Immunological Disorders in Adult Patients with Trichophytia and Microsporia of the Genital Area, Tajikistan
To study the state of the main parameters of immunity in the peripheral blood of adult patients with trichophytia and microsporia of the skin of the genitals and surrounding areas
Introduction
In the first years of the 21st century, there has been a marked decrease in the incidence of trichophytia and microsporia among the child population, while in the adult population there has been an increase, with predominant localization on the skin of the genitals and surrounding areas. This phenomenon is also observed in other Central Asian countries [1, 2].
Disorders in the body’s immune system play a crucial role in the pathogenesis of common and atypical forms of dermatophytia [3, 4]. Successful protection of the patient’s body in response to the penetration of pathogenic fungi is associated with an increase in, first of all, the activity of the cellular link of immunity. CD4 helper and CD8 suppressor subsets of T lymphocytes responsible for formation of cellular immunity or delayed-type hypersensitivity (HPT) recognize antigen (pathogenic fungi) and regulate intensity and nature of immune response [3, 4, 5, 6]. In zooanthroponous dermatophytes, “granulomatous” inflammation develops - the only effective cell-mediated immunological defense [3, 7].
In the available sources we found an article, in which were researched immunological disorders in adults with zooanthroponous forms of inguinal dermatophytia - neutrophilic leukocytosis, a decrease in the relative number of lymphocytes, CD3, CD4, CD8 lymphocytes, an increase in IgM and IgG were detected in peripheral blood [8].
Purpose: Study the state of the main parameters of immunity in the peripheral blood of adult patients with trichophytia and microsporia of the skin of the genitals and surrounding areas.
Research Materials and Methods
137 patients with trichophytia and pubic microsporia were examined, of which 88 (64.2%) were men, 49 (35.4%) were women. The age of patients ranged from 16 to 40 years, the average age of patients was 28.2 + 1.7 years. The duration of diseases ranged from 2 weeks to 5 months, averaging 6.9 ± 0.2 weeks. When analyzing anamnestic data, it turned out those patients contracted mycoses in various ways, as shown in Figure 1.
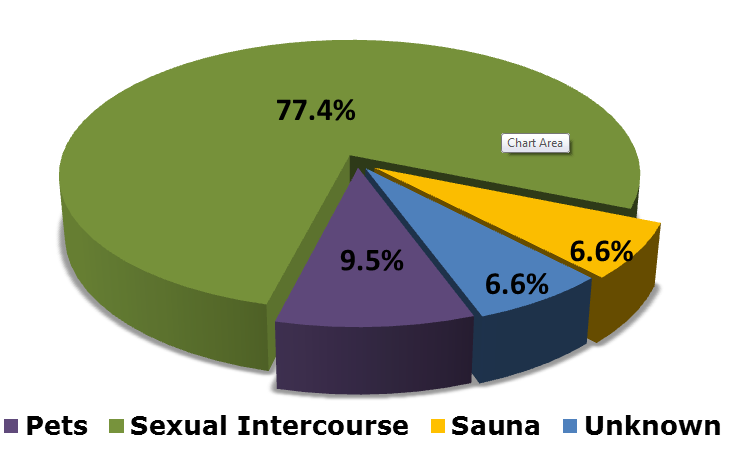
As shown in Figure 1, 77.4% of patients (106 individuals; 62 men, 44 women) associated their disease with sexual contact: 58 (42.3%) patients (35 men, 23 women) contracted from accidental sexual partners, 48 (35.1%; 27 men, 21 women) - from spouses or cohabitants. There were 24 sexual couples, 17 of them married. 9.5% (n = 13) of patients were infected from pets (9 patients - from cattle and small cattle, when caring for them, 4 - from cats/kittens that were taken to their bed), 6.6% (n = 9) - in a sauna or bath, probably, according to patients, through a towel, in 6.6% (n = 9) cases - the route of infection could not be established. 39 (28.5%) of patients had a messy sexual lifestyle.
The diagnosis of mycosis was established by microscopic detection of spores and mycelium of Trichophyton ectothrix or Microsporon fungi in the hair and scales of the skin of the pubic region, lower abdomen, inguinal and other regions. A luminescent study was conducted by us to confirm or exclude the disease or microsporia. A cultural study allows you to determine the genus and type of causative agent, to determine latent dermatomycosis, the wearing of dermatomycoses by healthy persons, which is important for the correct conduct of anti-epidemic measures.
The quantitative content of CD3, CD4, CD8 and CD20 lymphocytes was determined by the immunofluorescence method “Status” using a set of monoclonal and polyclonal antibodies, the quantitative content of total immunoglobulins A, M and G in blood serum by the immunoenzyme method, circulating immune complexes by the precipitation method of polyethylene glycol according to Grinevich and Alferov, 1981, and phagocytic number (FN) and phagocytic activity of neutrophil leukocytes (PANL) - according to Park, 1972. The serum content of proinflammatory (interleukins 1β, 6) and anti-inflammatory (interleukins 10) cytokines was determined by the immune-enzyme method using the Immuno-BEST system (Novosibirsk). To compare the obtained immunological results, 30 healthy people aged 20 to 35 years were examined.
