Searching for Etiopathophysiological Links for ‘Long Covid’
Introduction: The Long Covid Syndrome: The post-acute sequelae of COVID-19 (PASC) or ‘Long Covid’ is a varying, relapsing, and remitting disorder that may follow recovery from acute infection with SARS-CoV-2 in some patients and last for a variable period. It has a protracted course culminating as lingering and incapacitating illness predisposed by certain constitutional factors and comorbidities. Akin to COVID-19, it primarily affects the respiratory system, but other systems such as neurologic, cardiologic, hepatic, renal and pancreatic, and cutaneous systems may be involved. As the infection can harm the immune system, various organs including lungs fall prey to the aberrant immune response. Etilogical Correlates and Pathogenesis: Long Covid is a multisystem disorder entailing multiple symptoms related to various organs. There are several theories about the etiology of Long Covid such as continuing presence of the virus and its biologically active fragments, reinfection with the same or a different variant, dysfunctional immune reactions leading to a chronic inflammatory state, an ill-defined condition exhibiting symptoms of myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) suggestive of a complex, multisystem disorder, post-traumatic stress following severe COVID-19 illness and critical care issues, and aftermath resulting due to disturbed microbiota in gut, lungs, and other organs. Long Covid Pathogenesis: New Insights: The SARS-CoV-2 infection activates the humoral immunity leading to formation of antigen-antibody complexes and the antigen-antibody reactions, which may propagate to organ damage. Simultaneously, viral superantigens may overstimulate immune responses, inducing negative feedback loops to hamper immune function and allow the virus to persist and replicate. The persistent virus may contribute to long Covid. There may develop various autoantibodies causing tissue injury and fibrosis in lungs and other organs. The Altered Microbiome leading to the microbial dysbiosis has also been implicated in persisting inflammatory processes culminating as Long Covid. Conclusion: Therapeutic Considerations: With expanding awareness, it has been recommended that all patients after recovery from COVID-19 should have access to healthcare. On the practical side, there are being established clinics for people with Long Covid backed by multidisciplinary teams for supportive and specific treatment and follow up. The anti-fibrotic and anticoagulant agents may be helpful in preventing further lung damage and thrombotic episodes. The role of a COVID-19 vaccine in preventing Long Covid is not known, but it may be helpful in reducing morbidity. The strategies to improve the intestinal dysbiotic microbiota through probiotics and microbial transplant appear promising.
Introduction-The Long Covid Syndrome
Post-Acute Sequelae of COVID-19 (PASC)
The post-acute sequelae of COVID-19 (PASC) or ‘Long Covid’ is a varying, relapsing, and remitting disorder that may follow recovery from acute infection with SARS-CoV-2 in some patients and last for a variable period. The patients report various symptoms, such as fatigue, dry cough, shortness of breath, headaches, and muscle aches [1]. There are respiratory, cardiovascular, neurological, gastrointestinal, and urological symptoms in unpredictable combinations. In fact, the list of Long Covid symptoms is enormous and Akrami, et al. [2] have reported as many as 205 symptoms in their study of over 3,500 people. The most common symptoms reported in the study were fatigue, post-exertional malaise, and cognitive dysfunction. Further, these symptoms may fluctuate, and there are phases of improvement punctuated with relapse [3]. There is a protracted course of the disease following SARS-CoV-2 infection from acquiring the virus to Long Covid, culminating as lingering and incapacitating illness predisposed by certain constitutional factors and comorbidities (Figure 1).
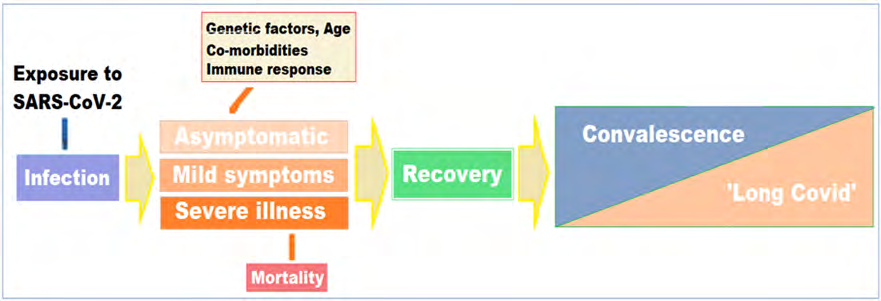
The SARS-CoV-2 virus primarily affects the respiratory system, affecting and damaging lung alveoli. Simultaneously it causes endothelitis and microthrombi, enters the blood vessels and may disseminate in the whole body. It also stimulates the inflammatory milieu in the body, causing significant release of cytokines and chemokines leading to cytokine storm in severe cases. The resultant organ damage takes much longer to recover and is responsible for the symptoms of Long-COVID-19. There is a diversity of human response to the SARS-CoV-2 virus, variable course of COVID-19 illness, and a puzzling array of symptoms of Long Covid. The response to the virus and the disease course, depend on various factors including the constitutional factors including the individual immune status, genetic make-up, and presence of comorbidities. These differences could make certain persons more susceptible to Long Covid [4].
Incidence and Prevalence of Long Covid
The UK Office for National Statistics (ONS) considers Long Covid as persistence of various symptoms for more than four weeks. The UK ONS in a survey, which encompassed over 20,000 COVID-19 patients with +ve test, the prevalence was ~20% at four weeks to ~12% after a period of 20 weeks [5]. As per a rough estimate, over 10% of those infected with SARS- CoV-2 may suffer with Long Covid, which is more common in women than in men. As per the Post-Hospitalisation COVID-19 study (PHOSP-COVID), 23% of women and 19% of men still had symptoms 5 weeks after infection. Further the prevalence has been estimated to be about 20-30% in those who were not admitted to hospital, with at least one enduring symptom one month later and about 10% three months later. For others having been admitted to hospital, it was 50-89% with at least one enduring symptom after two months. In other studies, it has been highlighted that the incidence and prevalence of Long Covid is not predicted by severity of preceding COVID-19 illness [6].
