Genetic Variation in TNF-α, its Relation with Inflammatory Biomarkers and Susceptibility to Rheumatoid Arthritis
Background: Tumor necrosis Factor-α (TNF-α) is encoded and controlled by TNF-α gene, which is involved in rheumatoid arthritis (RA) susceptibility. This research aimed to identify genetic variations of TNF-α (G308A) and to establish its association with inflammatory markers in Rheumatoid Arthritis predisposition. Methods: In the present study, fifty RA patients and fifty volunteers were involved and evaluated for the C-reactive protein, rheumatoid factor, and TNF-α were estimated by ELISA, Erythrocyte Sedimentation Rate (ESR) by Wintergreen method and for TNF-α-308 G>A polymorphism by polymerase chain reaction with amplification refractory mutation system (PCR-ARMS). Results: The CRP, RF, ESR and TNF-α were significantly elevated in RA patients relative to controls. The serum level TNF-α was also significantly elevated in female patients and in patients ≥50 years. Analysis of TNF-308 gene polymorphism revealed that GG genotypes were more prevalent in RA patients than in the healthy individuals and that GG genotype may be a potential factor to RA. The G allele was more common in RA than in the control. Elevated TNF-α serum levels were significantly associated the GG genotype and functional disability in RA patients. Conclusion: TNF-α promoter 308polymorphism GG genotype may be considered as a risk factor for RA and the TNF-α serum level was significantly related to the functional disability in the disease.
Introduction
Rheumatoid arthritis (RA) is considered as one of autoimmune diseases that cause joint damage throughout the body and it is a state of prolonged inflammation that results in joint deformity and function loss within 10years after initiation [1]. Immune cells hyperactivity causes destruction of the synovial sheath, and joint damage results in severe arthritis with a progressive deterioration of the joint cartilage [2]. It affects the quality of life and has a major negative impact on the ability to perform day-to-day activities [3]. Epidemiological data suggest the involvement of multiple genetic factors and environmental triggers. Overall, the heritability of RA is thought to be around 65% [4], the disease is known to be a complex disorder that leads to its development and appearance. Genetic predisposition, gender and oldness, contagious causes, biochemical, nutritional, socioeconomic, and ethnic aspects are risk factors for the disease. Most of these variables are likely related with both the onset and strength of the disease [5].
Alteration in cytokine production plays a major role in the disturbance of the immune system and causes RA which is the commonest autoimmune disease [6]. The immune cells secrete cytokines that involved in the contact between cells during cell injury, infection, and inflammation, and it is a vital component of immune system communication [7]. The most of these cytokines are pro-inflammatory as interleukins (IL1,6,15,16,17,18), tumor necrosis factor and interferon gamma that cause local and systemic effects of the disease [8]. Tumor necrosis factor is a powerful cytokine that triggers the release of other cytokines, TNF-α- and IL-1 release causes damaging effects on the joints [9]. Aberrations of TNF-α had been observed in rheumatoid arthritis [10].
TNF-α plays an important role in facilitate various immune responses including inflammation [11], necrotic lesions and cell suicide regulation [12], and cytotoxic activity stimulation [13]. TNF-α is capable of inducing its function through binding to membrane receptors [14]. Type I receptors (TNFRI) are more general and developed on all types of cells compared to Type II (TNFRII) that found specifically on immunological cells [15].
TNF-α is coded and controlled by TNF-α gene that positioned inside the major histocompatibility region of Class III in 6chromosome [16]. Individual alterations in TNF development in healthy controls were observed with phenotypes of high and low producers suggesting a major genetic involvement in TNF-α synthesis regulation [17], these findings recommend that polymorphism in the TNF-α regulatory region might influence its production. G to A transformation at position 308 (rs 1800629) was most frequently studied among the common polymorphisms in the promoter [18].
TNF-α overproduction contributes to various diseases such as inflammatory intestinal disease and rheumatoid arthritis [19], TNF-α inhibitors play a considerable role in treatment of chronic rheumatoid arthritis [20], for TNF-α, genetic variation on-308 results in two allic variants in which guanine (G) describes the more prevalent variant and adenine (A) describes the low prevalent one [21]. This study was conducted to detect TNF-α genetic variant and assess its relationship with certain inflammatory markers for the risk of development of rheumatoid arthritis.