All patients underwent a laboratory examination for STI at the time of initial treatment and in dynamics 1 and 2 months after the end of treatment. All patients underwent a mandatory serological examination for syphilis and HIV infection. Statistical processing of the research results was carried out by the method of variation statistics. Determined the arithmetic mean (M) and errors of the mean (±). The reliability of differences in quantitative indicators in groups was determined by Student’s t-test (t): at p less than 0.05, the difference was considered significant.
Results
The results of the immunological studies are shown in Table 1.
| Indicators | Control group | Patients | Р |
|---|---|---|---|
| Lymphocytes, abs. | 2122 ± 149 | 1947 ± 112 | > 0,1 |
| Lymphocytes, % | 31,7 ± 1,8 | 29,3 ± 1,3 | > 0,1 |
| CD (Т-lymphocytes), % 3 | 69,8 ± 2,8 | 63,6 ± 2,1 | > 0,1 |
| CD (Т-helpers), % 4 | 42,8 ± 2,2 | 36,3 ± 1,5 | < 0,02 |
| CD (Т-suppressors), % 8 | 27,3 ± 1,7 | 23,7 ± 1,3 | > 0,1 |
| CD / CD 4 8 | 1,57 ± 0,12 | 1,54 ± 0,11 | > 0,1 |
| CD (В-lymphocytes), % 20 | 15,2 ± 1,2 | 17,2 ± 1,1 | > 0,1 |
| IgA, g/l | 2,42 ± 0,17 | 3,08 ± 0,13 | < 0,01 |
| IgM, g/l | 1,86 ± 0,14 | 2,43 ± 0,12 | < 0,01 |
| IgG, g/l | 12,8 ± 0,9 | 15,7 ± 1,1 | > 0,1 |
| CIC, g/l | 2,06 ± 0,16 | 2,81 ± 0,13 | < 0,01 |
| PANL, % | 75,3 ± 5,4 | 53,2 ± 4,2 | < 0,01 |
| FN | 5,5 ± 0,3 | 4,2 ± 0,2 | < 0,01 |
| IL-1β | 1,88 ± 0,15 | 2,85 ± 0,21 | < 0,01 |
| IL-6 | 2,86 ± 0,18 | 3,98 ± 0,23 | < 0,01 |
| IL-10 | 7,33 ± 0,46 | 5,56 ± 0,32 | < 0,01 |
Table 1: Immunological indicators in patients with smooth skin dermatophytia of atypical localization. P-reliability of differenc
Table 1: Immunological indicators in patients with smooth skin dermatophytia of atypical localization. P-reliability of difference Table 1 data show that in peripheral blood of patients with zooanthroponous smooth skin trichomycoses of atypical localization compared to healthy people, lymphocyte inhibition was detected, which resulted in a decrease in the number of CD4 (T-helper) lymphocytes (P < 0.02), the content of which was increased in 16 (11.7%) of 137 patients examined, corresponded to the values of healthy people in 33 (24%) patients, lower In the study of CD8- lymphocyte subpopulations, it was found that 34 (24.8%) patients dominated their increased activity, 51 (37.2%) patients registered their normal functional activity, 52 (37.9%) - decreased. 25 (18.3%) patients showed an increased content of CD3 lymphocytes, 37 (27%) - reduced, 75 (54.7%) did not differ from the data of the control group.
From the side of indicators of humoral immunity, an increase in their activity is determined, which was manifested by an increase in serum content (by 27%, P < 0.01) IgA and IgM (by 31%, P < 0.01), as well as the CIC (by 36%, P < 0.01).
The IgA rate in 64 (46.7%) patients was higher than in healthy people, in 52 (37.9%) - within the norm, in 21 (15.3%) - lower. An increase in the number of IgM was observed in 61 (44.5%) patients, a decrease in 14 (10.2%), and in 62 (45.3%) within normal values. Increased CIC figures are determined in 66 (48.2%) patients, decreased in 20 (14.6%), normal in 51 (37.2%). The content of non-specific factors of protection of the body of PANL and FN was reduced respectively in 69 (50.4%) and 63 (46%) patients, within normal values in 45 (32.8%) and 41 (29.9%), increased - in 23 (16.8%) and 33 (24.1%).