The men with positive COVID-19 test are more likely to suffer with a severe form of the disease, whereas women with a positive test are more likely to get the ongoing symptoms in form of Long Covid. The current data suggest that 70–80% of people experiencing severe acute forms of COVID-19 are men, whereas 70–80% of those suffering from Long Covid are women [7]. In addition, there is a distinctive age distribution and Long Covid is most common in middle-aged people, the prevalence has been reported 25.6% at 5 weeks for those between 35 and 49 years old, and less common in younger people and older people. Among the younger people, such as children aged 2–11, about 9.8% of those who test positive for the virus may have lingering symptoms after at least 5 weeks [8]. There are studies to indicate that the children may suffer with Long Covid [9].
The Enduring Effects of Long Covid
• Effects on Respiratory System The COVID-19 begins as a respiratory disease. Clinically, Long Covid is multi-system inflammatory syndrome (MIS). There may occur delayed manifestations of MIS, due to dysregulated adaptation in various organs. The inflammatory process is manifested as increased CRP, D-Dimer, LDH, Ferritin, and IL-6 [10]. It has been documented that the lung damage gradually reduced over two weeks. Certain COVID-19 patients continue to suffer with fatigue, respiratory and other symptoms long after the recovery period. In fact, a follow up study of hospitalized COVID-19 patients documented that even over 70% of them were having shortness of breath a month after discharge and 13.5% were using oxygen at home [11]. Further, there is evidence from previous coronavirus outbreaks, especially the severe acute respiratory syndrome (SARS) epidemic, suggesting that the effect may last for a variable period and symptoms may linger for years. A study recorded long-term lung damage in SARS caused by hospitalized patients still had visible lesions on their lungs, and 38% had reduced diffusion capacity [12].
Gholamrezanezhad, et al. [13] tracked patients using CT scans to study their lungs and found that lung scans were helpful. They followed up on 33 of them for over a month later and found that more than one-third had tissue death that has led to visible scars. The analysis of lung CT images of these 919 patients from published studies has reported that the lower lobes of the lungs are the most frequently damaged. An Austrian study noted that lung damage lessened with time and 88% of participants had visible damage 6 weeks after being discharged from hospital, but by 12 weeks, this number had fallen to 56%. Defective pulmonary gas exchange is detected through xenon gas radio-diffusion study [14].
• Effects on Other Systems COVID-19 primarily strikes the respiratory system, but as various tissues also harbour the ACE2 receptors, other organs such as heart, brain, and kidneys are also involved. COVID-19 can affect multiple organs such as neurologic, cardiologic, hepatic, renal and pancreatic, and cutaneous systems. As the infection can harm the immune system, various organs including lungs fall prey to the aberrant immune response. Further, some patients recovered from COVID-19 are left with a weakened immune system and decreased immune-system activity leading to a multitude of after-effects [15, 16].
The heart and vasculature are particularly susceptible for over-reactive immune system. During the acute phase of COVID-19, about one-third of patients show cardiovascular symptoms. Some patients also have pulmonary thrombosis. There can result vasculitis, myocarditis, and cardiomyopathy [17]. The patients having pneumonia may be at increased risk of cardiovascular disease 10 years later, as shown by the SARS and MERS data [18]. Many patients experience neurological complications due to inflammation or the virus infecting the brain, such as chronic fatigue, delirium, and the cognitive difficulties, including confusion and memory loss, persisting for a variable period after the acute phase.
Etilogical Correlates and Pathogenesis
The exact cause(s) of the PASC or Long Covid is presently unknown, but the syndrome is likely to have multiple triggers and involve multiple conditions with different associations [7]. With multiple symptoms related to various organs, it seems logical to conclude that long COVID is a multisystem disorder entailing multiple mechanisms [19]. In fact, the etiology of Long-COVID-19 seems to be a continuum of the disease pathogenesis of acute illness. There is likely to be tissue damage due to altered microenvironment due to a sudden spurt in inflammosomes and cytokines. The tissue damage also occurs due to hypoxia and oxidative stress.
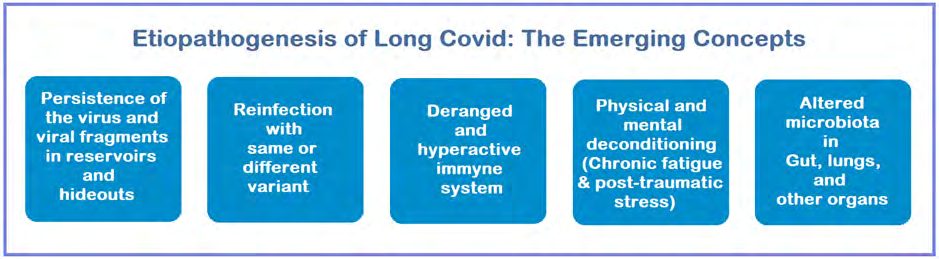
There have been sponsored several theories about the cause of Long Covid such as continuing presence of the virus and its biologically active fragments, reinfection with the same or a different variant, dysfunctional immune reactions leading to a chronic inflammatory state, an ill-defined condition exhibiting symptoms of myalgic encephalomyelitis/ chronic fatigue syndrome (ME/CFS) suggestive of a complex, multisystem disorder, post-traumatic stress following severe COVID-19 illness and critical care issues, and aftermath resulting due to disturbed microbiota in gut, lungs, and other organs (Figure 2). The search for the etiological factors of Long Covid aims to help in its prevention as well as design therapeutic strategies. Further, the understanding of the pathophysiology of Long-COVID-19 is important to predict, prevent and treat long-term consequences of COVID-19.
Persistence of Virus and Viral Fragments
Following the acute course of COVID-19, the SARS- CoV-2 virus may persist and continue to replicate in in cells expressing ACE2 receptors such as endothelial cells. The persistent virus infection could induce both cell damage and direct activation of dendritic cells, which could lead to autoimmunity. In fact, a persistent infection could explain various symptoms of long COVID. Salmon-Ceron et al have reported people who had tested positive for Covid19 and whose symptoms had either lasted longer than two months from initial onset or had recurred [20]. They found that 25% still had positive PCR nose and throat swabs.
