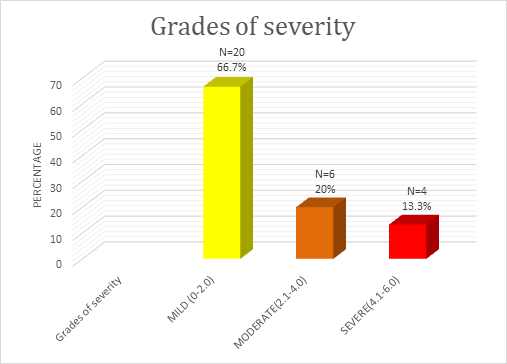
Graph 5: Distribution of Cases According to Grades of Severity of PRQLQ Score.
Association of PRQLQ domains and grades of severity showed nose symptoms being affected in all 30 (100%) patients and majority of them had mild degree of affection i.e, 20 (66.7%).
Discussion
The family history was directly proportional to the grade of AR and Asthma severity. The entity of cough variant rhinitis has been proposed as it primarily results from post nasal drip. Cough featured in (90%) of the subjects in our study followed by sneezing, rhinorrhoea and nose block. A similar study has highlighted cough as an important symptom in children with AR and Asthma [4]. In a cross-sectional study rhinorrhoea was the most common manifestation followed by itchy nose, nasal congestion and watery eyes [8, 9]. Nasal congestion was however seen as the most common symptom in another study [10]. Chronic cough should be detected as a symptom of AR and Asthma and treated appropriately for steroid- sparing effect. Nevertheless, another contradictory study reported nasal congestion to be the most common symptom of the disease [10]. Our study revealed allergic shiners as the most common finding followed by DNS and ITH. Day time somnolescence increased school absenteeism and led to diminished school performance. Similar observations were noted in other studies [11].
Asthma was the most common comorbidity observed in our study. A similar observation was reported which revealed that AR and Asthma control were directly proportional to each other [12]. Another interesting study showed AR findings in 58% of asthmatic children; however no association was established with asthma severity [13]. The other noteworthy co-morbidities were Post nasal drip, Pharyngotonsillitis, Speech and behavioural abnormalities, allergic conjunctivitis and dermatitis. The domains of PRQLQ highlighted majorly the nose symtptoms in children.
Similar findings were noted in two Indian studies and a study conducted in western Iran [8, 11, 12]. The positive aspects of the domains of PRQLQ across age groups revealed mild affection.
Conclusion
Rhino-conjunctivitis quality of life would be an adjuvant and enhance management of patients with AR and Asthma. It should be incorporated in the history taking and therapeutic management as a clinical assessment tool. The questionnaire by Juniper EF, et al. would serve as a validated method for assessing PRQLQ in the paediatric age group.
References
-
Juniper EF (1998) Impact of upper respiratory allergic diseases on quality of life. J Allergy Clin Immunol 101(2): 386-391.
-
Juniper EF, Guyatt GH, Griffith LE (1994) Determining a minimal important change in a disease-specific Quality of Life Questionnaire. J Clin Epidemiol 47(1): 81-87.
-
Juniper EF (1997) Quality of life in adults and children with asthma and rhinitis. Allergy 52(10): 971-977.
-
Lahiri KR, Tullu MS, Kalra R (2010) Clinical Profile, Co-Morbidities and Health Related Quality of Life in Pediatric Patients with Allergic Rhinitis and Asthma. Al Ameen J Med Sci 3(4): 300-311. 5. Durham SR, Nelson H (2011) Allergen immunotherapy: a centenary celebration. World Allergy Organ J 4(6): 104-106. 6. Scadding GK (2015) Optimal management of allergic rhinitis. Arch Dis Child 100(6): 576-582.
-
BrozekJ L, Bousquet J, Agache I, Agarwal A, Bachert C, et al. (2017) Allergic Rhinitis and its Impact on Asthma (ARIA) guidelines-2016 revision. J Allergy Clin Immunol 140(4): 950-958.
-
Kalmarzi R, Khazaei Z, Shahsavar J, Gharibi F, Tavakol M, et al. (2017) The impact of allergic rhinitis on quality of life: a study in western Iran. Biomedical Research and Therapy 4(9): 1629-1637.
-
Mohammadi K, Gharagozlou M, Movahedi M (2008) A single center study of clinical and paraclinical aspects in Iranian patients with allergic rhinitis. Iran J Allergy Asthma Immunol 7(3): 163-167.
-
Shariat M, Pourpak Z, Khalesi M, Kazemnejad A, Sharifi L, et al. (2012) Quality of life in the Iranian adults with allergic rhinitis. Iran J Allergy Asthma Immunol 11(4): 324-328.
-
Bhattar A, Kolhe S, Rai R, Jafri N (2019) Allergic Rhinitis with Commorbidities and Rhinoconjunctivitis Quality of Life(RCQOL) In Children. Global J Research Analysis 8(4): 1-3.
-
Nanda MS, Devi R (2019) Seasonal variation of allergy profile of patients visiting a tertiary care hospital in hilly areas of Himachal Pradesh. Int J Community Med Public Health 6(1): 146-150.
-
Oladeji S, Nwawolo C, Adewole (2013) Allergic rhinitis among adult bronchial asthmatic patients in Lagos, Nigeria. J West Afr Coll Surg 3(2): 1-14.
- Are the Vaccines the Only Solution to Prevent the COVID-19 Pandemic? Part Two
- Clinical Characteristics of Women in this New Global Immunodeficiency
- Cell Dynamics in HIV Pathogenesis: Insights and Implications
- Determination of the CDR (CDR1, CDR2) « Complementary- Determining Region Invertebrate Primitive Antibody from Sea Star »
- Prioritizing Care for High-Risk COVID-19 Patients in the EU: 10 Civic Recommendations to the Institutions
- Comprehensive Insights into ModRNA Vaccines: Persistent PP-Spike Recombinant Protein, Hyperimmune/Inflammatory Reactions, Thrombotic Vasculopathy, Chronic Organ Complications and Excess Deaths