Detection of Syphilis among HIV-Positive and HIV-Negative Patients in Ogun State, Nigeria
Background: Syphilis is still one of the major causes of death in some developing countries where HIV infection is also prevalent. The aim of this study was to determine the prevalence of syphilis among HIV positive and negative women in Ogun state. Methods: The serum samples of 240 (120 HIV Positive and 120 HIV Negative) consenting female participants were collected randomly and screened using two brands of Syphilis Immunochromatographic rapid diagnostic test (RDT) kits: LabAcon (Biotest Biotech Co., Ltd., Hangzhou, China) and Perfect (Abbon Health care, Ltd, UK). The demographic and clinical information of the participants were collected using a structured questionnaire. Statistical analysis was carried out using SPSS Statistics software package (version 18.0). One-way analysis of variance (ANOVA) and Tukey-Kramer Multiple Comparisons Test was used to test for significant differences in the prevalence of syphilis among the study population. P values <0.05 was considered significant. Results: The outcome of the study shows that Syphilis exist among both HIV-positive and HIV-negative women in Ogun State with a prevalence rate of 11.7% and 4.2%, respectively using LabAcon RDT kit and also 9.2% and 2.5%, respectively, using Perfect RDT kit. The occurrence of syphilis was significantly (P<0.05) higher among HIV-positive subjects compared to their HIV-negative counterparts. All the participants who tested positive to syphilis were symptomatic regardless of their HIV status. Significant risk factors of syphilis associated with HIV infected subjects include past history of sexually transmitted infection and engagement in unprotected sex (p<0.05). Conclusion: Syphilis exists among both HIV-positive and HIV-negative women in Ogun State and therefore the need for routine screening for syphilis among women, especially those infected with HIV cannot be over-emphasized.
Introduction
Syphilis is a chronic, sexually transmitted infection affecting an estimated 36 million people worldwide, with 11 million new cases occurring annually [1, 2]. In recent years, rates of primary and secondary syphilis have risen sharply in particular populations, most prominently amongst men who have sex with men, while a general increase in infectious syphilis cases in both heterosexual men and women has been observed in cities across North America, Europe, and Asia [3, 4]. This sexually transmitted infection is caused by a spirochaete, called Treponema palladium. The organism belongs to the family Spirochaetaceae, order Spirochaetales, phylum Spirochaetes, which is a phylogenetically ancient and distinct group of bacteria. Due to the cell structure, physiology, genetics, and pathogenic features T. pallidum is a very unusual microorganism [5]. Pathogenic treponemes cause venereal syphilis, yaws, endemic syphilis, and pinta—multi-stage, infections that, although similar, can be differentiated based on clinical, epidemiologic, and geographic criteria [6, 7]. Only venereal syphilis is transmitted by sexual activity. The pathogenic treponemes are uncultivatable, slow-growing microorganisms with identical flat-wave morphologies. They poorly tolerate desiccation, elevated temperature, and ambient oxygen tension, traits that explain why efficient transmission requires close personal contact. T. pallidum is considered the most virulent subspecies because it routinely traverses blood-brain and maternal-fetal placental barriers [8].
Treponema pallidum causes a chancre at the inoculation site (primary syphilis). A maculopular rash and lymphadenopathy are prominent in the second stage of syphilis. Fever, malaise, nausea, headache, joint pain, and anorexia may also be present. Next, a latent stage occurs in which the organism invades vital organs. A final, tertiary stage may display gummas, cardiovascular disease, and neurosyphilis. Sexual transmission occurs when the spirochetes gain access through a break in a mucosal surface through genital-genital or oral-genital contact with an infected partner. The spirochete replicates locally in the primary stage (chancre) and then disseminates causing secondary infection. Transmission may also occur transplacentally or at the time of delivery to infect a fetus/ neonate, causing congenital or neonatal syphilis infection [9].