Liotti et al. used PCR tests with patients discharged from an Italian hospital deemed to have recovered from COVID-19 and found 17% tested positive [21]. Referring to a number of other publications, Yong’s, et al. [6] also reported that some patients still tested positive for COVID-19 four months later. They also noted the virus has been detected in faeces for up to two months regardless of gastrointestinal symptoms. A persistent virus infection could induce both cell damage and direct activation of dendritic cells, which could lead to autoimmunity. In fact, a persistent infection could explain various symptoms of long Covid. Further, the continuing morbidity may be partly due to a persistent systemic infection indicated by continued virus RNA shedding [22].
Further, if the virus itself is not at work, there is evidence that fragments of the virus, the genomic bits, and the viral non-structural proteins (NSPs) and structural proteins (SPs), can persist for months, might disrupt the body in certain ways even though they cannot infect the cells [23]. It has been suggested that in certain cases, the viral persistence may lead to a specific immune response responsible for Long Covid symptoms. The autoantibodies play a part, with the immune system attacking the various tissues and organs harbouring the viral reservoirs or lingering fragments of viral RNA or proteins contributing to the persisting inflammatory process leading to pericarditis and/or myopericarditis, and inflammation of olfactive bulbs occasionally found in case of persistent or recurrent anosmia.
Further, the SARS-CoV-2 genome has been found in respiratory cells, cells lining the blood vessels, and the syncytia, in Long Covid patients. These histopathologic changes, persistence of the abnormal cells, and the virus- infected cells may be linked with continuance of ongoing viral replication and organ damage, and persistence of long Covid symptoms in those recovered from the disease. Similarly, the SARS-CoV-2 fragments have been found in interstitial cells of the myocardium along with inflammatory changes [24]. In another study, Maiese, et al. [25] has reviewed major autopsy findings associated with CVS in COVID-19 patients from 28 published studies involving 341 cases. They found severe direct endothelial injury associated with intracellular virus, multifocal necrosis, interstitial inflammatory infiltration, myocarditis, pericarditis, and myocardial hypertrophy, along with lymphocytic endotheliitis in various organs such as lung, kidney, liver, and small intestine.
Deranged and Hyperactive Immune System
The deranged and hyperactive immune system is another likely mechanism which entails damaging effects on various tissues and organs. There occurs tissue damage in various organs due to altered microenvironment following altered immunity and perturbed inflammatory Response. Simultaneously, the inadequate immune response may also lead to an auto-inflammatory chronic condition in a genetically predisposed individual [20]. From an immunologic perspective persistent infection and autoimmunity are two distinct mechanisms that could be caused by SARS- CoV-2. Further, Long Covid symptoms may be explained by immune-mediated autonomic instability resulting in physical deconditioning leading to muscle weakness, cardio- respiratory impairment, hypovolaemia, and neuropathy [26]. The inflammatory changes seen in COVID-19 may result in inflammation of blood vessels, myocarditis and arrhythmias which may explain various symptoms and findings in Long Covid [27].
The lung damage and reduced exercise tolerance have been correlated with serum markers of inflammation and mitochondrial stress. Betty Raman, et al. prospectively studied 58 COVID-19 patients post-hospital discharge and 30 comorbidity-matched controls for multiorgan (brain, lungs, heart, liver, and kidneys) magnetic resonance imaging (MRI), spirometry, six-minute walk test, cardiopulmonary exercise test (CPET), quality of life, cognitive and mental health assessments. The study found that at 2-3 months from disease-onset, 64% of patient’s experienced persistent breathlessness and 55% complained of significant fatigue. On MRI, tissue signal abnormalities were seen in the lungs (60%), heart (26%), liver (10%) and kidneys (29%) of patients [28]. The microvascular damage may also be a cause of persistent organ damage in patients with enduring symptoms. The autopsy findings suggest that focal damage of the microvascular pulmonary circulation due to the SARS- CoV-2 virus infection may also be the cause of persistent lung damage in patients who recover from severe COVID-19 [29].
Evans, et al. [8] Studied 1,077 COVID-19 patients, recording symptoms including physical impairments, mental-health difficulties such as anxiety, and cognitive impairments in areas such as memory and language. The researchers also recorded basic information such as age and sex, and biochemical data such as levels of C-reactive protein as a measure of inflammation. The cluster analysis is a mathematical tool to analyse and record identifiable groups of patients with similar epidemiological profiles. The PHOSP-COVID Collaborative Group working to correlate is the evidence of inflammation, cardiovascular affliction, and other changes. Other studies have also documented altered levels of cytokines in the blood samples of Long Covid patients, suggesting the derangement of immune system as well as proinflammatory markers [30].
Chronic Fatigue and Post Traumatic Stress
As such, it is not uncommon for an infection to trigger long-lasting symptoms. A study of 253 people diagnosed with certain viral or bacterial infections found that after 6 months, 12% reported persistent symptoms including disabling fatigue, musculoskeletal pain, neurocognitive difficulties, and mood disturbance [31]. In fact, the percentage is akin to the Long Covid prevalence observed in the United Kingdom by the ONS. Some people with Long Covid may look similar to the ME/CFS but striking difference is that people with Long Covid are more likely to report shortness of breath than are those with ME/CFS [32]. The long Covid is, thus, an umbrella term and there are multiple syndromes under this coalition.
One of the most insidious long-term effects of COVID-19 is severe fatigue manifesting as crippling exhaustion and malaise following recovery from acute infection. In an Italian study involving 143 post-discharge COVID-19 patients, 53% reported fatigue and 43% had shortness of breath for over 2 months [1]. Another study showed that 25% of patients in China had abnormal lung function after 3 months, and that 16% were still fatigued [33]. These symptoms resemble chronic fatigue syndrome, also known as myalgic encephalomyelitis (ME). There are no known biomarkers and diagnosis is based on symptoms.
