Epidemiological Characterization of the Infection by Treponema Pallidum in Pregnant Women in Beira City, Sofala, Mozambique
Introduction: Syphilis is one of several diseases that can be transmitted during pregnancy and childbirth, which can lead to complications during pregnancy and in the newborn. This is especially so when the pregnant woman is not diagnosed or treated properly and in a timely manner. Methodology: Data from 262 pregnant women prospectively included, aged 18-41years, attended at the Ponta Gêa Health Centre for antenatal clinics has been analyzed from January to September of 2016. In the prospective study, a rapid treponemal and a non-treponemal test were performed. A structured questionnaire was used to collect socio demographic and clinical variables, which was developed from the literature review. Results: The prevalence of active syphilis was 11.8%; the majority of reactive pregnant women were aged 18-25years (55.4%), (61.3%) of pregnant women were treated with doses below those recommended; only a small number of the partners were treated successfully. The highest seroprevalence of syphilis was found in housewives (77%), in those who attended primary education (71.6%) in those who had a monthly income of 1000- 3000 MZN (70.3%), in those with two or more pregnancies (55.7%) and living with someone has husband and wife (63.5%). The syphilis/HIV co-infection rate was high. Conclusion: According to the results obtained in this study, urgent measures are needed to assess the problems encountered and to improve the screening approach, treatment and monitoring of syphilis during pregnancy in order to prevent the cases of congenital syphilis.
Introduction
Effective preventive measures, such as condom use and relatively inexpensive treatment options aimed at disrupting the chain of transmission and preventing new cases, have not stopped Sexually Transmitted Infections (STIs) from continuing to be among the main causes of illness in the world [1, 2, 3]. Currently, these infections are still a major global public health problem, mainly in developing countries, affecting mainly women of child-bearing age and children [4, 5, 6]. STI- related complications are the leading cause of morbidity and mortality during pregnancy in these countries [7, 8], contributing to a high incidence of cervical carcinoma [9, 10]. The impact of these diseases on pregnant women and in their newborns is largely related to the non-compliance with the standards recommended for antenatal surveillance in order to prevent complications, such as vertical transmission [11]. Among STIs, syphilis stands out being one of the most worrying infection due to its consequences in adults and newborns of infected mothers. Infection in the newborn is entirely preventable if the mother’s infection is diagnosed and treated early during pregnancy with benzathine- penicillin.
More than one million people get a STI every day. Each year approximately 499million people acquire curable STIs, with etiology attributed to Treponema pallidum (syphilis), Neisseria gonorrhoeae (gonorrhea), Chlamydia trachomatis (chlamydiosis) and Trichomonas vaginalis (trichomoniasis) [12].
Two other WHO studies, conducted in 2005 and 2008, with the same methodological approach, i.e. to estimate new cases of curable STIs (chlamydia, gonorrhea, syphilis and trichomoniasis) in adults aged 15 to 49, showed that between these years there was an increase of approximately 11% of the number of cases, from 448.3 million in 2005 to 498.9million of new cases in 2008. The results of this study suggest that there was no improvement in the overall burden of curable STIs in this period [12, 13].
Among STIs that can be transmitted during gestation and delivery, syphilis has a high rate of vertical transmission and severe complications in the newborn. This infection is a systemic, sexually transmitted disease caused by a spirochete, Treponema pallidum, with a worldwide distribution, which in itself is a major public health problem [2, 14]. This infection is also a substantial cause of adult morbidity and may be, although rarely and mainly in individuals co-infected with Human Immunodeficiency Virus (HIV), a cause of death and increase the risk of transmission of this virus [8]. In recent years, there has been an increase in the prevalence of syphilis in both developing and industrialized countries, with an increase in the number of cases of primary and secondary syphilis in women of child-bearing age [3, 15, 16, 17, 18, 19].
Maternal syphilis continues to be a major cause of perinatal death in many developing countries, affecting a large number of pregnant women and resulting in substantial maternal and perinatal morbidity and mortality, which could be prevented through early diagnosis and proper treatment [13, 20, 21].
This whole situation is perfectly controllable, provided certain requirements are met. At present, the efficacy of syphilis treatment is well recognized, its diagnosis and its viable, cheap and cost-effective prevention in almost all situations [2, 13, 22], so it is regrettable that cases of syphilis continue to occur and congenital syphilis still exists.
Study Methodology
Description of the Study Area
This study was carried out at Ponta Gêa Health Centre. This health unit is among the six health units of the public sector with the highest number of users in the Beira city and is the Health Centre with better service delivery Pereira et al. In this unit, about 100 antenatal clinics are expected each month, so it has been used as a sentinel post for surveillance rounds for syphilis and HIV (MISAU, 2011).
Type and Study Population
This is a descriptive cross-sectional epidemiological study, the group studied was composed of pregnant women observed in antenatal clinics at the same Health Centre from April to June 2016. The invitation to these women to participate in the study was made by a nurse trained for data collection and informed consent was obtained during the usual lectures of antenatal clinics. After obtaining the informed consent, a blood sample was collected, according to the recommendations for the collection and processing of samples in use at this Health Centre. The analysis was performed at the Biochemistry Laboratory of the Ponta Gêa Health Centre. In parallel, clinical data were also collected from pregnant women with reactive syphilis tests for the data sheet.