Treponema pallidum and Human immunodeficiency virus (HIV) can co-infect the same host, because their risk factors are the same and they are both transmitted sexually [10]. By the end 2007, 33 million people were infected by HIV and meanwhile, syphilis is still one of the major causes of death in some developing countries where HIV infection is also prevalent [11].
Syphilis ulcers can facilitate the transmission of HIV, decrease CD4 levels and increase viral load among HIV infected patients. On the other hand, HIV infection increases the risk of neurosyphilis [12]. It may alter syphilis’s clinical features and its treatment outcomes and it might be related with syphilis treatment failure, especially if neurosyphilis had a delayed diagnosis [13]. In addition, syphilis can mimic various clinical expressions and cause severe cardiovascular and neurological problems among the HIV infected patients [14].
Symptomatic syphilis infections increase human immunodeficiency virus (HIV) transmission and acquisition two to five fold, and modelling studies predict that eradication of syphilis would have a significant impact on HIV prevention [15, 16]. The increasing prevalence of infectious and congenital syphilis, despite the continued sensitivity of T. pallidum to treatment with penicillin, underscores the need for syphilis vaccine development as a complement to traditional screening and treatment approaches for the global elimination of syphilis. In addition, although T. pallidum has not yet exhibited resistance to penicillin, resistance to second-line therapy such as macrolide-based antibiotics has emerged [17]. As a result, and because of the devastating consequences of congenital syphilis, penicillin- allergic pregnant women require desensitization and treatment with penicillin, further emphasizing the need for an alternative control measure. Syphilis can reach a latent stage where there are no symptoms and then escalate into a tertiary stage with many problems such as neurological problems, sore and inflamed gummas and heart problems.
Treponema pallidium infection has been identified as an important risk factor for the development of syphilis disease among HIV patients because they are immunosuppressed individuals. Considering the increasing prevalence of HIV and also extensive use of highly active antiretroviral therapy in developing nations, the diagnosis of syphilis among such patients should be timely established using screening tests that are both sensitive and specific. However, this is not the case with the many commercially sold rapid diagnostic test kits in the markets.
Syphilis is common among Nigerian populace. To the best of our knowledge, no work has been done to assess the prevalence of Syphilis among HIV and Non-HIV infected female individuals in Ogun state. Besides, there is need to identify factors that predispose female individuals in this setting to Syphilis. Scarcity of information in this regard, therefore necessitates this study. The aim of this study is therefore to determine the prevalence of syphilis and associated risk factors among HIV and non-HIV infected women in Ogun state using two rapid diagnostic kits.
Materials and Methods
Study Design
This was a cross sectional descriptive study.
Study Area
This study was carried out among women receiving healthcare at Babcock University Teaching Hospital (BUTH), Ilishan-Remo, Ogun State, as well as General Hospital, Ijebu-Ode, Ogun State. BUTH is a 300 bed space capacity private hospital and the only tertiary hospital in the community. While Ilishan-Remo community is one of the geo-political wards in Ikenne Local Government Area of Ogun State, situated in the tropical area of south-western part of Nigeria, coordinates $7^\circ 29'00''\text{N}, 2^\circ 55'00''\text{E}$. On the other hand, General Hospital, Ijebu-Ode, Ogun is a 1000 bed space capacity Government owned hospital and the only tertiary hospital in the Itoro Local Government Area (LGA), also situated in the tropical area of south-western part of Nigeria, coordinates $6.8131^\circ\text{N}, 3.9249^\circ\text{E}$.
Study Duration
The study was carried out within the period of 2 months (September- November, 2020).
Study Population
This cross sectional institutional based study was carried out among HIV and Non-HIV infected female individuals in Ogun state.