The clinical condition bears similarity to myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), which was observed after SARS epidemic in Hong Kong. A follow-up study of 233 patients infected with SARS showed that 27% of the patients suffered with ME/CSF [34]. Similarly, in another study, 22 people who recovered from SARS in Toronto still suffered fatigue, aches, depression and altered sleep patterns one to three years later [35]. It was suggested that the symptoms might result from lingering inflammation after the virus was gone, as well as the psychological trauma of the infection.
A subset of patients with prolonged COVID-19 symptoms has been shown to have similarity with ME/CFS [36]. The most commonly reported incapacitating symptom following the COVID-19 is fatigue. A similar symptom occurs following viral infections and was noted after the Spanish Flu pandemic and the more recent SARS, MERS, and Ebola epidemics. Finally, there is possibility of the post- traumatic stress induced by the COVID-19 illness which can be exacerbated by intensive health care (post-intensive care syndrome) received especially for severe or critical disease. The post-traumatic stress can precipitate mental deconditioning, especially in those with previous history of anxiety, depression, insomnia, or other mental health difficulties. The mental deconditioning may be accompanied by physical deconditioning due to a lack of exercise while ill and later during recovery.
The Reinfection with Same or Different Variant
The hypothesis about reinfection with same or Different Variant of SARS-CoV-2 has been propagated to explain the persisting symptoms in Long Covid. The partial and/or short-lived immunity, and immune suppression, as induced by its super antigens, also plays a crucial role in reinfection and establishing persistent SARS-CoV-2 infections. Evidence for persistent infection has been indicated by prolonged viral shedding in feces in several studies. Reactivation or reinfection of the SARS CoV-2 is a concern associated the long Covid. One likely explanation for reinfection is waning of neutralizing antibodies within 2–3 months following recovery from SARS-CoV-2 infection. Serial antibody estimation and evidence of active viral replication can indicate the reinfection. The reinfection may entail lingering Long Covid symptoms as well as the probability that some of the long Covid patients may also act as the carriers of the virus. In this respect, the notions of virus persistence, viral reservoirs, chronic viral shedding, and related aspects are important.
The occasional cases of reinfection occur but the possibility of a significant number of reinfections leads us to the possibility existence of SARS-CoV-2 viral reservoirs. In general, subset of persistent viruses can go latent, when the viruses disappear, leaving their genetic material to re- emerge later. Even after two months following the infection, SARS-CoV-2 mRNA, SPs and NSPs have been detected in the intestines of those infected. Further, four months after onset of COVID-19, immunofluorescence and PCR analysis of intestinal biopsies show persistence of viral RNA and protein [23]. The immune system is likely to react these remnant proteins. The concept of potential viral reservoirs is captivating, as several viral infections are known to lie in body reservoirs, such as Ebola and hepatitis B. Experimentally, when a mouse is infected with murine coronavirus which infects the liver and the CNS, viral RNA can persist in its central nervous system (CNS) without being infectious. Further, the RNA can remain for the mouse’s whole lifetime, and associated with demyelinating disease.
In the persistent infection, SARS-CoV-2 virus is dispersed into various organs, and it is common for these patients, to test negative for viral genes, then test positive again as they shed low amounts of viral RNA. Further, the tests for COVID-19 may detect a scrap of the viral genome, which may last as long as 15 weeks. The COVID-19 patients with mild or asymptomatic disease were more likely to be persistently PCR positive than participants with a more severe illness. However, higher total antibodies levels associated with persistent viral RNA shedding may not increase the transmission risk [37]. Further, fully recovered individuals with persistent viral RNA shedding are unlikely to be a significant source of SARS-CoV-2 transmission and seem to have a more durable immunity, strongly reducing the risk of re-infection.
The persistent virus infection implies persistent superantigen exposure, which in turn induces systemic inflammation leading to cardiovascular morbidity and development of diabetes, documented following COVID-19. In addition, diabetes and cardiovascular disease worsen the outcome in case of reinfection, predispose for residual inflammation and development of autoimmune reaction. The reinfection may be an interesting proposition; however, the difference in clinical profile between the initial manifestations of COVID-19 and the prolonged symptoms in Long Covid fails to support this hypothesis.
The Altered Microbiota in Gut and Other Organs
The human gut harbours a huge population of enteric microbiota, majorly dominated by Bacteroidetes and Firmicutes that produces several metabolites to maintain the gut homeostasis. The gut microbiota plays important roles such as vitamin synthesis, protection against pathogens, and development and maturation of host immune system. Diet, environmental factors, and genetics play an important role in shaping gut microbiota. Gut microbiota diversity is decreased in old age. Any deviation from normal gut microbial composition is defined as microbial dysbiosis and characterized by preponderance of pathobionts and decline in the populations of the key taxa like Bacteroidetes and Firmicutes. The gut microbiome has been shown to influence the immune system response to COVID-19 infection and potentially affect disease severity and outcome.
Although COVID-19 is primarily a respiratory illness, there is mounting evidence to suggest that the gut microbiome is involved in its clinical manifestations. The gut microbiome influences the immune system in general and may potentially affect COVID-19 severity, course, recovery, and outcome in form of Long Covid.
Besides the gut, other organs such as lungs also harbour Fusobacterium, Haemophilus, Prevotella, Streptococcus, and Veillonella as main genera, which are relatively small as compared to the enteric microbiota. The emergence and maintenance of lung microbiota is governed by the equilibrium between microbial migration from the upper respiratory tract and microbial removal by the host defense systems. Even in small concentrations, the airway microbiome is crucial to the host immunity. The gut–lung axis also involves the migration of immune cells from gut to respiratory tract through circulation. The gut may regulate the responses in lungs via host-acquired inflammatory mediators in the circulation. Further, the lungs and the gut are intricately linked and affect the homeostasis through existence of an immunological co-ordination between the gut and lungs.