Pregnant women included in the prospective group and with reactive samples using a rapid treponemal syphilis test (Rapid syphilis test 3.0 SD BIOLINE-TDR) were submitted to an RPR test. Women with reactivity for both tests were analyzed in terms of the characteristics of T. pallidum infection and then monitored, in order to verify if their therapy was adequate and was in accordance to the clinical phase of the infection (Figure 1).
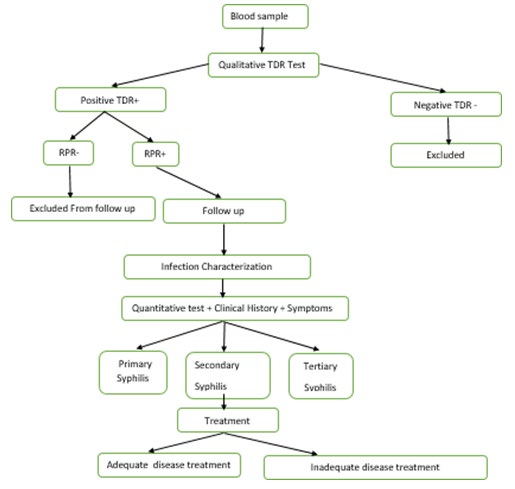
- The case definition was defined as any woman, whose results were reactive in the POCT and RPR tests (Table 1).
Table 1: Prevalence calculation formula in the prospective
T. pallidum Infection Screening
The whole blood from each of the pregnant women was collected into a heparin tube, transported to the laboratory and centrifuged at 2500 revolutions per minute (rpm) for five minutes. After centrifugation, the plasma was removed with a micropipette, the serum was then tested for the detection of antibodies against T. pallidum by a rapid treponemal test (Rapid syphilis test 3.0 SD BIOLINE). Diagnostic confirmation was performed with a non-treponemal test (RPR- Rapid Plasma Reagin Test).
Rapid Syphilis Test 3.0 SD Bioline
The 3.0 SD BIOLINE test is a continuous phase of an Immuno chromatographic test for the qualitative detection of antibodies of all T. pallidum isotype (IgG, IgM, IgA). The T. pallidum antigens used are 15kD and 17kDa recombinants. Serum, plasma or blood samples can be used for performing this group of tests. Processing this test does not require equipment, its storage being at a room temperature of (2- 30°C). In all samples included in the study, a qualitative evaluation was performed by POCT, according to the instructions of the Commercial shop of laboratorial tests. The plasma (10μl) was removed with the aid of a pipette into the testing well designed for this and then four drops of the diluent were added, waiting an interval of 20 minutes to obtain the result. If the control bar was not visible, the test was discarded and the sample was tested with a new test.
Non-Treponemal Test
The RPR test used in this study was the Macro-Vue-RPR Card Test. This technique is based on the flocculation method and uses as antigen a stabilized suspension of coal particles containing cardiolipin, cholesterol, lecithin, ethylene diamine tetra-acetic acid (EDTA) and choline chloride. EDTA stabilizes the antigen, dispensing with the need for daily preparation as it is necessary when using the VDRL test and choline chloride makes serum inactivation unnecessary. Coal particles make it possible to read the reaction macroscopically. The test was performed according to the protocol established by the Medicine shop in the qualitative evaluation. The result was obtained in less than 30minutes, which is why RPR can be considered a rapid test, although not a point of care.
Qualitative Evaluation
In all blood samples included in the study were performed a qualitative evaluation by the RPR technique. For such, a drop of (50μl) undiluted sample was put with the aid of a pipette into one of the circles of the carton provided by the Medicine shop, spreading it over the entire surface thereof. Thereafter, a drop of antigen suspension was added, stirred and the carton was placed on the automatic rotary shaker at 100rpm for 8minutes. In order to verify the correct execution of the technique and the state of the reagents, it was carried out simultaneously with the positive and negative controls. The reading was carried out under good light source. The test was considered reactive when flocculation was visualized (presence of black lumps) and non-reactive in its absence.
Data Management
The data were obtained during the antenatal clinics in the Ponta Gêa Health Centre wards and consisted of socio demographic data, symptoms, clinical signs and laboratory test results based on sheets suitable for the collection of retrospective and prospective data. Subsequently, the sheets were taken to the premises of Beira Operational Health Research Centre (CIOB) belonging to the National Institute of Health of Mozambique (INS), located in the same enclosure where the Ponta Gêa Health Centre is located, for typing and archiving them. The information gathered was inserted into a program file, and independent typists were selected and trained to work according to the double typing process for data input and comparison. The differences verified were corrected by the study investigators based on the data collection sheets that were filed at the CIOB’s premises. The electronic files were saved in a separate hard drive and in a USB drive. In the course of this process some sheets were excluded due to lack of some data.
Statistical Analysis
The data were analyzed by the SPSS programs, using a 95% confidence interval and a permissible error of 5%. The relative frequencies were calculated using this program. The data were analyzed jointly by the researchers.
Ethical Considerations
The study was submitted for the approval of the National Bioethics Committee for Health (Maputo, Mozambique) and then notified the Ethics Committee of the Institute of Hygiene and Tropical Medicine of the New University of Lisbon. This study was performed according to “good clinical practice” (GCP) and all relevant regulatory requirements.
