Reveal the Myths about Role of Vitamin D Level on Some Hematological Parameters
Background: Vitamin D (Vit-D) may have effect on hematological parameters. Objective: To measure the effect of Vit-D on blood indices, our study was conducted to assess the relationship between Vit-D levels and hematological parameters. Subjects and Methods: The present study was cross section study conducted on 200 patients. Demographic data including age, sex, disease history and blood samples were withdrawn to measure serum vitamin D levels and hematological parameters. Data were reported as Mean ±SD and as frequency (percentage). ANOVA test was used to compare the mean serum levels of vitamin D in terms of sex, age or disease history. Results: Subjects enrolled into the study were 200 patients; 115(57.5%) females and 85(42.5%) males with mean age± SD of 37.6± 15.5 years. The mean serum vitamin D level in patients was 21.96 ± 14.31. There was non-significant relationship between hematological parameters and serum vitamin D level based on Pearson’s test. Conclusion: According to the findings of this study, it is interesting area of research that vitamin D was not the sole factor that have a role on hematological parameters as other factor may play a role as erythropoietin
Introduction
The complete blood count (CBC) tests and the analysis of blood smear images help to evaluate, diagnose, and monitor various health conditions, such as anemia, leukemia, infections, and allergic conditions. For blood disorders, such as anemia, which is based on HB level, the production and destruction of red blood cells are evaluated. In red blood cell disorder such as anemia, other red cell indices such as (mean cell volume) MCV, mean cell hemoglobin (MCH), mean corpuscular hemoglobin concentration (MCHC), RBC, and red blood cell distribution width (RDW or RCDW) are evaluated to narrow down on the causes of anemia. If the red cell indices are suggested of iron deficiency anemia (IDA), further tests to confirm the IDA will be done. In normal blood, red blood cell (RBC) counts range from 4.2 to 5.9 million cells per square centimeter. High RBC counts can be indicative of serious medical conditions, such as heart, lung, or kidney disease. Primary or secondary polycythemia in polycythemia HB is also raised; a bone marrow disorder also causes high RBC counts. Normal WBC counts range from 4,500 to 10,000 WBCs per microliter of blood. High WBC counts (above 30000 cells per microliter) indicate an infection, systemic illness, inflammation, allergy, leukemia, or burn induced tissue injury. If leukemia is suspected, analysis of blood smear is done to look for morphology of the leukemic cells and followed by bone marrow examinations. For platelets, which are small blood cell fragments that assist in blood clotting, normal counts range from 150,000 to 450,000 platelets per microliter. In patients with low platelet count such as in patients with dengue infection, their platelet count is monitored closely and the value is within critical level, the patient might need platelet transfusion. Generally, any abnormal blood smear reading indicates an infection or disease [1].
Anemia is a common nutritional problem in public health, and may further complicate chronic diseases including kidney and heart disease, resulting in fatigue, shortness of breath, and decreased physical capacity, and if severe enough, cardiovascular morbidity and mortality. Several factors may contribute to anemia including nutrient deficiencies, namely iron, but also folate, vitamins B12 and B6, as well as blood loss, infection, hemoglobinopathies, and inflammation. Given the multifactorial etiology of anemia, it can be classified into different subtypes such as iron deficiency anemia or anemia of nutrient deficiency, and anemia of inflammation (also called anemia of chronic disease). Vitamin D, through its down-regulatory effects on inflammatory cytokines and hepcidin may favorably impact anemia, particularly anemia of inflammation. This review will highlight recent advances in our understanding of the vitamin D-anemia association though mechanistic studies, epidemiologic studies, and early clinical trials [2].
Vitamin D is ‘‘a fat-soluble steroid hormone” ingested in the diet but the major produced occur through the skin after exposure to the solar ultraviolet rays in sunlight. Vitamin D is converted by the liver to inactive form ‘‘25(OH) Vitamin D, it has a half- life of 15 days” and is metabolized in kidneys to the active form “1,25-dihydroxyvitamin D” by the enzyme “25- hydroxyvitamin D-1α-hydroxylase (CYP27B1)” [3].
The normal range of Vitamin D assay has approximately 20-60ng/dL, this range may be too low for many serum patients, so when the concentration is less than 30ng/mmol leading to the case called ‘‘Vitamin D deficiency” and if it is less than 10ng/ml (12.5nmol/L) signifies severe deficiency [3].