Methods
This research is a case control study done in the College of Applied Medical Sciences, Taif University’s female section. The study comprised fifty patients with rheumatoid arthritis disease who joined the Rheumatology Clinic, King Faisal Special Hospital, Taif, KSA. Fifty healthy people of similar age and sex with the RA patients and with no clinical and laboratory signs of RA or other diseases were used as a control group.
The research was accepted by the ethical committee of the College of Applied Medical Sciences and all contributors attained informed consent after knowing the research goal. According to the American College of Rheumatology, inclusion criteria are all patients with rheumatoid arthritis selected and have positive rheumatoid factor [22]. Exclusion criteria are patients with other rheumatologic diseases like: Systemic lupus erythematous, mixed disease of the connective tissue, dermatomyositis, and scleroderma. According to the Kellgren score [23], the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) and the Lequesne index [24, 25], functional disability in RA has been measured in all patients.
Preparation of Blood Samples
A 10ml of peripheral venous blood sample has been collected from all included participants; 5ml of each sample obtained were collected in EDTA tubes for DNA extraction and ESR estimation.
The residual sample was left for one hour to coagulate at room temperature in a serum separator collection tube, and centrifuged for 5minutes at 3000rpm. The serum was collected and stored at -20°C until to be used. In serum samples of patients and controls, CRP and RF values were measured using Human C Reactive Protein ELISA Kit (CRP), abcam, Cambridge, MA, USA (Cat No: ab99995), and rheumatoid factor (RF), ELISA Kit, My Bio Source, Inc. San Diego (Cat No. MBS262327), CA 921953308, USA, respectively and by using Westergren approach ESR was calculated. Serum TNF-α level was estimated by using Abcam Human TNF alpha ELISA Kit, Cambridge, MA, USA (ab181421) according to the manufacturer’s protocol.
Genomic DNA Extraction
DNA from the peripheral blood obtained in tubes containing EDTA from patients and controls was extracted and purified using the QIAamp DNA mini kit (Qiagen CA, USA). The purified DNA was held at-80°C until using for genotyping.
TNF-α -308 G>A Promoter Polymorphism Detection by (PCR-ARMS)
Genotyping of TNF-α-308 G>A was performed using the polymerase chain reaction with amplification refractory mutation system (PCR-ARMS) as described by Balog A, et al. [26]. The PCR was performed with the recombinant Taq polymerase master mix (Dream taq green, code number k1081,LOT:00643300) (Thermo Fisher Scientific Ballics UAB, V A Cracino 8, LT002241 Vilnius, Lithuania) in a whole size of 25μl, TNF-α Primer sequences were as follows: TNF-α G forward primer: 5′-ATA GGT TTT GAG GGG CAT GG-3′; TNF-α A forward primer: 5′-AATA GGT TTT GAG GGG CAT GA-3′; and common reverse primer, 5′-TCT CGG TTT CTT CTC CAT CG-3′. Process conditions were performed for 1min at 9°C followed by 10cycles for 15s at 95°C and 50s at 65°C using thermal cycler with heated lid (Mastercycler® pro, Eppindorf, Germany), and 72°C for 40s and then 20cycles of 95°C for 20s, 56°C for 50s, and 72°C for 50s. The amplified PCR products were analyzed by 2% agarose gel and ethidium bromide staining followed by ultraviolet visualization. The PCR product for TNF-α-308 was detected at 184bp. The PCR assay had a positive regulation by amplifying the human growth hormone (HGH) gene.
Statistical Analysis
Data were collected, tabulated and analyzed using the computer program SPSS version 22.0. In this study, qualitative data existed by numbers and percentage and quantitative data were existing as mean and standard deviation. For comparing qualitative variables, chi-square (x²) test was used. A p-value of <0.05 was considered significant and Odd Ratio (OR) was used and 95% Confidence Interval (C.I.).
Results
The current research comprised of fifty RA patients and fifty volunteers. The patient’s age varied between 41 to 66years while in controls varied between 41 to 68years and includes 11male and 39female patients, 14 male and 36 female controls.
| No | Patients | Controls | |||
|---|---|---|---|---|---|
| % | No | % | |||
| Age | <50 | 14 | 28 | 16 | 32 |
| ≥50 | 36 | 72 | 34 | 68 | |
| Sex | Male | 11 | 22 | 14 | 28 |
| Female | 39 | 78 | 36 | 72 |
Table 1: Age and Sex of RA patients and controls.