Results
The total number of pregnant women included in the study was 262. Their mean age was 24.88 based on a 95% confidence interval, with the lower limit being 23.74 and the upper limit being 26.02, the median was 24, and the mode was 23. RPR non-specific and Rapid syphilis test 3.0 SD BIOLINE were reactive in 31/262 samples of pregnant women (11.8%). The SD antibody specific test was reactive in 74/262 samples (28.2%) and the non-specific one (RPR) was non-reactive in 43/74 samples (58.1%), as described in Table 1.
| Test Result | Rapid Test Results (Rapid syphilis test 3.0 SD BIOLINE) | Total | |||||
|---|---|---|---|---|---|---|---|
| Non-reactive | Reactive | ||||||
| N | % | N | % | N | % | ||
| RPR Result | Non- reactive | 188 0 | 100 0 | 43 31 | 58. 1% 41. 9 % | 231 31 | 88.2 11.8 |
| Reactive | |||||||
| Total | 188 | 100 | 74 | 100 | 262 | 100 |
Table 2: Results of specific tests (Rapid syphilis test 3.0 SD BIOLINE) and non-specific (RPR) for the detection of antibodies ag
Of the 262pregnant women studied, 137/262(52.2%) were in the age group between 18-25years, 79/262(30.2%) between 26-30years, 35/262(13.4%) between 31-35years, 10/262 3.8%) between 36-40 years and 1/262(0.4%) was over 40years. Of the 137pregnant women who were in the age group between 18-25years, 41/137(29.9%) were reactive and 96/137(70.1%) non-reactive; 21/79(26.6%), 8/35(22.9%) and 3/10(30%) of the reactive were in the age groups between 26-30years, 31-35years and above 36years, respectively. In the case of women with non-reactive samples, 58/79(73.4%), 27/35 (77.1%) and 7/10(70%) were between 26-30years, 31-35years and above 36years, respectively (Table 2).
Regarding the educational level of the 262women studied, 123/262(46.9%) attended primary education, 103/262(39.3) attended secondary education, 28/262(10.7) attended higher education and 8/262 (3.1%) did not attend any level of education. Among the women who attended the primary level, 53/123(43.1%) had reactive samples; and in 70/123(56.9%) of these women the samples were non- reactive; in those who attended the secondary education in 15/103(14.6%) pregnant women the samples were reactive, whereas in 88/103(85.4%) they were non-reactive; regarding the ones who have attended higher education, 6/28 (21.4%) samples showed reactivity whereas in 22/28(78.6%) no anti-T. pallidum antibodies were detected in their samples (Table 2).
Among the 262pregnant women studied, 35/262(13.4%) were teachers, 186/262(71%) domestic servants, 26/262(9.9%) students, 9/262(3.4%) unemployed and 6/262(2,3%) belonged to other professional categories. Of the pregnant women who reported being domestic servants, 57/186(30.6%) had reactive samples, while 129/186 (69.4%) had non-reactive samples; 8/35(22.9%) of the pregnant women were reactive and 27/35(77.1%) non-reactive in the teachers’ group. The number of female students who presented reactivity in their samples was 7/26(26.9%), while 19/26(73.1%) had non-reactive tests; 2/9(22.2%) of those who had reactive and 7/9(77.8%) of those who had non- reactive were unemployed. For women who belonged to other professional categories other than those mentioned above or who were not domestic servants, 6/6(100%) had non-reactive samples, none of which had reactive samples (Table 2).
Monthly, 181/262(69.1%) women had a monthly income between 1000- 3000MZN, 18/262(6.9%) from 4000- 7000MZN, 19/262(7.3%) between 8000-10000 MZN, 8/262 3%) had income above 10000MZN and 36/262(13.7%) had no monthly income. The tests were reactive in samples of 52/181(28.7%) with monthly income between 1000- 3000MZN, 7/18(38.9%) of 4000-7000MZN, 6/19(31.6) 8000-10000MZN, 0/8(0%) had an income above 10000MZN and 9/36(25%) did not have any monthly income. In women with non-reactive samples 129/181(71.3%), 11/18(61.1%),
13/19(68.4%), 8/8(100%) and 27/36(75%) had, respectively, a monthly income between 1000- 3000MZN, 4000-7000MZN, 8000-10000MZN and no income (Table 2). If we look at the type of religion of the women included in the study, 162/262(61.8%) professed Protestantism, 80/262(30.6%) Catholicism and 20/262(7.6%) the Muslim faith Regarding Protestant women, 45/162(27.8%) had reactive samples; in 117/162(72.2%), they were non- reactive; 25/80(31.3%) with reactive and 55/80(68.7%) non-reactive samples were Catholic women; the number of Muslim women who presented reactivity was 4/20(20%); and pregnant women with non-reactive samples, 16/20(80%) were Muslims (Table 2).
As for the languages spoken, the Cisena, Ndau, Machuabo, Emakhuwa, Cinyungwe, Xitswa and Xichangana languages were spoken respectively by 70/262(26.7%), 90/262(34.4%), 29/262(11.1%), 26/262(9.2%), 13/262(5%), 15/262(7.2%), 4/262(1.5%) study participants. Other languages were spoken by the remaining 15/262(5.7%) women. If we consider women whose samples showed antibodies against T. pallidum, 27/70(36.5%), 23/90(26.6%), 9/29(3.4%), 7/26(26.9%), 5/13 38.5%)
2/15(13.3%) and 1/4(25%) spoke Ndau, Machuabo, Emakhwa, Cinyungwe, Xitswa and Xichangana languages, respectively. These same languages were spoken by 43/70(61.4%), 67/90(74.4%), 20/29(69%), 19/26(73.1%), 8/13(61.5%), 13/15(86.7%) and 3/4(75%) participants with non-reactive samples (Table 2).