Vitamin D plays a dual role in the human body as a prohormone nutrient and fat soluble vitamin. Due to its pleiotropic nature, beyond its influence on bone health, vitamin D demonstrates significant involvement in various gene expression processes and plays key roles in calcium and phosphate metabolism, which are involved in a multitude of physiological and pathophysiological mechanisms. Deficiency in vitamin D is linked to numerous illnesses and pathological conditions, including musculoskeletal health, immunity, cardiovascular disease, cancer and mental health, as well as deterioration of athletic performance. The high prevalence of low serum vitamin D concentration is a global problem in all age groups, even in regions of high sun exposure [4].
Vitamin D also regulates the process of erythropoiesis by stimulating erythroid progenitor cells in a synergistic fashion with other hormones and cytokines, including erythropoietin (EPO), and it has been reported that vitamin D is crucial for normal red blood cell production. The prevalence of anemia and the use of erythropoiesis-stimulating agents (ESA) have been found to be negatively correlated with serum VitD levels regardless of kidney function in the general population. The role of vitamin D in erythropoiesis has also been suggested by several clinical observations, especially in haemodialysis patients, where administration of VitD has been has been associated with dose reductions in erythropoiesis-stimulating agents (ESA) and increased reticulocytosis. Furthermore, vitamin D3 (calcitriol), in synergism with erythropoietin (EPO), increases the production of erythropoietin (EPO) receptor at the mRNA and protein levels in vitro [5].
Vitamin D also plays an integral role in the inflammatory response by down regulating pro-inflammatory cytokines. Moreover, recent studies investigating the clinical outcomes related to low vitamin D status have found that suboptimal 25-hydroxyvitamin D (25OHD) levels are independently associated with morbidity and all-cause mortality in non- institutionalized populations. Although low vitamin D status and elevated RDW are both independently associated with increased systemic inflammation and undesirable clinical outcomes, the relationship between these two biomarkers is not known. Therefore, in this hypothesis generating work, our goal was to investigate the association between serum 25OHD levels and RDW in a large [6].
Erythrocyte sedimentation rate (ESR) is one of the most widely performed laboratory assays in human medicine because it highlights the occurrence and the extent of inflammation. It is based on the principle that the sedimentation of red blood cells in autologous plasma is faster in patients with an increased plasma concentration of certain proteins, generally associated with acute tissue damage, chronic inflammation or infection, malignancy, and pregnancy. In fact, the rates of aggregation and sedimentation are manifestations of the blood suspension instability, based on a reciprocal effect between the erythrocyte membrane surface and plasma proteins called “agglomerans” such as fibrinogen, immunoglobulin M (IgM), and alpha-2- macroglobulin. Other factors influencing the ESR are primarily linked to the hematocrit (Hct) value and, in general, to blood interferents such as lipemia and hemolysis. In human medicine, the ESR is commonly used as a generic sickness index in conjunction with the patient’s clinical history, physical examination findings, and clinicopathological results. In addition, its clinical utility has been demonstrated in human medicine in primary care assistance, geriatric patients, hospitalized patients, hematological malignancies, stroke, heart disease, as well as in several inflammatory conditions of the osteomuscular system, and also cancer [7].
Objective
To clarify the effects of vitamin D level on hematological indices such as (hemoglobin, hematocrit, MCV, MCH, MCHC, RWD) and also on white blood cells and platelets and erythrocytes sedimentation rate.
Subjects and Methods
Subjects
Cross section study was conducted on 200 patients who underwent a comprehensive blood test. 85(42.5%) males and 115(57.5%) females their mean age was 37.6±15.5 years. The blood samples were collected at Aljawdah Medical Laboratory Company, Taif, KSA from January 2020 to May 2020, the following were excluded from the study.
- Patients with hematological diseases
- Patients with liver or kidney diseases
- Patients receive vitamin D supplement with the last three months
Methods
All Serum samples were tested for Vitamin D level using The ARCHITECT plus (Abbott Laboratories, USA).
Results
The ARCHITECT 25-OH Vitamin D assay is a quantitative delayed one-step competitive immunoassay to determine the level of vitamin D in human serum and plasma using CMIA technology with flexible assay protocols, referred to as Chemifiex.
- Sample, assay diluent and paramagnetic anti-vitamin D coated microparticles are combined. 25-OH vitamin D present in the sample is displaced from the vitamin D binding protein and binds to anti-vitamin D coated microparticles, forming an antigen- antibody complex.
- After incubation, a conjugate containing acridinium- labeled vitamin D is added to the reaction mixture and binds to unoccupied binding sites of the anti-vitamin D coated microparticles.
- After further incubation and washing, Pre-Trigger and Trigger Solutions are added to the reaction mixture.
- The resulting chemiluminesoent reaction is measured as relative light units (RLUs). There is a relationship between the amount of 25-OH vitamin D in the sample and the RLUs detected by the ARCHITECT iSystem optics. Results are calculated automatically based on the previously established calibration curve.