Analysis of the state of the examined cytokines showed that the concentration of proinflammatory cytokines IL-1β and IL-6 in the serum of patients with smooth skin mycoses was increased by 52% (P < 0.01) and 39% (P < 0.01), respectively, compared with the control group, and the anti- inflammatory cytokine IL-10, on the contrary, was decreased by 32% (P < 0.01). The IL-1β content was increased in 71
(51.8%) patients, decreased in 24 (17.5%), within the normal range in 42 (30.7%), IL-6 and IL-10 were increased in 58 (42.3%) and 55 (40.1%), decreased in 27 (19.7%) and 25 (18.2%), within the norm - in 52 (37.9%) and 57 (41.6%).
Immunological disorders depended on the age of mycotic infection. In patients with smooth skin trichomycoses of atypical localization, already in the first month of the disease, violations by the humoral link of immunity are detected, manifested in an increase in IgA (P < 0.05), IgM (P < 0.05) and circulating immune complexes (CIC) (P < 0.02), a decrease in PANL (P < 0.02) and FN (P < 0.05). With the duration of the pathological process of more than 1 month, inhibition of the activity of the cellular link of immunity is found, characterized by a reliable decrease in the total number of CD3 lymphocytes (P < 0.05), their CD4 subpopulation (P<0.02), a continuing tendency to decrease the absolute and relative number of lymphocytes and their T-suppressor subpopulation. At the same time, the activity of the humoral immunity link continues to increase, as evidenced by an increase over time in serum IgA (P < 0.01), M (P < 0.01) and G (P < 0.02), and a further increase in the number of CIC (P < 0.001). PANL and FN continue to be depressed (P < 0.001 and < 0.01, respectively). Already at the early stages of mycotic infection on smooth skin, patients show an increase in the activity of serum pro-inflammatory cytokines, which was expressed by an increase in their IL-1β (P < 0.02) and IL-6 (P < 0.05) content in the first month of the disease, while simultaneously reducing anti-inflammatory IL-10 (P < 0.05). Over time, the activity of cytokines increases, as evidenced by a further increase in the concentration of IL-1β (P < 0.01) and IL-6 (P < 0.02) in the blood serum of patients with a disease duration of more than 1 month and a more pronounced decrease in their IL-10 content (P < 0.01).
Thus, the study showed that in adult patients with zooanthroponous smooth skin trichomycoses of atypical localization, immunological disorders are observed, characterized by suppression of the activity of the cell link of immunity, phagocytic reactions, anti-inflammatory cytokines and an increase in activity of humoral and pro- inflammatory cytokines. The inhibition of cellular immunity was accompanied by a deficiency of CD4 lymphocytes, an increase in the activity of humoral immunity by an increase in the content of serum IgA, IgM, as well as circulating immune complexes. Immunological disorders are more pronounced in patients with disease duration of more than 1 month, with severe suppressive forms of mycoses.
References
-
Abidova, ZM, Nurmatov UB (2009) Clinical course and treatments for zooanthroponous trichophytia in adults with localization of lesions in the pubic region. Problems of medical mycology. 11(2): 31-35.
-
Khismatullina ZR, Medvedev YA (2013) Zoanthroponous trichophytia. Ufa: State Unitary Enterprise IPK of the Ministry of Internal Affairs for the Republic of Belarus “TID”, pp: 112.
-
Goldsmith LA (2018) Fitzpatrick Dermatology in Clinical Practice, pp: 1072.
-
Karibaeva AT (2010) Modern features of the clinic, epidemiology, immune mechanisms of trichophytia, microsporia and improvement of therapy. Sciences, pp: 41.
-
Abidova ZM, Imamov OS, Rakhimov IR (2017) The nature of the immune response in zooanthroponous trichophytia. Dermatovenerology and aesthetic medicine, pp: 92-93.
-
Usubaliyev MB, Kozmina YV (2013) Pathomorphological changes and results of complex treatment of inguinal dermatophytia. Bulletin of KGMA 4(1): 114-120.
-
Usubaliyev MB, Kolybekova GM, Kasymova AZ (2013) Clinical-epidemiological and etiological features of inguinal dermatophytia 3: 115-119.
-
Shchelkunova OA, Reshetnikov TB (2012) Features of immune status in patients with microsporia and its correction. Medicine and education in Siberia 2: 49-53.
- Are the Vaccines the Only Solution to Prevent the COVID-19 Pandemic? Part Two
- Clinical Characteristics of Women in this New Global Immunodeficiency
- Cell Dynamics in HIV Pathogenesis: Insights and Implications
- Determination of the CDR (CDR1, CDR2) « Complementary- Determining Region Invertebrate Primitive Antibody from Sea Star »
- Prioritizing Care for High-Risk COVID-19 Patients in the EU: 10 Civic Recommendations to the Institutions
- Comprehensive Insights into ModRNA Vaccines: Persistent PP-Spike Recombinant Protein, Hyperimmune/Inflammatory Reactions, Thrombotic Vasculopathy, Chronic Organ Complications and Excess Deaths