In this study, 170/262(64.9%) pregnant women were living with someone has husband and wife, of which 48/170(28.2%) had reactive samples and 122/170(71.8%) non-reactive and 92/262(35.1%) of pregnant women who were not living with someone has husband and wife, 26/92 samples (28.3%) detected antibodies against T. pallidum, which did not occur in 66/92(71.7%) (Table 2).
Of the total number of pregnant women included in the study, 62/262(23.7%) were in their first gestation and in 200/262(76.3%) in their second or more. The antibody test was reactive in the blood of 18/62(29%) women who were in the first gestation and 56/200(28%) in the second or more, being non-reactive in 44/62(71%) and 144/200(72%) pregnant women who were respectively in the first and second or more gestations (Table 2).
| Age of the Participants | Reactive women N | Non-Reactive Women | ||
|---|---|---|---|---|
| N | % | N | % | |
| 18-25 | 41 | 55,4 | 92 | 51.0 |
| 26-30 | 21 | 23,4 | 58 | 31.0 |
| 31-35 | 8 | 10,8 | 27 | 14.3 |
| 36-40 | 3 | 4,1 | 7 | 3.7 |
| >40 | 1 | 1,4 | 0 | 0.0 |
| Total | 74 | 100 | 188 | 100 |
| Level of Education | N | % | N | % |
| Primary level | 53 | 71,6 | 70 | 37.2 |
| Secondary level | 15 | 20,3 | 88 | 46.8 |
| High Education | 6 | 8,1 | 22 | 11.7 |
| No Education | 0 | 0 | 8 | 4.3 |
| Total | 74 | 100 | 188 | 100 |
| Participants occupations | N | % | N | % |
| Domestic servant | 57 | 77 | 129 | 68.6 |
| Teachers | 8 | 10,8 | 27 | 14.4 |
| Students | 7 | 9,5 | 19 | 10.1 |
| Unemployed | 2 | 2,7 | 7 | 3.7 |
| Others | 0 | 0 | 6 | 3.2 |
| Total | 74 | 100 | 188 | 100 |
| Monthly income (MZN) | N | % | N | % |
| 1000-3000 | 52 | 70.3 | 129 | 68.6 |
| 4000-7000 | 7 | 9.5 | 11 | 5.9 |
| 8000-10000 | 6 | 8.1 | 13 | 6.9 |
| Above 10000 | 0 | 0 | 8 | 4.3 |
| No income | 9 | 12.1 | 27 | 14.3 |
| Total | 74 | 100 | 188 | 100 |
| Ethnicity | N | % | N | % |
| Sena | 27 | 36,5 | 43 | 22.9 |
| Ndau | 23 | 31,1 | 67 | 35.6 |
| Macua | 7 | 9,5 | 19 | 10.1 |
| Nhúngue | 5 | 6,8 | 8 | 4.3 |
| Matsua | 2 | 2,7 | 13 | 6.9 |
| Changana | 1 | 1,4 | 3 | 1.6 |
| Machuabo | 9 | 12,2 | 20 | 10.6 |
| Other | 0 | 0 | 15 | 8.0 |
| Total | 74 | 100 | 188 | 100 |
| Religião | N | % | N | % |
| Protestants | 45 | 60,9 | 117 | 62.2 |
| Catholic | 25 | 33,9 | 55 | 29.3 |
| Muslim | 4 | 5,4 | 16 | 8.5 |
| Total | 74 | 100 | 188 | 100 |
| Marital status | N | % | N | % |
| Single | 26 | 35,1 | 64 | 34 |
| Married | 48 | 64,9 | 122 | 64.9 |
| Other | 0 | 0 | 2 | 1.1 |
| Total | 74 | 100 | 188 | 100 |
| Gestation | N | % | N | % |
| First | 18 | 24,3 | 44 | 23.4 |
| Two or more | 56 | 55.7 | 144 | 76.6 |
| Total | 74 | 100 | 188 | 100 |
Table 3: Socio demographic characteristics of study participants.
According to Table 3, 222/262(84.7%), 32/262(12.2%) and 8/262(3.1%) pregnant women went to their first antenatal clinic, in the first, second and third trimesters, respectively. Of the 222 women who went to their first antenatal clinic in the first trimester, 60/222(27 %%) samples were reactive, while 162/222(72.9%) did not show reactivity; 12/32(37.5%) and 2/8(25%) samples were reactive and 20/32(62.5%) and 6/8(75%) non-reactive belonging to the women who went to their antenatal clinic in the second and third trimesters of pregnancy (Table 3).
| Trimesters of Pregnancy | N | % |
|---|---|---|
| First trimester | 60 | 81. 1 |
| Second trimester | 12 | 16. 2 |
| Third trimester | 2 | 2.7 |
| Total | 74 | 100 |
| Treatment | N | % |
| One dose | 11 | 35.5 |
| Two doses | 8 | 25.8 |
| Three doses | 12 | 38.7 |
| Total | 31 | 100 |
Table 4: Women’s pregnancy trimesters with rapid reactive syphilis test.
Women with Rapid syphilis test 3.0 SD BIOLINE and RPR reactive samples were given three doses of penicillin in 12/31(38.7%) of these women, two doses to 11/31(35.5%), and one dose to 8/31(25.8). Only two partners were tested for syphilis and treated with three doses, 2/31(6.5%). The remaining patients did not show up at the sanitary unit for diagnosis and treatment, although being notified (Table 4).