And all the CBC and ESR samples were tested by using Sysmex Automated Hematology Analyzer for CBC and Manually for Erythrocyte sedimentation rate (ESR).
Statistical Analysis
Collected data were coded, tabulated and introduced to a Personal Computer (PC) using the Statistical Package for Social Science (SPSS) for windows version 25.
Ethical Concerns
Ethical approval for this study was obtained from the Ethics Review Committee of the College of Applied Medical Sciences at Taif University, Taif, KSA (Tables 1 & 2; Figures 1-4).
| N | Minimum | Maximum | Mean | Std. Deviation | Skewness | Kurtosis | |||
|---|---|---|---|---|---|---|---|---|---|
| Statistic | Statistic | Statistic | Statistic | Statistic | Statistic | Std. Error | Statistic | Std. Error | |
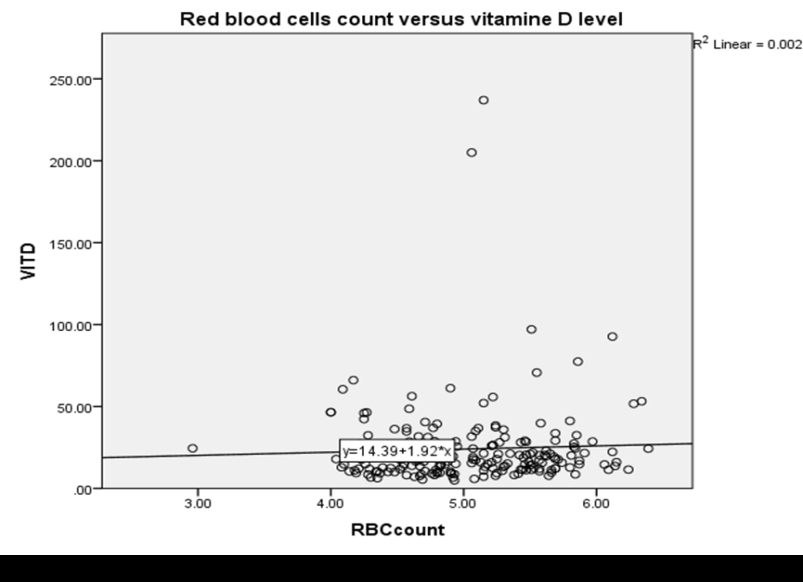
| RBCcount | 200 | 2.96 | 6.39 | 5.0456 | 0.58569 | -.048- | 0.172 | -.244- | 0.342 |
| Hb | 200 | 7.8 | 31.3 | 14.264 | 2.42099 | 1.405 | 0.172 | 11.522 | 0.342 |
| Hct | 200 | 25.6 | 74.5 | 42.197 | 5.64189 | 0.673 | 0.172 | 4.546 | 0.342 |
| MCH | 200 | 16 | 86.6 | 28.4885 | 5.0832 | 7.185 | 0.172 | 86.22 | 0.342 |
| MCHC | 200 | 27.7 | 43 | 33.565 | 1.67289 | -.088- | 0.172 | 6.131 | 0.342 |
| MCV | 200 | 57.3 | 94 | 83.779 | 6.41651 | -1.474- | 0.172 | 2.707 | 0.342 |
| RWD | 200 | 11.5 | 26.4 | 13.6225 | 1.7227 | 3.065 | 0.172 | 16.216 | 0.342 |
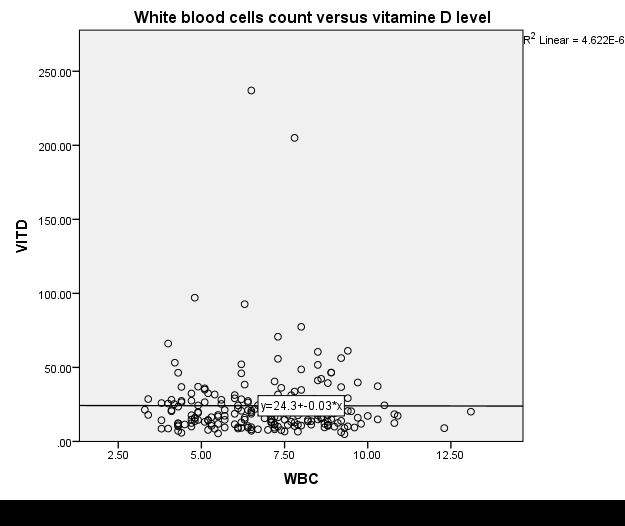
| WBC | 200 | 3.3 | 13.1 | 6.9259 | 1.91833 | 0.23 | 0.172 | -.450- | 0.342 |
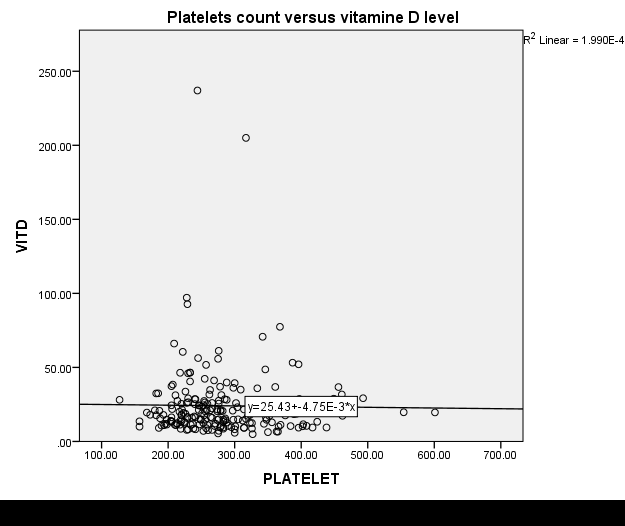
| Platelets | 200 | 127 | 601 | 278.52 | 74.22673 | 1.211 | 0.172 | 2.141 | 0.342 |
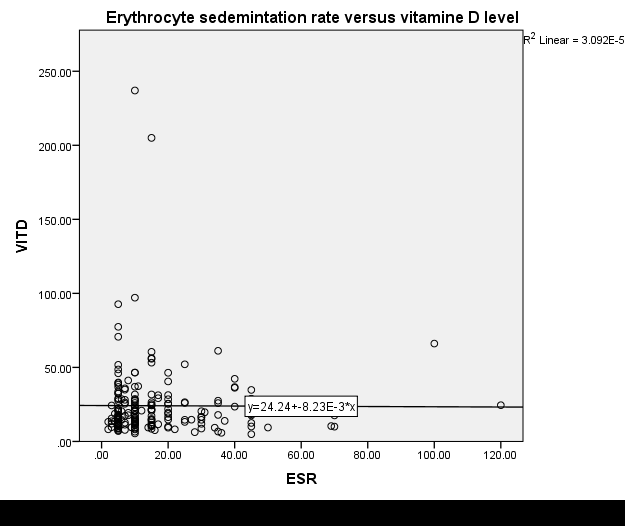
| ESR | 200 | 2 | 120 | 16.695 | 16.87769 | 2.644 | 0.172 | 9.851 | 0.342 |
| Vitamin D | 200 | 4.9 | 237 | 24.1045 | 24.98376 | 5.444 | 0.172 | 39.547 | 0.342 |
Table 1: Shows descriptive Statistics of hematological parameters and vitamin D in the study group.