C Reactive Protein
For RA patients, the C-reactive protein level (CRP) differed from 10.3 to 55.6mg/L with a mean ±S Dvalue of 30.02±11.48 and in controls differed from 1.01 to 8.12mg/L with a mean ± SD value of 4.32±2.1. There was a statistically difference in CRP values in patients and controls (t=15.58, P<0.0001), (Figure 1A).
Rheumatoid Factor (RF)
Analysis of serum level of RF in patients and controls. In RA patients the serum level of RF ranged between 15.21 and 55.37IU/ml with a mean ± SD value of 31.04±10.64IU/ ml. meanwhile in the controls it ranged between 0.19 and 4.02IU/ml with a mean ±SD value of 1.475±0.93, the variance in serum RF levels between patients and controls was statistically significant (t=19.58, P <0.0001), (Figure 1B).
Erythrocyte Sedimentation Rate (ESR)
In patients with RA the ESR ranged between 35 and 128mm/hr with a mean ±SD value of 72±28mm/hr. In control individuals ESR ranged between 1 and 13mm/h with 7.68±2.97mm/h as a mean ±SD value. There was statistically significant difference between patients and controls (t=16.06, P<0.0001), (Figure 1C).
Tumor Necrosis Factor (TNF-α) Levels in RA Patients and Controls
In RA patients the serum level TNF-α was ranged between 22.5 and 60.15pg/ml with a mean ±SD value of 38.19±12.34pg/ml. In the control group, it ranged between 0.001 and 4.65pg/ml with a mean ±SD value of 1.42±1.47pg/ ml. The difference between both groups was statistically significant (t=20.92, P <0.0001), (Figure 1D).

Figure 1: Levels of CRP (A), RF (B), ESR (C), and TNF- α(D) in RA patients and the controls. A. The difference of CRP levels in patients and controls was statistically significant (t=15.58, P<0.0001). B. The difference between in RF serum levels among RA patients and controls was statistically significant (t=19.58, P<0.0001). C. The difference between RA patients and the controls was statistically significant (t=16.06, P<0.0001) as regard ESR. D. The serum level TNF-α in RA patients was statistically significant (t=20.92, P <0.0001), compared to control group.
TNF-α serum level was found to be correlated with the patients’ age in RA. In patients less than 50years the serum level ranged between 22.5 and 28.4pg/ml with a mean and SD value of 24.9±1.7pg/ml. In patients with age more than 50years it ranged between 28.9 and 60.2 with a mean ±SD RA patients Controls OR X2 P (N= 50) (N= 50) (CI 95%) Genotypes No % No %
10 0.0058* GG 30 60 20 40 3.6 ( 1.1 – 11.8)
GA 15 30 18 36 2 ( 0.57 – 6.97) AA 5 10 12 24
value of 44.5±9.9 pg/ml. The difference between both age groups was statistically significant (t=7.837, P <0.0001), (Figure 2A). The serum levels of TNF-α were assessed in RA patients according to their sex. In males the serum level ranged between 25.3 and 30.9pg/ml with a mean and SD value of 28.1±1.9pg/ml. In females it ranged between 22.5 and 60.2pg/ml with a mean ±SD value of 41.03±12.6pg/ml. The difference between males and females was statistically significant (t=3.378, P=0.0015), (Figure 2B).
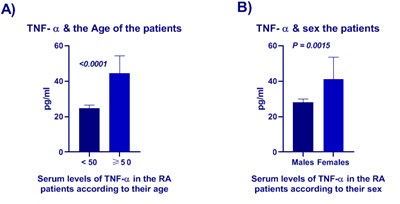
Figure 2: Serum level of TNF-α in patients with RA according to their age (A) and their sex (B). A. The serum level ranged from 22.5 to 28.4pg/ml with an average and SD value of 24.9±1.7pg/ml in RA patients below 50 years. RA patients over 50 had a mean ±SD value of 44.5±9.9 pg/ml, ranging from 28.9 to 60.2. B. The serum levels of TNF-α was statistically significant between males and females (t=3.378, P= 0.0015).
Genotyping of TNF-α 308 Promoter Polymorphism
We evaluated the incidence of TNF-308 genetic variant in the studied subjects; we found that GG genotypes were more prevalent in RA patients than in the controls and that GG genotype may be a possibility reason to RA and AA genotypes were high frequent in controls than in the RA. The difference in the frequency of TNF-α 308 polymorphism genotypes was statistically significant between RA patients and the controls (P=0.0058), (Table 2).