HIV/syphilis co-infection was detected in 20/63(31.7%) of HIV-positive pregnant women, of which 8/20(40%) had active syphilis. In this study, the number of non-reactive women for HIV-positive in the anti- T. pallidum antibody test was 54/74(73%) and in the participants with reactive POCT was (74), anti- HIV test was reactive in 20(27%), as described in table 13. Regarding only to active syphilis, the number of HIV cases in these participants was 8/31(25.8%), being 23/31(74 %) in those in which active syphilis was not diagnosed (Table 5).
| Results | Syphilis Results | Total | |||||
|---|---|---|---|---|---|---|---|
| Non-reactive | Reactive | ||||||
| N | % | N | % | N | % | ||
| HIV Results | Non-reactive | 145 43 | 77.1% 22.9% | 54 20 | 73.0% 27.0% | 199 63 | 76.0% 24.0% |
| Reactive | |||||||
| Total | 188 | 100.0% | 74 | 100.0% | 262 | 100.0% |
Table 5: Relationship between the results of HIV and T. pallidum antibodies detection tests in pregnant women.
Discussion
In the study, it was verified that the greater percentage (55.4%) of the women were in the age group between 18- 25 years and the smaller percentage (4.2%) over 36 years old, as in the results obtained in the retrospective study, so that the comparison of the results on the age of the pregnant women was previously performed, when the data from the retrospective study were discussed.
The prevalence of anti-T. pallidum antibodies in pregnant women observed at the antenatal care at Ponta Gêa Health Centre from April to June 2016 was 11.8%, being above the predicted average in the last round of epidemiological surveillance where the prevalence for this region of the center of the country was 2% [23], and was also higher than the 9%, described in the 2007 epidemiological surveillance round for this province [24]. In a study conducted in Mozambique in the province of Sofala, the prevalence was 9.5% Luján et al., Zambia 9.3% [25] and Tanzania 7.3% [26]. However, this prevalence was lower than in other studies, for example, a study carried out in rural areas of southern Mozambique, where prevalence was 12% [27]. However, the Ministry of Health report estimated a prevalence of syphilis of 15% for Sofala province [28].
This prevalence of 11.8% is determined simultaneously by the reactivity of a treponemal and a non-treponemal test and will therefore be the cases of active syphilis. However, there were more than 43 pregnant women whose samples were reactive only by Rapid syphilis test 3.0 SD BIOLINE, which probably had syphilis in the past that was treated. Thus, if we consider the reactive samples in one or other test, the prevalence of the active and passive set of infection increases to 28.2%. There were no big differences regarding the relationship between the age groups and reactivity in the search for anti- T. pallidum antibodies, although the highest prevalence was found in the age groups of 18-25 and above 36 years.
There are more unemployed female people and the gender parity index can reflect the different opportunities in different socioeconomic sectors. The disparity in the labour market may also be related to the differences in the profile of people and skills, as well as in the level of education, which is generally lower in women. Hence, the gender disparities in the unemployment rate, is by far higher in women. Whatever may lead to this inequality, in the provision of social services, as well as in the economic sectors as in the labour market, it always affects negatively the human development [29].
In this study, the higher percentage (77%) of pregnant women with reactive result by syphilis rapid test were also housewives, whereas the unemployed ones had the least number of reactive samples (2.7%) Other studies performed in other countries such as China [30], Brazil [31], and Ethiopia [32].
Discordant results were found in the last round of epidemiological surveillance in the country conducted in 2009, where the result showed higher seroprevalence in women who were domestic servants or housewives [23]. Perhaps this disagreement of the results is related to the fact that, as mentioned above, the researchers of the epidemiological surveillance round have included in the group of domestic servants women who do housework at home.
The majority of women (70.3%) had a monthly income between 1000-3000 MZN, and 12.4% did not have any. Public sector wages serve as an indicator of the rest of the labour market, and so the public sector is a reference for the Mozambican labour market that the adjustment of other private sectors always occurs after the approval of the minimum wage by the Government, usually in April of each year. The minimum wage in the civil service in Mozambique is fixed at 2270 MZN. In Mozambique, the occupational categories with the best salary are those of the specific career, such as magistracy, telecommunications and inspection. The careers with the lowest wages are, curiously, the most important sectors such as agriculture, health and education [24]. A study in Ethiopia revealed results similar to this, since most women had a monthly income below 1000 ETB [32]. In China [30] it was shown that most of the women had no monthly income and among those who had the majority, was below 1000 RMB and in Brazil it was below three minimum wages [33, 34]. There appeared to be no relationship between the monthly income of these women and the presence of anti-T. pallidum antibodies, although it is necessary to analyze a larger number of individuals to reach a definitive conclusion on this subject.
It was found that (46.6%) of the women attended primary education, very close to those who reported having secondary education. In this study, the number of women with higher education was high (10.7%), while 3.1% of pregnant women did not have any level of education. Data that was published by the Institute of Statistics of Mozambique show that the majority of the population (28.3%) of Beira city that attends school completed the primary level and a lower percentage (0.6%) of this population of the same city completed the higher level [35]. According to INSIDA [36], in the final report of the national survey of prevalence, Behavioural risks and information on HIV/AIDS in Mozambique, about 3 out of 10 women (29%) do not have any level of education. It should be noted that 43.1% of the pregnant women who attended the primary level had reactive samples, being the group with the highest infection by T. pallidum, followed by those with higher education (21.4%).