It has been documented that gut microbiota composition is significantly altered in patients with COVID-19 compared with non-COVID-19 individuals irrespective of the medication received [38]. Several gut commensals with known immunomodulatory potential such as Faecalibacterium prausnitzii, Eubacterium rectale and bifidobacteria have been shown to be underrepresented and low in samples collected up to 30 days after recovery from acute COVID-19. Further, the altered composition was related with disease severity and elevated concentrations of inflammatory cytokines and serum markers such as C reactive protein, lactate dehydrogenase, and aspartate aminotransferase and gamma-glutamyl transferase. Further, in a subset of recovered patients with COVID-19 experiencing persistent symptoms, such as fatigue, dyspnoea, and joint pains, the gut microbiome was shown to be dysbiotic 80 days after initial onset of symptoms [38].
There has been shown association between gut microbiota composition, levels of cytokines and inflammatory markers in patients with COVID-19 suggesting that the gut microbiome is involved with the disease severity as well as outcome via modulating the immune responses. The gut microbial dysbiosis persists after the disease resolution, partly because of the medications given during the acute phase and could contribute to the persistent Long Covid symptoms.
Long Covid Pathogenesis-New Insights
Superantigens Hypothesis and Histological Correlates
There seems a possibility that the virus may be entering into blood vessels in its earliest phase when infecting the nasal and oral mucosa, and pharynx, and traversing to infect the olfactory bulb on the inferior surface of the brain supported and protected by the cribriform plate, leading to anosmia and dysgeusia. Another extrapulmonary manifestation in COVID-19 is the formation of antigen-antibody complexes by 2-3 weeks, which activate the humoral immunity. The antigen-antibody reactions may propagate to organ damage leading some patients continue to suffer from long Covid symptoms after clearing the infection. Simultaneously, viral super antigen may overstimulate immune responses, inducing negative feedback loops that hamper the immune function and allow the virus to persist and replicate. The SARS-CoV-2 super antigens are known to cause a strong immune response and cytokine storm, by a polyclonal T cell activation.
The orchestration of antigen-specific immune responses is important in understanding the concepts related to antigens and super antigens. In a normal physiological situation, the viral antigens are presented by Dendritic cells (DCs) to T lymphocytes leading to activation of T cells with an antigen-specific T-cell receptors (TCRs). The activation of specific T cells leads to clonal expansion for antigen- specific T-cell population resulting in effective clearance of the virus. In an aberrant pathophysiological situation, super antigens are presented by DCs to T lymphocytes and lead to activation of a large subgroup of T lymphocytes through their common receptors. The large groups of activated T cells have clonal expansion leading to immune overreaction [39]. In a favourable situation, the immune response is downregulated by negative feedback loops involving CD4+CD25+ Treg lymphocytes and IL-10. The protective down-regulation of superantigen responses occurs naturally and the superantigen-induced immune reactions are checked for generating immune hyper-response. The down regulation of the immune system by corticosteroid treatment may also lead to immune suppression through down-regulating of the superantigen response to reduce morbidity and mortality in severe COVID-19 [22]. The downregulation of superantigen response, naturally or as result of corticosteroid treatment is likely to result in a partially effective immunity allowing the virus to persist.
There may occur/develop various autoantibodies during the course of COVID-19. In single-center and retrospective study from Huanshi, China involving 8 severe and 13 critical cases of COVID-19, demonstrated anti‒52 kDa SSA/Ro antibody, anti‒60 kDa SSA/Ro antibody, (SSA = Sjögren’s- syndrome-related antigen A), and antinuclear antibody (ANA) in 20%, 25%, and 50% of patients, respectively [40]. The autoantibodies may aggravate the ongoing damage and fibrosis in lungs and lead to other long-term consequences occurring in Long Covid patients. The immune dysregulation may also be responsible for the prothrombotic state and its related conditions in COVID-19. In addition, endotheliitis and hypoxemic tissue injuries may play a part apart from antigen- antibody reactions and aberrant immune response. This is also endorsed by histopathological correlates of COVID-19 showing extensive alveolar damage, thrombosis of the lung micro- and macro-vasculature, pneumocytes and endothelial cells showing viral RNA, and presence of syncytial cells [41].
The Altered Microbiome and Immunologic Correlates
The gastrointestinal (GI) tract is the largest immunological organ in the body and gut microbiota influence immune responses. Further, the ACE2 receptors are widely expressed in the gut enterocytes and the amino acid transport function of ACE2 has been linked to gut microbial ecosystem. The SARS-CoV-2 infection is, thus, bound to affect the gut microbiome and enteric milieu, which in turn influences the severity of COVID-19 as well as the magnitude of the immune system response to the infection. The elderly, immune-compromised patients, and patients with other co- morbidities like type-2 diabetes, cardiovascular disorders have a general imbalance of gut microbiota (dysbiosis) and fare poorly in combating COVID-19 [42].
Various studies have noted persistent alterations in the fecal microbiome during the hospitalization and later, as compared with controls. Considering this, the alteration in the variety and volume of bacteria in the gut, leading to the microbial dysbiosis may also be implicated in persisting inflammatory symptoms following recovery from COVID-19, or Long Covid. Further, various studies have identified the viral RNA of SARS-CoV-2 in fecal specimens [43]. Further, the fecal microbiota alterations have been associated with fecal shedding of SARS-CoV-2 genome and COVID-19 severity. Another study noted that though about 12% of patients with COVID-19 will manifest GI symptoms, SAR-CoV-2 shedding was observed in 40.5% of patients [44]. Further, the viral genome has been identified from anal/rectal swabs of the COVID-19 patients even after the clearance of virus from the upper respiratory tract [45].
In an oft-quoted study, Yeoh YK, et al. [38] analysed the blood and stool samples and medical records from 100 hospital in-patients who had tested positive for COVID-19 and from 78 people without COVID-19, as controls. The serial faeces samples were collected up to 30 days after the virus was no longer detected in nasal and throat swabs. The gut microbiome, in respect of both the taxa and range of microorganisms, was found to be significantly altered compared with people who had not had COVID-19. The analysis suggested that Gut microbiome composition was significantly altered in patients with COVID-19 compared with non-COVID-19 individuals irrespective of whether patients had received medication. Several gut commensals with known immunomodulatory potential such as Faecalibacterium prausnitzii, Eubacterium rectale and bifidobacteria were reduced in COVID-19 patients and remained low up to 30 days after disease resolution. There appear to exist a direct bidirectional relationship between the COVID-19 virus and the gut and lung microbiomes [46].