- *Statistically significant TNF-α 308 polymorphism genotypes between RA patients and the controls.
Table 2: Genotypes frequency of TNF-α 308 promoter polymorphism among the studied participants.
Analysis of allele’s frequency of TNF-α 308gene polymorphism revealed that the G allele was more frequent in RA (75%) and in controls (58%), A allele was more in the controls (42%). This difference was statistically significant P=0.0162, (Table 3).
| Groups Alleles | RA patients | Controls | OR (CI 95%) | P | ||
|---|---|---|---|---|---|---|
| (n=100) | (n=100) | |||||
| No | (%) | No | (%) | 2.172 | 0.0162* | |
| G | 75 | 75 | 58 | 58 | CI: 1.196 to 3.919 | |
| A | 25 | 25 | 42 | 42 |
Table 3: Alleles frequency of TNF-α 308 gene polymorphism among the studied participants.
*Statistically significant in alleles frequency of TNF-α 308 gene polymorphism between RA patients and the controls. Table 3: Alleles frequency of TNF-α 308 gene polymorphism among the studied participants.
TNF-α 308 Promoter Polymorphism and Serum Level of TNF-α
The serum level of TNF-α was observed to be elevated in patients with GG genotypes of RA in relation to the controls.
*The serum level of TNF-α in RA patients was statistically significant (t=21.56, P<0.0001), compared to control group. Figure 3: Serum levels of TNF-α in the patients and controls with GG genotype of TNF-α gene polymorphism.
The serum levels ranged between 29.02 and 60.15pg/ ml in RA patients with GG genotype with a mean ±SD value of 46.35±8.95pg/ml. on the other hand, it ranged between 0.24 and 4.7pg/ml with a mean ±SD values of 2.73±1.3pg/ ml in the controls with low GG genotype. The difference was statistically significant t=21.56, P<0.0001, (Figure 3).
Functional Disability Indices in RA
There is several indices to evaluate the functional activity of patients with RA, these includes Kellgren score, Lesquene index for activity, and Womac index. We assessed the relation of serum level of TNF-α, CRP, RF and the functional ability of RA patients using the above mentioned indices. The serum RF and CRP levels were not significantly correlated with different Kellgren scores, Lequesne grades, and Womac index scores. Meanwhile, the TNF-α serum levels was significantly associated with each grade of Kellgren score (P <0.0001), with Lequesne index (P<0.0001), and Womac index (P<0.0001), (Table 4).
| Patients | TNF-α Level | CRP Level | RF Level | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| No | % | Mean | SD | P | Mean | SD | P | Mean | SD | P | |
| Kelleqern score: | |||||||||||
| Grade 0 | 3 | 6 | 17.59 | 11.07 | <0.0001* | 16.02 | 4.042 | 0.184 | 18.24 | 5.273 | 0.6 |
| Grade I | 18 | 36 | 25.22 | 6.138 | 31.17 | 11.65 | 30.19 | 12.99 | |||
| Grade II | 22 | 44 | 42 | 10.83 | 30.39 | 11.88 | 29.27 | 13.04 | |||
| Grade III | 7 | 14 | 50.51 | 18.88 | 31.89 | 9.288 | 30.29 | 18.74 | |||
| Lesquene index for activity | |||||||||||
| Mild 1-4 | 16 | 32 | 23.45 | 6.015 | <0.0001* | 28.91 | 12.56 | 0.228 | 28.63 | 13.05 | 0.4 |
| Moderate 5-7 | 17 | 34 | 34.12 | 9.645 | 27.61 | 11.31 | 27.27 | 12.01 | |||
| severe 8-10 | 4 | 8 | 38.26 | 19.77 | 42.3 | 6.053 | 39.88 | 11.62 | |||
| Very severe 11-13 | 9 | 18 | 48.15 | 15.64 | 29.96 | 11.61 | 25.61 | 15.41 | |||
| Extremely severe ≥14 | 4 | 8 | 47.79 | 23.94 | 32.52 | 6.095 | 35.62 | 18.4 | |||
| Womac OA index | |||||||||||
| Less severe ≤ median (25) | 20 | 40 | 25.78 | 2.457 | <0.0001* | 29.74 | 11.93 | 0.891 | 29.5 | 12.26 | 0.9 |
| More severe > median (25) | 30 | 60 | 46.46 | 8.739 | 30.2 | 11.37 | 28.8 | 28.8 |
Table 4: Association of the serum levels of TNF-α, CRP, and RF levels and functional disability indices.