Results from other countries also showed a higher seroprevalence of syphilis in pregnant women who had a level of education below the eighth year of school [32, 37, 38, 31]. The last round of epidemiological surveillance in 2009 demonstrated a higher seroprevalence in pregnant women without any level of education, similarly to four other studies conducted in China [30], Argentina [39], and Tanzania [36, 40].
Regarding religious worship, 61.8% professed Protestantism, 30.5% Catholicism and 7.6% Muslim religion. These results are similar to those published by the Mozambican National Institute of Statistics, according to which the largest percentage (36.9%) of the Beira population attends Protestant churches and the lowest percentage (6.5%) the Islamism [35]. Regarding the relationship between religion and reactivity of serological tests, 60.9% of the women followed during the study with reactive results were Protestants and 5.4% were Muslims.
The largest percentage (36.4%) of women spoke Cisena language, and only 1.4% of these women spoke Chichangana language. These results are in agreement with the information available in the government portal of the Sofala province, where it is described that Sena is one of the most representative ethnic groups. According to the INE in the general census of the population and housing of 1997, 1, 289, 3091 people speak Cisena throughout the Mozambican territory, distributed by four Provinces, with Sofala province having the highest percentage (604,690), which corresponds to 46.9% of the total population, compared to the other three provinces where the this language is spoken, namely Manica, Tete and Zambézia [29]. Different results were obtained in a study conducted in a rural area in southern Mozambique, since a larger percentage (79%) of women spoke Chichangana, the language of the natives of this province. However a smaller percentage of individuals spoke other languages [27].
In the prospective study, 64.9% of the participants lived with their partners has husband and wife. If instead of considering the fact that these women living only with someone has husband and wife, these women were married, the results would certainly have been different, since the data of the INE in 2012 indicate that the Beira city has 12.3% married individuals. This means that the individual contracted civil or religious marriage and lives with his/her partner [35].
In this study, and as discussed in the last Round of Epidemiological Surveillance conducted in the country, the highest seroprevalence of anti-T. pallidum antibodies were found in pregnant women who were living with their partners has husband and wife or who were married, respectively [23]. Similar results have been described in publications of other authors [30, 40].
However, there were published results that reached different conclusions, as was the case of a study in Tanzania that showed that the reactivity in the tests for syphilis diagnosis was not influenced by the civil status in that population [26], as well as in another study in Brazil in which women living alone or with their relatives were the most infected [38].
Among the study participants, 76.3% had one or more gestations, which had a reactive test in a large percentage (55.7%) when compared to those who were pregnant for the first time (24.3%). These results are consistent with the results of the 2009 epidemiological surveillance round, in which a higher seroprevalence of syphilis was found in pregnant women with two or more gestations [23]. Other studies have shown similar results: in Argentina the largest number of pregnant women infected was found in those who had had two or more gestations Menéndez C, et al. [27]; in Tanzania and Ethiopia in more than five gestations (32 and 40) and in Brazil in those with four or more gestations [31]. This study found that the vast majority of women (81.1%) went to antenatal clinics during the first trimester of pregnancy, with 15.3% only attending antenatal clinics in the last two trimesters of pregnancy. In Brazil, were verified similar results to these, with respect to a large percentage of women going to their first antenatal clinic during the first trimester [38, 31]. Contrary to these, in another study conducted in the same country the highest percentage of pregnant women went to the first antenatal clinic in the second trimester of the gestation [37].
In Mozambique, around 1 million women visit the antenatal clinic each year and the recommendation is that screening for syphilis should be carried out in all women at the first antenatal clinic in the health units with laboratory capacity [38]. In this study all women were tested for syphilis at their first antenatal clinic. Most women with reactive Rapid syphilis test 3.0 SD BIOLINE were diagnosed in the first trimester.
A large proportion of the women with Rapid syphilis test 3.0 SD BIOLINE and reactive RPR (61.3%) were treated at lower doses than the recommended ones, and only the correct dose was given to 38.7%(12/31), i.e. three doses of antibiotic, which is not in accordance with international and Mozambique standards, as mentioned above. This situation of inadequate treatment also exists in other countries, especially in countries where the access to health care is deficient in certain populations. For example, in Brazil, only 38.8% of pregnant women with rapid tests for syphilis diagnosis were treated with three doses of benzathine penicillin and there was no information available on the therapeutics performed in 28% of pregnant women [37].
In relation to sexual partners, only two were tested and treated with appropriate doses. The remaining ones did not show up at the health unit despite being notified, which suggests the need to invent new methods that would make notifications more effective. It is often very complicated to monitor and treat sexual partners and this situation is common around the world. However, the situation generally gets worse in countries with poor resources. In the study of 10.5% of sexual partners of pregnant women were treated with three doses of penicillin, and no information was available on the remaining ones [37]. Also another study reported that although 71.7% of sexual partners of women with reactive tests were treated, only 56.1% were treated adequately. In addition, the vast majority of male partners was not treated simultaneously with their female partners (81.8%), which could lead to reinfection and transmission to newborns [31].
Antibody testing for HIV was reactive in 24% of the study participants. In this study, the reactivity rate in the Rapid syphilis test 3.0 SD BIOLINE test in women infected by HIV was 31.7%, of which a large percentage had active syphilis. It also demonstrates once again the great relationship between these two infections and that syphilis may be a marker/ pathfinder for the presence of HIV infection, since 27% of women with anti-T. pallidum antibodies were infected with this virus. There were no significant differences in co- infection rates among participants with active and treated syphilis.
Conclusion
In the study the age group of women whose samples were the most reactive for anti-T. pallidum antibodies were the younger age group, which should be taken into account by the country’s authorities in future prevention and control programs.