The pattern also exhibited correlation with disease severity and elevated concentrations of inflammatory cytokines and other markers such as C reactive protein, lactate dehydrogenase, aspartate aminotransferase and gamma-glutamyl transferase. The association between gut microbiota composition, levels of cytokines and inflammatory markers in patients with COVID-19 suggest that the gut microbiome is involved in the magnitude of COVID-19 severity possibly via modulating host immune responses. In a subset of recovered patients with COVID-19 experience persistent symptoms, such as fatigue, dyspnoea, and joint pains, some over 80 days after initial onset of symptoms, the dysbiotic gut microbiome could contribute to immune-related Long Covid symptoms. It was inferred that the altered microbiome was associated with enhanced values for inflammatory markers in suggesting that the microbial dysbiosis may contribute to Long Covid symptoms.
In another study, Zuo T, et al. [47] found that patients with COVID-19 had significant alterations in fecal microbiomes compared with controls, characterized by enrichment of opportunistic pathogens and depletion of beneficial commensals, at time of hospitalization and later.
The depleted symbionts and gut dysbiosis persisted even after clearance of SARS-CoV-2 and resolution of respiratory symptoms. Further, the baseline abundance of Coprobacillus, Clostridium ramosum, and Clostridium hathewayi correlated with COVID-19 severity, and there was an inverse correlation between abundance of Faecalibacterium prausnitzii (an anti- inflammatory bacterium) and disease severity.
The gut microbiota derived signals are known to tune the immune cells for pro and anti-inflammatory responses thereby affecting the susceptibility to various diseases. In SARS-CoV-2 infection also, a healthy gut microbiome is pivotal in maintaining an optimal immune system to prevent an array of excessive immune reactions that eventually become detrimental to lungs and other vital organs. Like the gut microbiota, there is presence of distinct microorganisms in the lungs predominantly while Bacteroidetes, Firmicutes, and Proteobacteria. Interestingly, the gut microbiota has been shown to affect pulmonary health through the bidirectional gut-lung axis. Various respiratory viral infections including SARS-CoV-2 cause perturbations in the gut microbiota, and in turn the disease course is influenced by gut microbiome [48].
Conclusion: The Therapeutic Considerations
Right now, our understanding about both COVID-19 and Long Covid is expanding. The COVID Human Genetic Effort aims to find genetic variants that compromise people’s immune systems and make them more vulnerable to the virus [49]. The study plans to include those with long-term impairment, hoping to understand why their symptoms persist and to find ways to help them. The virus can also have the opposite effect, causing parts of the immune system to become hyperactive and trigger harmful inflammatory activity.
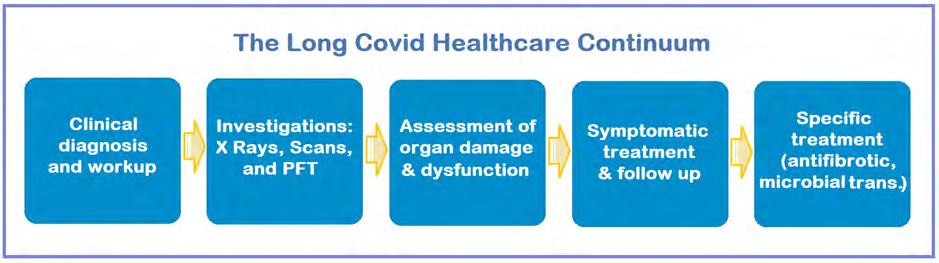
The issue of having a lingering form of the disease was started on social media like Facebook group for people with long COVID. Today, it has moved from being a curiosity, to a recognized public-health problem. In January 2021, the World Health Organization revised its guidelines for COVID-19 treatment to include a recommendation that all patients should have access to follow-up care in case of Long Covid [50]. On the practical therapeutic side, some countries are already opening clinics for people with Long Covid. There is a growing consensus that the long Covid clinics should be backed by multidisciplinary teams for supportive and specific treatment and follow up.
The trials suggest that anti-fibrotic and anti- inflammatory agents such as pirfenidone, deupirfenidone (the selectively deuterated form of pirfenidone), and Nintedanib may be helpful. Other drugs like, apixaban, an anticoagulant that might reduce the risk of dangerous blood clots; and atorvastatin, an anti-inflammatory may be helpful. Finally, the role of COVID-19 vaccines in preventing Long Covid is not known, although they may be helpful in preventing death and severe illness. Further, the impact of vaccines in people who are already having Long Covid is also not known. In a UK survey of more than 800 people with Long Covid, it was reported that 57% saw an overall improvement in their symptoms, 24% no change and 19% a deterioration after their first dose of vaccine [51].
The strategies to improve the intestinal dysbiotic microbiota may be helpful in reducing severity in COVID-19 and Long Covid. The prebiotics and probiotics may be helpful [52]. Further, the adjunctive therapies based on the modulation of the gut-lung axis and re-establishment of eubiosis could be an important therapeutic approach for constraining the harmful consequences of COVID-19 [53]. The microbiome transplants may hold promise for Long Covid and have been proposed as a potential treatment for individuals suffering long-term incapacitating symptoms [54].
In the United Kingdom, the Post-Hospitalisation COVID-19 Study (PHOSP-COVID) aims to follow 10,000 patients for a year, analysing clinical factors such as blood tests and scans, and collecting data on biomarkers [55]. It is a consortium of leading researchers and clinicians from across the UK to understand and improve long-term health outcomes for confirmed or suspected COVID-19 patients. Currently the information is limited concerning the long-term effects of COVID-19 and the ongoing medical, psychological and rehabilitation needs for these patients. The PHOSP-COVID team aims to develop trials of new strategies for clinical care to improve their long-term health. A similar study of such patients for has been launched in the United States.