*Highly statistically significant association of the serum levels of TNF-α, CRP, and RF levels and functional disability indices in advanced stage of RA. Table 4: Association of the serum levels of TNF-α, CRP, and RF levels and functional disability indices.
Discussion
Rheumatoid arthritis (RA) is considered the highest prevalent inflammatory arthropathy that results in progressing articular injury, impairment of function and comorbidity [27]. Cytokine shows a significant role in the disease pathway, it triggers the inflammatory response, resulting in edematous joint damage and subsequently bone destruction through disease process. The TNFα gene has been identified as a critical element in conditions of inflammation and autoimmunity [28]. The functions played by TNF-α seem conflicting, and this was due to the genetic changes in the TNF-α locus that control the development and effect of the gene [29], and may be associated with increased TNF-α production [30]. This research aims to discover the genetic variants of TNF-α (G-308A) and to determine its relationship with RA.
In our research, we examined the CRP, and TNF-α level in addition to ESR in RA patients and the controls. We noted that the serum levels of CRP and TNF-α differ significantly between RA patients and controls, P<0.0001 and P<0.0001 respectively. Also there was a statistically difference in ESR between the two groups (P<0.0001). These results were in line with other studies of Feldmann M, et al. [27], Elahi MM, et al. [29], Shrivastava AK, et al. [31], Klimiuk PA, et al. [32], who reported that patients with RA have elevated levels of inflammatory markers, which indicate a potential role in the disease pathogenesis. Such biomarkers can also be used in the diagnosis and treatment of RA as indicators of syndrome development.
The TNF-α serum levels in RA patients assessed in relation to their age and sex. There was significantly increased TNF-α in patients with age above 50years (P<0.0001). Female patients were also noted to have a significantly higher TNF-α level than male patients (P=0.0015).
We assessed 308G >A polymorphism in the TNF-α promoter location in RA patients and controls. Our results revealed that in RA patients the genotype incidence of -308 G >A polymorphism was GG (60%), GA (30%), and AA (10%). While the incidence in control group was GG (40%), GA (36%), and AA (24%), the statistical study revealed a significant difference of this polymorphism between two groups (p=0.0058) in the genotype frequency of this polymorphism.
Our results of allele frequencies in RA patients indicate significant lower -308 A allele and higher -308 G allele frequencies relative to controls (P=0.016). These findings are similar to those recorded from different studies that based on different ethnicities [28, 33, 34, 35, 36]. As well as other reports have been published, this research holds the results that TNF -308 and allele has a protective impact on RA development. In contrast to our results, the studies of Danis VA, et al. [37], Vinasco J, et al. [38], Rodríguez-Carreón AA, et al. [39], Cuenca J, et al. [40] who confirmed that a allele in RA patients was statistically increased compared to control group.
In our study, we found a significant correlation between the serum level of TNF-α and GG genotypes in RA patients relative to the controls (P<0.0001). Our findings confirm the outcomes of Nemec P, et al. [41] who recorded high TNF-α in plasma and joint synovial fluidin RA patients with polymorphisms in the TNF-α promoter On the other hand, Pawlik A, et al. [42] reported no differences in TNF-α serum levels and genotype distribution and allelic frequencies of -308 G>A TNF-α polymorphism between RA patients and controls. The variability in TNFα expression between individuals indicates the presence of functionally distinct TNF alleles, including 308promoter polymorphism; that may play a role in RA susceptibility found that a significant increase in TNFα expression was observed in Egyptian patients with RA compared to healthy individuals but this increase in expression was not linked to a certain -238G/A and -376G/A single nucleotide polymorphism [43, 44].
The functional disability in RA patients was also evaluated using Kellgren scores, Lesquene grades, and Womac index scores and the serum levels of CRP, RF, and TNF-α. There was no statistically significant correlation between the serum levels of CRP, and RF and the degree of functional disability in RA patients. Meanwhile, the TNF-α serum levels were significantly correlated with the grade or the severity of functional disability in RA patients. Its
level was correlated with the grade of disability using the Kellgren score (P<<0.0001), level of disability by Lesquene index (P<0.0001), and severity of disability by Womac index (P<0.0001). This observation reveals that the serum level of TNF-α may be used as a measure of functional disability in RA patients.