The prevalence in the reactivity of women’s samples in the studies is enormous, being up some studies and under the studies carried out within the country, as well as in other African countries. It is necessary to analyze whether the tests used are within the validity period, if the transport and storage conditions are the recommended ones, if the test is carried out and read according to the manufacturer’s recommendations, and if the results are all recorded, or it will be necessary to check all possible situations that may rise unreliable results. Next, it will be necessary to confirm if this situation is punctual and limited to this Health Centre, region or if it is common all over the country.
In the results obtained in the study it should still be commented because it diverted the attention of the health authorities, due to the fact that there were a significant number of women with T. pallidum infection who did not receive treatment. In addition, most of those who received treatment, were not properly treated. The same has happened with regard to the sexual partners of the women studied, which is extremely important, since these men, not being cured, can re-infect women who have sex with them. Here, the situation is even more serious because only two partners had been diagnosed and treated.
The high prevalence of infection with the human immunodeficiency virus (HIV) and or T. pallidum co-infection is also relevant, and the opportunity for counseling for STIs during pregnancy should never be missed. If the results of this study reflect the prevalence of syphilis and the approach to screening, treatment and monitoring of this infection during pregnancy at the country level, so it will be necessary urgent action by the competent authorities to overcome the problems encountered. These will have to address not only the prevention, but also the control and the transmission of these infections to the newborn. All this will only be possible through a plan of action and advocacy, with financial investment and that must be monitored, without which no objective will be achieved.
Acknowledgment
A massive thank you to all who collaborated to carry out this research, namely: Pregnant women attended at the antenatal clinic at Ponta Gêa Health Centre who participated in the study. Thanks to the Ministry of Health in particular to the professionals of Ponta Gêa Health Centre by their technician support. The Pedagogical University for the research funding.
References
-
Galban E, Benzaken AS (2006) Syphilis Situation In 20 Latin American and Caribbean Countries: Year 2006. Artigo, pp: 1-7.
-
(2008) Eliminação Mundial Da Sífilis Congénita: Fundamento Lógico E Estratégia Para Acção. Organização Mundial da Saúde (OMS), pp: 1-46.
-
Ferreira LJM (2013) Infection with Treponema pallidum: Serological Analysis and DNA Research. Dissertation for Master’s Degree in Medical Microbiology. Sexually Transmitted Diseases Unit of the Institute of Hygiene and Tropical Medicine. Rua da Junqueira, pp 55.
-
Mayaud P, Mabey D (2004) Approaches to the control of sexually transmitted infections in developing countries: old problems and modern challenges. Sex Transm Infect 80(3): 174-182.
-
Dupont WD, Plummer WD (2008) PS: Power and Sample Size Calculation (Version 3.1.6).
-
Abdelrahim NA, Ahmed HI, Fadl-Elmula IM, Bayoumi MA, Homeida MM (2016) Sexually transmitted infections other than HIV/AIDS among women of low socio- economic class attending antenatal clinics in Khartoum, Sudan. Int J STD & AIDS 28(8): 781-787.
-
Moodley P, Sturm AW (2000) Sexually transmitted infections, adverse pregnancy outcome and neonatal infection. Semin Neonatol 5(3): 255-269.
-
Chico RM, Mayaud P, Ariti C, Mabey D, Ronsmans C, et al. (2012) Prevalence of malaria and sexually transmitted and reproductive tract infections in pregnancy in sub- Saharan Africa: a systematic review. JAMA 307(19): 2079-2086.
-
Ferlay J, Autier P, Boniol M, Heanue M, Colombet M, et al. (2007) Estimates of the cancer incidence and mortality in Europe in 2006. Ann Oncology 18(3): 581-592.
-
Sankaranarayanan R (2006) Overview of cervical cancer in the developing world. FIGO 6th Annual Report on the Results of Treatment in Gynecological Cancer. Int J Gynecol Obstet 95(1): 205-210.
-
Almeida MFG, Pereira SM (2007) Epidemiological Characterization of Congenital Syphilis in Salvador City Bahia. DST-J bras Doenças Sex Transm 19(3-4): 144-156.
-
(2008) Global prevalence and incidence of selected curable sexually transmitted infections: Overview and estimates. World Health Organization (WHO), pp: 42.
-
Newman L, Kamb M, Hawkes S, Gomez G, Say L, et al. (2013) Global estimates of syphilis in pregnancy and associated adverse outcomes: analysis of multinational antenatal surveillance data. PLoS Med 10(2): e1001396.
-
Revathi TN, Bhat S, Asha GS (2011) Benign nodular tertiary syphilis: a rare presenting manifestation of HIV infection. Dermatol Online J 17(2): 5.
-
Walker DG, Walker GJ (2002) Forgotten but not gone: The continuing scourge of congenital syphilis. Lancet Infect Dis 2(7): 432-436.
-
Cruz J, Lisboa C, Azevedo F (2011) Serological diagnosis of Syphilis- New guidelines. Rev from Soc Port Dermatology and Venereol 69(4): 523-530.
-
Brosco JP, Mattingly M, Sanders LM (2006) Impact of specific medical interventions on reducing the prevalence of mental retardation. Arch Pediatr Adolesc Med 160(3): 302-309.
-
Oliveira VM, Verdasca IC, Monteiro MC (2008) Detecção de sífilis por ensaios de ELISA e VDRL em doadores de sangue do Hemonúcleo de Guarapuava, Estado do Paraná. Revista da Sociedade Brasileira de Medicina Tropical 41(4): 428-430.