| Hematological parameter versus Vitamin D | Pearson's correlation |
| RBCcount | 0.045 |
| Hb | -0.014 |
| Hct | 0.009 |
| MCH | -0.055 |
| MCHC | -0.024 |
| MCV | -0.045 |
| RWD | 0.073 |
| WBC | -0.002 |
| Platelets | -0.014 |
| ESR | -0.006 |
Table 2: Shows Pearson’s correlation between hematological parameters and vitamin D in the study group.
Discussion
Vitamin D (Vit-D) has been shown to play important roles in the regulation of several systems beside its role in bone and mineral metabolism. Vitamin D regulates the process of erythropoiesis by stimulating erythroid progenitor cells in a synergistic fashion with other hormones and cytokines, including EPO, and it has been reported that vitamin D is crucial for normal red blood cell production [8].
The lack of association between vitamin D status and the two main hematology parameters used to diagnose anemia— Hb and HCT—and the higher mean values of RBC, in the group with reduced vitamin D concentrations in our study, vitamin D deficiency might be particularly associated with inflammatory anemia, although it is worth emphasizing that a positive association between vitamin D and morphological parameters was also observed in healthy adults the impact of vitamin D on iron status is less proven, especially in terms of its effect on non-hematological parameters. Despite the association between vitamin D and blood morphology indices having been investigated relatively often, the results are contradictory, mainly due to the study of different subtypes of anemia [9].
Vitamin D is known to directly modify cytokine responses by upregulating anti-inflammatory cytokines, such as IL-10, and by inhibiting the proliferation of IL-2, tumor necrosis factor (TNF)-α, and the production of interferons. Increased levels of pro-inflammatory cytokines secondary to low vitamin D status has also been shown to interfere with normal erythropoiesis and to induce erythropoietin insensitivity in the bone marrow [10].