The association between TNF 308G/A polymorphism and its production with responsiveness to anti TNF treatment still controversial revealed in RA patients with the TNF-α 308G allele reacts better to TNF-α adversary therapy [21], indicating that this allele plays an important role in the treatment by anti-TNF-alpha therapy in contrast results from Rielly, et al. who reported that the common TNF -308 (A) variant expects reduced responsiveness to treatment by TNF-α antagonists.
In conclusions, the present study showed that TNF-α promoter 308polymorphism GG genotype may be considered as a risk factor for Rheumatoid Arthritis and the TNF-α serum level was significantly related to the functional disability in the disease. The TNF-alpha -308A/G polymorphism may represent a significant risk factor for RA in Saudi population. We suggest that the study’s population be screened for TNF-α promoter 308 polymorphism to allow early diagnosis before complications arise to start early treatment with immunomodulator. A future study with a large number of patients is therefore needed to highlight these findings.
References
-
Li F, Xie X, Chen J, Gao J, Lu F (2015)Association of TNF-α gene polymorphisms with the risk of rheumatoid arthritis in Han Chinese population from Hunan. Zhong Nan Da XueXue Bao Yi Xue Ban 40(9): 945-954.
-
Sadaf T, John P, Bhatti A, Malik JM (2019) Lack of association of -863C/A (rs1800630) polymorphism of tumor necrosis factor-a gene with rheumatoid arthritis. Arch Med Sci 15(2): 531-536.
-
Singh JA, Saag KG, Bridges SL, Akl EA, Bannuru RR, et al. (2015) American College of Rheumatology guideline for the treatment of Rheumatoid Arthritis. Arthritis Rheumatol 68(1): 1-26.
-
Alamanos Y, Drosos AA (2005) Epidemiology of adult rheumatoid arthritis. Autoimmune Rev 4(3): 130-136.
-
Saad MN, Mabrouk MS, Eldeib AM, Shaker OG (2016) Identification of rheumatoid arthritis biomarkers based on single nucleotide polymorphisms and haplotype blocks: a systematic review and meta-analysis. J Adv Res 7(1): 1-16.
-
Ghorban K, Ezzeddini R, Eslami M, Yousefi B, Moghaddam BS, et al. (2019) PTPN22 1858C/T polymorphism is associated with alteration of cytokine profiles as a potential pathogenic mechanism in rheumatoid arthritis. Immunology letters 216: 106-113.
-
Kasama T, Isozaki T, Takahashi R, Miwa Y (2016) Clinical effects of tocilizumab on cytokines and immunological factors in patients with rheumatoid arthritis. Int immunopharmacol 35: 301-306.
-
Choy E (2012) Understanding the dynamics: pathways involved in the pathogenesis of rheumatoid arthritis. Rheumatology 51(5): 3-11.
-
Chen L, Huang Z, Liao Y, Yang B, Zhang J (2019) Association between tumor necrosis factor polymorphisms and rheumatoid arthritis as well as systemic lupus erythematosus: a meta-analysis. Brazilian J Med Biol Res 52(3): 7927.
-
Nalbant S, Birlik A (2017) Cytokines in rheumatoid arthritis.
-
Wallach D, Varfolomeev EE, Malinin NL, Goltsev YV, Kovalenko AV, et al. (1999) Tumor necrosis factor receptor and Fas signaling mechanisms. Annu Rev Immunol 17(1): 331-367.
-
Laster SM, Wood JG, Gooding LR (1988) Tumor necrosis factor can induce both apoptic and necrotic forms of cell lysis. J Immunol 141(8): 2629-2634.
-
Beyaert R, Fiers W (1994) Molecular mechanisms of tumor necrosis factor‐induced cytotoxicity: What we do understand and what we do not. FEBS Lett 340(1-2): 9-16.
-
Brockhaus M, Schoenfeld HJ, Schlaeger EJ, Hunziker W, Lesslauer W, et al. (1990) Identification of two types of tumor necrosis factor receptors on human cell lines by monoclonal antibodies. Proc Natl Acad Sci USA 87(8): 3127-3311.
-
Wajant H, Pfizenmaier K, Scheurich P (2003) Tumor necrosis factor signaling. Cell Death & Differentiation 10(1): 45-65.