There is evidence that SARS-CoV-2 virus may induce neurological impairments by invading the central nervous system leading to chronic myalgias and certain neurological deficits. The COVID-19 survivors from ICU care are likely to manifest various psychological, physical, and cognitive impairments. The Long Covid may results in a relevant morbidity for 3-6 months, and rehabilitation services and dedicated Long Covid healthcare might be needed for more than 12 months [56]. There are recommendations that the rehabilitation should commence in the critical care setting to prevent neuromuscular complications and improves functional status in later during Long Covid phase.
References
-
Carfì A, Bernabei R, Landi F (2020) Gemelli Against COVID-19 Post-Acute Care Study Group. Persistent Symptoms in Patients after Acute COVID-19. JAMA 324(6): 603-605.
-
Davis HA, Assaf GS, Akrami A (2020) Characterizing Long COVID in an International Cohort: 7 Months of Symptoms and Their Impact. Preprint at medRxiv.
-
Ziauddeen N, Gurdasani D, O Hara ME (2021) Characteristics of Long Covid: findings from a social media survey. Preprint at medRxiv.
-
Raveendran AV, Jayadevan R, Sashidharand S (2021) Long COVID: An overview. Diabetes Metab Syndr 15(3): 869-875.
-
UK Office for National Statistics (2021) Prevalence of ongoing symptoms following coronavirus (COVID-19) infection in the UK: 4 June 2021.
-
Yong SJ (2021) Long COVID or post-COVID-19 syndrome: putative pathophysiology, risk factors, and treatments, Infectious Diseases pp: 1-18.
-
Marx V (2021) Scientists set out to connect the dots on long COVID. Nat Methods 18: 449-453.
-
Evans RA, McAuley H, Harrison EM (2021) PHOSP-COVID Collaborative Group. Physical, cognitive and mental health impacts of COVID-19 following hospitalisation – a multi-centre prospective cohort study. Preprint at medRxiv.
-
Buonsenso D, Munblit D, De Rose C (2021) Preliminary evidence on long COVID in children. Acta Paediatr 110(7): 2208-2211.
-
Iqbal FM, Lam K, Sounderajah V (2021) Characteristics and predictors of acute and chronic post-COVID syndrome: A systematic review and meta-analysis. Eclinicalmedicine 36: 100899.
-
Weerahandi H, Hochman KA, Simon E (2020) Post- discharge health status and symptoms in patients with severe COVID-19. Preprint at medRxiv.
-
Zhang P, Li J, Liu H (2020) Long-term bone and lung consequences associated with hospital-acquired severe acute respiratory syndrome: a 15-year follow-up from a prospective cohort study. Bone Res 8: 8.
-
Salehi S, Abedi A, Balakrishnan S, Gholamrezanezhad A (2020) Coronavirus Disease 2019 (COVID-19): A Systematic Review of Imaging Findings in 919 Patients. AJR Am J Roentgenol 215(1): 87-93.
-
Salamanna F, Veronesi F, Lucia Martini L (2021) Post- COVID-19 Syndrome: The Persistent Symptoms at the Post-viral Stage of the Disease. A Systematic Review of the Current Data. Front Med 8: 653516.
-
National Institute for Health Research (2021) Living with COVID-19 A Dynamic Review of the Evidence around Ongoing COVID-19 Symptoms (Often Called Long COVID).
-
(2021) Living with Covid19 - A dynamic review of the evidence around ongoing Covid19 (often called Long Covid). Second review.
-
Varga Z, Flammer AJ, Steiger P (2020) Endothelial cell infection and endotheliitis in COVID-19. Lancet 395(10234): 1417-1418.
-
Xiong TY, Redwood S, Prendergast B, Chen M (2020) Coronaviruses and the cardiovascular system: acute and long-term implications. Eur Heart J 41(19): 1798-1800.
-
Ayoubkhani D, Khunti K, Nafilyan V, (2021) Epidemiology of post-COVID syndrome following hospitalisation with coronavirus: a retrospective cohort study. Preprint at medRxiv.
-
Salmon Ceron D, Slama D, De Broucker T (2020) APHP COVID-19 research collaboration. Clinical, virological and imaging profile in patients with prolonged forms of COVID-19: A cross-sectional study. J Infect 82(2): e1-e4.
-
Liotti M, Menchinelli G, Marchetti S (2020) Assessment of SARS-CoV-2 RNA Test Results Among Patients Recovered from COVID-19 With Prior Negative Results. JAMA Intern Med 181(5): 702-704.
-
Jacobs JJL (2021) Persistent SARS-2 infections contribute to long COVID-19. Med Hypotheses 149: 110538.
-
Gaebler C, Wang Z, Lorenzi JCC (2021) Evolution of antibody immunity to SARS-CoV-2. Nature 591(7851): 639-644.
-
Lindner D, Fitzek A, Bräuninger H (2020) Association of Cardiac Infection with SARS-CoV-2 in Confirmed COVID-19 Autopsy Cases. JAMA Cardio 5(11): 1281- 1285.
-
Maiese A, Manetti AC, La Russa R (2020) Autopsy findings in COVID-19-related deaths: a literature review. Forensic Sci Med Pathol pp: 1-18.
-
Dani M, Dirksen A, Taraborrelli P (2021) Autonomic dysfunction in ‘long COVID’: rationale, physiology and management strategies. Clin Med (Lond) 21(1): e63-e67.
-
Barker Davies RM, O’Sullivan O, Senaratne KPP (2020) The Stanford Hall consensus statement for post- COVID-19 rehabilitation. Br J Sports Med 54(16): 949- 959.
-
Raman B, Cassar MP, Tunnicliffe EM (2021) Medium-term effects of SARS-CoV-2 infection on multiple vital organs, exercise capacity, cognition, quality of life and mental health, post-hospital discharge. EClinicalMedicine 31: 100683.