-
Temmerman M, Gichangi P, Fonck K, Apers L, Claeys P, et al. (2000) Effect of a syphilis control programme on pregnancy outcome in Nairobi, Kenya. Sex Transm Infect 76(2): 117-121.
-
Myer L, Wilkinson D, Lombard C, Zuma K, Rotchford K, et al. (2003) Impact of on-site testing for maternal syphilis on treatment delays, treatment rates, and perinatal mortality in rural South Africa: a randomised controlled trial. Sex Transm Infect 79(3): 208-213.
-
Varonesi R, Focaccia R (2005) Tratado de Infecciologia. 3 (Edn.), Editora Atheneu. São Paulo.
-
Hawkes S, Matin N, Broutet N, Low N (2011) Effectiveness of interventions to improve screening for syphilis in pregnancy: a systematic review and meta-analysis. Lancet Infect Dis 11(9): 684-691.
-
Da Saúde M (2011) Epidemiological Surveillance of HIV and its Demographic Impact in Mozambique. Group in the fight against HIV/AIDS in Mozambique, Maputo.
-
(2008) HIV Epidemiological Surveillance Round 2007: National Directorate of Medical Assistance, National STI/ HIV/AIDS Control Program. Republic of Mozambique. Ministry of Health (MISAU).
-
Ronald A, Plourde P (1998) Why are syphilis control programs failing?. Int J Infect Dis 2(3): 121-122.
-
Swai RO, Somi GRG, Matee MIN, Killewo J, Lyamuya EF, et al. (2006) Surveillance of HIV and syphilis infections among antenatal clinic attendees in Tanzania-2003/2004. BMC Public Health 6: 91.
-
Menéndez C, Castellsagué X, Renom M, Sacarlal J, Quintó L, et al. (2010) Prevalence and Risk Factors of Sexually Transmitted Infections and Cervical Neoplasia in Women from a Rural Area of Southern Mozambique. Infect Dis Obstet Gynecol 9: 609315.
-
Nhatave I (2006) Saúde Materna em Moçambique Revisão da Literatura, pp: 61.
-
(2015) Women and Men in Mozambique. National Statistics Institute (INE).
-
Zhou H, Chen X, Hong F, Pan P, Yang F, et al. (2007) Risk factors for syphilis infection among pregnant women: results of a case-control study in Shenzhen, China. Sex Transm Infect 83(6): 476-480.
-
Hildebrand VLPC (2010) Congenital syphilis: factors associated with the treatment of pregnant women and their partners/Congenital syphilis: factors associated with treatment of pregnant women and their partners. Rio de Janeiro 9: 73.
-
Melku M, Kebede A, Addis Z (2015) Magnitude of HIV and syphilis seroprevalence among pregnant women in Gondar, Northwest Ethiopia: a cross-sectional study. HIV AIDS (Auckl) 7: 175-182.
-
Assefa A (2014) A Three Year Retrospective Study on Seroprevalence of Syphilis among Pregnant Women at Gondar University Teaching Hospital, Ethiopia. Afr Health Sci 14(1): 119-124.
-
Baretta P (2003) Syphilis: Prevalence in Pregnant Women and Newborns. Work presented to the Federal University of Santa Catarina, for the conclusion of the Undergraduate Course in Medicine. Universidade Federal de Santa Catarina. Florianópolis, pp: 32.
-
(2012) General Population and Housing Census 2017. Instituto Nacional De Estatistica.
-
(2009) National Survey on Prevalence, Behavioral Risks and Information on HIV and AIDS in Mozambique (INSIDA).
-
Santos GC, Borges-Paluch LR, Dos Cerqueir TPS, Passos NCR (2015) Prevalence and Factors Associated with Syphilis in Pregnant Women Attended by Sus in a Municipality of Bahia. Revista Baiana de Saúde Pública 39(3): 529-541.
-
Peeling WR, Htun Y (2004) Diagnostic tools for preventing and managing maternal and congenital syphilis: an overview. Bull World Health Organ 82(6): 439-446.
-
Nonato SM, Melo APS, Guimarães MD (2015) Syphilis in pregnancy and factors associated with congenital syphilis in Belo Horizonte-MG, Brazil, 2010-2013. Epidemiol Serv Saúde 24(4).
-
Manyahi J, Jullu BS, Abuya MI, Juma J, Ndayongeje J, et al. (2015) Prevalence of HIV and syphilis infections among pregnant women attending antenatal clinics in Tanzania, 2011. BMC Public Health. 15: 501.
-
Pereira TM, Fernandes JC, Vieira A P, Basto AS (2007) Tertiary syphilis. Int J Dermatol 46: 1192-1195.
- Are the Vaccines the Only Solution to Prevent the COVID-19 Pandemic? Part Two
- Clinical Characteristics of Women in this New Global Immunodeficiency
- Cell Dynamics in HIV Pathogenesis: Insights and Implications
- Determination of the CDR (CDR1, CDR2) « Complementary- Determining Region Invertebrate Primitive Antibody from Sea Star »
- Prioritizing Care for High-Risk COVID-19 Patients in the EU: 10 Civic Recommendations to the Institutions
- Comprehensive Insights into ModRNA Vaccines: Persistent PP-Spike Recombinant Protein, Hyperimmune/Inflammatory Reactions, Thrombotic Vasculopathy, Chronic Organ Complications and Excess Deaths