-
Jahid M, Jha PK, Chawla D, Avasthi R, Ahmed RS (2017) Tumor necrosis factor-α-308 polymorphism in North Indian rheumatoid arthritis patients and association with mRNA and serum TNF-α. Clinical rheumatology 36(10): 2209-2216.
-
Louis E, Franchimont D, Piron A, Gevaert Y, Schaaf- Lafontaine N (1998) Tumour necrosis factor (TNF) gene polymorphism influences TNF‐α production in lipopolysaccharide (LPS)‐stimulated whole blood cell culture in healthy humans. Clin Exp Immunol 113(3): 401-106.
-
Groote DE (1998) Tumour necrosis factor (TNF) gene polymorphism influences TNF‐α production in lipopolysaccharide (LPS)‐stimulated whole blood cell culture in healthy humans. Clinical Exp Immunol 113(3): 401-406.
-
Sadaf T, John P, Bhatti A, Malik J (2018) Lack of association of –863C/A (rs1800630) polymorphism of tumor necrosis factor-a gene with rheumatoid arthritis. Arch Med Sci 15(2): 531-536.
-
Bitoun S, Miceli-Richard C, Verstuyft C, Juge PA, Dieudé P, et al. (2018) Frequency of tumour necrosis factor alpha receptor superfamily 1A multiple sclerosis-associated variants in patients with rheumatoid arthritis with anti- tumour necrosis factor therapy-related demyelinating complications. Ann Rheum Dis 77(12): 1835-1836.
-
Zeng Z, Duan Z, Zhang T, Wang S, Li G, et al. (2013) Association between tumor necrosis factor-α (TNF-α) promoter -308G/A and response to TNF-α blockers in rheumatoid arthritis: a meta-analysis. Modern rheumatology 23(3): 489-495.
-
Amett FC, Edworthy SM, Bloch DA, Mcshane DJ, Fries JF, et al. (1988) The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum 31(3): 315-324.
-
Kellgren JH, Lawrence JS (1957) Radiological assessment of osteo-arthrosis. Ann Rheum Dis 16(4): 494-502.
-
Roos EM. Klässbo M, Lohmander LS (1999) WOMAC Osteoarthritis Index: Reliability, validity, and responsiveness in patients with arthroscopically assessed osteoarthritis. Scand J Rheumatol 28(4): 210- 215.
-
Dawson J, Linsell L, Doll H, Zondervan K, Rose P, et al. (2005) Assessment of the Lequesne index of severity for osteoarthritis of the hip in an elderly population. Osteoarthritis and cartilage 13(10): 854-860.
-
Perrey C, Turner SJ, Pravica V, Howell WM, Hutchinson IV (1999) ARMS-PCR methodologies to determine IL-10, TNF-α, TNF-β and TGF-β1 gene polymorphisms. Transpl Immunol 2(7): 127-128.
-
Feldmann M, Maini RN (2001) Anti-TNFα therapy of rheumatoid arthritis: what have we learned?. Annu Re Immunol 19(1): 163-196.
-
Balog A, Gal J, Gyulai Z, Zsilák S, Mándi Y (2004) Tumour Necrosis Factor-a and Heat-Shock Protein 70-2 Gene Polymorphisms in a Family with Rheumatoid Arthritis. Acta Microbiol Immunol Hung 51(3): 263-269.
-
Elahi MM, Asotra K, Matata BM, Mastana SS (2009) Tumor necrosis factor alpha -308 gene locus promoter polymorphism: an analysis of association with health and disease. Biochim Biophys Acta 1792(3): 163-172.
-
Tsukamoto K, Ohta N, Shirai Y, Emi M (1998) A highly polymorphic CA repeat marker at the human tumor necrosis factor alpha (TNFAα) locus. J Human Genetics 43(4): 278-279.
-
Shrivastava AK, Singh HV, Raizada A, Singh SK, Pandey A, et al. (2015) Inflammatory markers in patients with rheumatoid arthritis. Allergol Immunopathol 43(1): 81- 87.
-
Klimiuk PA, Sierakowski ST, Latosiewicz RO, Cylwik BO, Skowronski J, et al. (2001) Serum cytokines in different histological variants of rheumatoid arthritis. J Rheumatol 28(6): 1211-1217.