The findings of the present study revealed that a high prevalence of VDD in hilly area at an altitude of more than 2000 meters was similar to plain areas. Although the hilly areas at high altitude have adequate sunshine with low air pollution compared to plain area. Promotion of an active outdoor lifestyle and activities among children in both homes and schools may counteract the VDD [11].
In study of Otero T, et al. [6] shows the analysis of data from a large community-based sample of adults in the United States suggests that low 25OHD levels are associated with elevated RDW. And they hypothesize that low vitamin D status may contribute to increased erythrocyte size heterogeneity through increased systemic inflammation. While in our study shows no evidence between vitamin D deficiency and hematological parameters among group of patients. The difference between our study and Otero T, et al. [6] 10 study may be due to the high altitude zone and the hypoxia-inducible factor (HIF-1) is a responsible of oxygen homeostasis within cells. And therefore regulator the erythropoietin.
Conclusion
The current results clearly indicate no association between vitamin D and haematological parameters among group of patients, due to the observational study design, it is difficult to assess exactly which of the other factors which have a role on further rigorous, randomized controlled trials examining the other factors is recommended.
References
-
Alomari Y, Abdullah S, Zaharatul Azma SR, Omar K (2014) Automatic Detection and Quantification of WBCs and RBCs Using Iterative Structured Circle Detection Algorithm. Computational and Mathematical Methods in Medicine pp: 1-17.
-
Smith E, Tangpricha V (2015) Vitamin D and anemia. Current Opinion in Endocrinology, Diabetes and Obesity 22(6): 432-438.
-
Beshboosh N, Abd Alaali Z, Mohammed M (2018) Relationship between vitamin d deficiency and physiological blood parameters in hypothyroidism patients. Biochemical and Cellular Archives 18(1): 465- 470.
-
Malczewska Lenczowska J, Sitkowski D, Surała O, Orysiak J, Szczepańska B, et al. (2018) The Association between Iron and Vitamin D Status in Female Elite Athletes. Nutrients 10(2): 167.
-
Refaat B, Ashour T, El Shemi A (2014) Ribavirin induced anaemia: the effect of vitamin D supplementation on erythropoietin and erythrocyte indices in normal Wistar rat. Int J Clin Exp Med 7(9): 2667-2676.
-
Otero T, Monlezun D, Christopher K, Camargo C, Quraishi S (2017) Vitamin D status and elevated red cell distribution width in community-dwelling adults: Results from the National Health and Nutrition Examination Survey 2001–2006. The journal of nutrition health & aging 21(10): 176-1182.
-
Militello C, Pasquini A, Medina Valentin A, Simčič P, De Feo G, et al. (2020) The Canine Erythrocyte Sedimentation Rate (ESR): Evaluation of a Point-of-Care Testing Device (MINIPET DIESSE). Veterinary Medicine International pp: 1-6.
-
Refaat B, Ashour T, El-Shemi A (2014) Ribavirin induced anaemia: the effect of vitamin D supplementation on erythropoietin and erythrocyte indices in normal Wistar rat. Int J Clin Exp Med 7(9): 2667-2676.
-
Malczewska Lenczowska J, Sitkowski D, Surała O, Orysiak J, Szczepańska B, et al. (2018) The Association between Iron and Vitamin D Status in Female Elite Athletes. Nutrients 10(2): 167.
-
Otero T, Monlezun D, Christopher K, Camargo C, Quraishi S (2017) Vitamin D status and elevated red cell distribution width in community-dwelling adults: Results from the National Health and Nutrition Examination Survey 2001–2006. The journal of nutrition, health & aging 21(10): 1176-1182.
-
Kapil U, Ravindra Mohan Pandey RM, Goswami R, Sharma B, Sharma N, et al. (2017) Prevalence of Vitamin D deficiency and associated risk factors among children residing at high altitude in Shimla district, Himachal Pradesh, India. Indian Journal of Endocrinology and Metabolism 21(1): 178-183.
- Are the Vaccines the Only Solution to Prevent the COVID-19 Pandemic? Part Two
- Clinical Characteristics of Women in this New Global Immunodeficiency
- Cell Dynamics in HIV Pathogenesis: Insights and Implications
- Determination of the CDR (CDR1, CDR2) « Complementary- Determining Region Invertebrate Primitive Antibody from Sea Star »
- Prioritizing Care for High-Risk COVID-19 Patients in the EU: 10 Civic Recommendations to the Institutions
- Comprehensive Insights into ModRNA Vaccines: Persistent PP-Spike Recombinant Protein, Hyperimmune/Inflammatory Reactions, Thrombotic Vasculopathy, Chronic Organ Complications and Excess Deaths