-
Kommoss FK, Schwab C, Tavernar L (2020) The Pathology of Severe COVID-19-Related Lung Damage - Mechanistic and Therapeutic Implications. Dtsch Arztebl Int 117: 500-506.
-
Sun B, Tang N, Peluso MJ (2021) Characterization and Biomarker Analyses of Post-COVID-19 Complications and Neurological Manifestations. Cells 10(2): 386.
-
Hickie I, Davenport T, Wakefield D (2006) Post-infective and chronic fatigue syndromes precipitated by viral and non-viral pathogens: prospective cohort study. BMJ 333: 7568.
-
Komaroff AL, Bateman L (2021) Will COVID-19 Lead to Myalgic Encephalomyelitis/Chronic Fatigue Syndrome?. Front Med (Lausanne) 7: 606824.
-
Zhao YM, Shang YM, Song WB (2020) Follow-up study of the pulmonary function and related physiological characteristics of COVID-19 survivors three months after recovery. EClinicalMedicine 25: 100463.
-
Lam MH, Wing YK, Yu MW (2009) Mental morbidities and chronic fatigue in severe acute respiratory syndrome survivors: long-term follow-up. Arch Intern Med 169(22): 2142-2147.
-
Moldofsky H, Patcai J (2011) Chronic widespread musculoskeletal pain, fatigue, depression and disordered sleep in chronic post-SARS syndrome; a case-controlled study. BMC Neurol 11: 37.
-
Wong TL, Weitzer DJ (2021) Long COVID and Myalgic Encephalomyelitis /Chronic Fatigue Syndrome (ME/ CFS) - A Systemic Review and Comparison of Clinical Presentation and Symptomatology. Medicina (Kaunas) 57(5): 418.
-
Plebani M (2020) Persistent viral RNA shedding in COVID-19: Caution, not fear. Ebiom 64: 103234.
-
Yeoh YK, Zuo T, Lui GC (2021) Gut microbiota composition reflects disease severity and dysfunctional immune responses in patients with COVID-19. Gut 70: 698-706.
-
Porritt RA, Paschold L, Rivas MN (2020) Identification of a unique TCR repertoire, consistent with a superantigen selection process in Children with Multi-system Inflammatory Syndrome. Preprint bioRxiv.
-
Zhou Y, Han T, Chen J (2020) Clinical and Autoimmune Characteristics of Severe and Critical Cases of COVID-19. Clin Transl Sci 13(6): 1077-1086.
-
Bussani R (2020) Persistence of viral RNA, pneumocyte syncytia and thrombosis are hallmarks of advanced COVID-19 pathology. EBioMedicine 61: 103104.
-
Ahlawat S, Asha, Sharma KK (2020) Immunological co-ordination between gut and lungs in SARS-CoV-2 infection. Virus Res 286: 198103.
-
Wong MCS, Huang J, Lai C (2020) Detection of SARS- CoV-2 RNA in fecal specimens of patients with confirmed COVID-19: A meta-analysis. J Infect 81(2): e31-e38.
-
Parasa S, Desai M, Chandrasekar VT (2020) Prevalence of Gastrointestinal Symptoms and Fecal Viral Shedding in Patients with Coronavirus Disease 2019: A Systematic Review and Meta-analysis. JAMA Netw Open 3(6): e2011335.
-
Wang Y, Chen X, Wang F (2021) Value of anal swabs for SARS-COV-2 detection: a literature review. Int J Med Sci. 18(11): 2389-2393.
-
Burchill E, Lymberopoulos E, Menozzi E (2021) The Unique Impact of COVID-19 on Human Gut Microbiome Research. Front Med 8: 652464.
-
Zuo T, Zhang F, Lui GCY (2020) Alterations in Gut Microbiota of Patients With COVID-19 During Time of Hospitalization. Gastroenterology 159(3): 944-955.
-
Dhar D, Mohanty A (2020) Gut microbiota and Covid-19- possible link and implications. Virus Res 285: 198018.
-
Helen Su (2020) National Institute of Allergy and Infectious Diseases (NIAID)/National Institutes of Health (NIH), Bethesda, USA and Co-leader Dr Jean-Laurent Casanova, The Rockefeller University, Howard Hughes Medical Institute (HHMI), New York, USA and Necker Hospital for Sick Children & INSERM, Paris, France.
-
The World Health Organization (2021) Revised guidelines for COVID-19 treatment.
-
(2020) Long COVIDSOS vaccine report.
-
Nikhra V (2020) The Transzoonotic Virome interface: Measures to balance, control and treat epidemics. Ann Biomed Sci Eng 4: 020-027.
-
De Oliveira GLV, Oliveira CNS, Pinzan CF (2021) Microbiota Modulation of the Gut-Lung Axis in COVID-19. Front Immunol 12: 635471.
-
Nejadghaderi SA, Nazemalhosseini-Mojarad E, Asadzadeh Aghdaei H (2021) Fecal microbiota transplantation for COVID-19; a potential emerging treatment strategy. Med Hypotheses 147: 110476.
-
The Post-Hospitalisation COVID-19 Study (PHOSP- COVID), the United Kingdom.
-
Barker Davies RM, O’Sullivan O, Senaratne KPP (2020) The Stanford Hall consensus statement for post- COVID-19 rehabilitation. Br J Sports Med 54(16): 949- 959.
- Are the Vaccines the Only Solution to Prevent the COVID-19 Pandemic? Part Two
- Clinical Characteristics of Women in this New Global Immunodeficiency
- Cell Dynamics in HIV Pathogenesis: Insights and Implications
- Determination of the CDR (CDR1, CDR2) « Complementary- Determining Region Invertebrate Primitive Antibody from Sea Star »
- Prioritizing Care for High-Risk COVID-19 Patients in the EU: 10 Civic Recommendations to the Institutions
- Comprehensive Insights into ModRNA Vaccines: Persistent PP-Spike Recombinant Protein, Hyperimmune/Inflammatory Reactions, Thrombotic Vasculopathy, Chronic Organ Complications and Excess Deaths