-
Seki N, Kamizono S, Yamada A, Higuchi T, Matsumoto H, et al. (1999) Polymorphisms in the 5′‐flanking region of tumor necrosis factor‐α gene in patients with rheumatoid arthritis. Tissue Antigens 54(2): 194-197.
-
Cvetkovic JT, Jonsson WS, Stegmayr B, Dahlqvist RS, Lefvert AK (2002) Susceptibility for and clinical manifestations of rheumatoid arthritis are associated with polymorphisms of the TNF-alpha, IL-1beta, and IL- 1Ra genes. J Rheumatology 29(2): 212-219.
-
Ozen S, Alikasifoglu M, Bakkaloglu A, Duzova A, Jarosova K, et al. (2002) Tumour necrosis factor α G→ A− 238 and G→ A− 308 polymorphisms in juvenile idiopathic arthritis. Rheumatology 41(2): 223-227.
-
Yen JH, Chen CJ, Tsai WC, Lin CH, Ou TT, et al. (2001) Tumor necrosis factor promoter polymorphisms in patients with rheumatoid arthritis in Taiwan. J Rheumatology 28(8): 1788-1792.
-
Danis VA, Millington M, Hyland V, Lawford R, Huang Q, et al. (1994) Increased frequency of the uncommon allele of a tumour necrosis factor alpha gene polymorphism in rheumatoid arthritis and systemic lupus erythematosus. Disease markers 12(2): 127-133.
-
Vinasco J, Beraun Y, Nieto A, Fraile A, Mataran L, et al. (1997) Polymorphism at the TNF loci in rheumatoid arthritis. Tissue antigens 49(1): 74-78.
-
Rodriguez Carreon AA, Zuniga J, Hernandez-Pacheco G, Rodriguez Perez JM, Perez Hernandez N, et al. (2005) Tumor necrosis factor-alpha− 308 promoter polymorphism contributes independently to HLA alleles in the severity of rheumatoid arthritis in Mexicans. J Autoimmunity 24(1): 63-68.
-
Cuenca J, Cuchacovich M, Perez C, Ferreira L, Aguirre A, et al. (2003) The -308 polymorphism in the tumour necrosis factor (TNF) gene promoter region and ex vivo lipopolysaccharide‐induced TNF expression and cytotoxic activity in Chilean patients with rheumatoid arthritis. Rheumatology 42(2): 308-313.
-
Nemec P, Goldbergova PM, Stouracova M, Vasku A, Soucek M, et al. (2008) Polymorphism in the tumor necrosis factor-α gene promoter is associated with severity of rheumatoid arthritis in the Czech population. Clin Rheumatol 27(1): 59-65.
-
Pawlik A, Florczak M, Ostanek L, Brzosko M, Brzosko I, et al. (2005) TNF-alpha -308 promoter polymorphism in patients with rheumatoid arthritis. Scand J Rheumatology 34(1): 22-26.
-
Kaijzel EL, Bayley JP, Van Krugten MV, Smith L, De Linde VP, et al. (2001) Allele-specific quantification of tumor necrosis factor α (TNF) transcription and the role of promoter polymorphisms in rheumatoid arthritis patients and healthy individuals. Genes & Immunity 2(3): 135-144.
-
Mousa AK, Ghoneim AM, Noha B, Ahmed E (2014) TNF-α genetic polymorphisms and its expression in Egyptian rheumatoid arthritis patients. Am J Life Sci 2(4): 234- 240.
-
Rielly DO, Roslin NM, Beyene J, Pope A, Rahman P (2009) TNF-α −308 G/A polymorphism and responsiveness to TNF-α blockade therapy in moderate to severe rheumatoid arthritis: a systematic review and meta- analysis, The Pharmacogenomics Journal 9: 161-167.
- Are the Vaccines the Only Solution to Prevent the COVID-19 Pandemic? Part Two
- Clinical Characteristics of Women in this New Global Immunodeficiency
- Cell Dynamics in HIV Pathogenesis: Insights and Implications
- Determination of the CDR (CDR1, CDR2) « Complementary- Determining Region Invertebrate Primitive Antibody from Sea Star »
- Prioritizing Care for High-Risk COVID-19 Patients in the EU: 10 Civic Recommendations to the Institutions
- Comprehensive Insights into ModRNA Vaccines: Persistent PP-Spike Recombinant Protein, Hyperimmune/Inflammatory Reactions, Thrombotic Vasculopathy, Chronic Organ Complications and Excess Deaths