Sample Size Calculation
The sample size for this study was calculated using the formula described by Pourhoseingholi, et al. [18]:
$$N = \frac{Z^2 \times P(1-P)}{D^2}$$
Where:
N= minimum sample size required
Z= confidence interval (1.96)
P= prevalence rate of HIV syphilis co-infection in a tested population
D= desired level of significance (0.05)
For the calculation, a 95% confidence interval, a P value of 0.019, i.e., a prevalence rate of 7.3% for HIV-syphilis co-infection among female patients from a previous study by Shimelis, et al. [19] and margin of error (d) set at 0.05 was used to determine the minimum sample size required. To minimize errors arising from the likelihood of non-compliance, 10% of the sample size was added.
$$N = \frac{Z^2 \times P(1-P)}{D^2}$$
Z = 1.96
P = 7.3% as reported by Shimelis, et al. [19]
d = 0.05
$$N = \frac{1.96^2 \times 0.073(1-0.073)}{(0.05)^2}$$
$$N = \frac{3.8416 \times 0.073 \times 0.927}{0.0025}$$
$$N = 0.2599$$
$$0.0025$$
$$N = 104$$
10% of 104: $10/100 \times 104 = 10.4 = 10$
Sample size is therefore $104 + 10 = 114$
The sample size calculated at a prevalence of 7.3% as reported by Shimelis, et al. [19] is 114. However, for uniformity and accuracy, the number shall be scaled up to 120. Since the study is designed to screen for syphilis among two type of study participants: HIV infected (Test) and Non-HIV infected (control) groups. The calculated sample size was multiplied by two (2) to give a total sample size of 240.
Sample Size
A total of 240 blood specimens were collected from consenting 120 HIV infected and 120 non-HIV infected women recruited from Babcock University Teaching Hospital
(BUTH), Ilishan-Remo, Ogun State, as well as General Hospital, Ijebu-Ode, Ogun State.
Ethical Consideration
Ethical clearance was obtained from the Babcock University Health Research Ethics Committee (BUHREC) before the commencement of the study; while administrative clearance was obtained from the administration of Babcock University Teaching Hospital, Ilishan- Remo, Ogun State, as well as Ogun State Hospital Management Board.
Eligibility of Subjects
Inclusion Criteria: Consenting HIV positive and HIV negative women attending Babcock University Teaching Hospital (BUTH), Ilishan- Remo, Ogun State and General Hospital, Ijebu-Ode, Ogun State, who are eighteen years or more (≥18 years) and not on any antibiotic therapy in the preceding two (2) weeks were randomly selected for the study.
Exclusion Criteria: Consenting HIV positive and HIV negative women attending Babcock University Teaching Hospital (BUTH), Ilishan- Remo, Ogun State and General Hospital, Ijebu-Ode, Ogun State, who are less than (<) 18 years and on any antibiotic therapy in the preceding two (2) weeks were excluded from the study.
Consent
Informed consent was obtained from each participant. The purpose and nature of the study, as well as the method of sample collection was explained to them properly, afterwards, participants were required to voluntarily complete the consent form in their own hand writing and endorsed by their signatures as proof of willingness to provide samples for the test. They were assured of the confidentiality.
Sample Collection
Two (2) ml of venous blood samples was collected into plain bottles and allowed to clot to get the sera from the patients. Following blood clotting, the serum was separated by aspiration using Pasteur pipette.
Sample Transportation
The blood samples were transported to the laboratory unit of the department of medical laboratory science, Babcock University and processed within 2 hours of collection. All samples were transported to the laboratory as soon as possible without delay and was processed on the same day of collection. The specimens were collected from each participant and labelled accordingly with their identification number on the specimen container.
Specimen Storage
Specimen was stored because they needed to be processed as soon as possible. But where delay is envisaged, the sera was stored at 2-80C for up to 3 days. For long term storage, specimens were kept below -200C. Frozen specimens was completely thawed and mixed well prior to testing. Repeated cycle of freezing and thawing of sera was avoided.
Laboratory Analyses
HIV Detection
HIV detection was carried out using the current National algorithm for HIV sero-diagnosis. This will involve the use of 3 rapid diagnostic kits, following their manufacturer’s instructions. Briefly, each patient’s serum will be screened for the presence of HIV antibodies using Determine (Abbott Laboratories, Tokyo, Japan) and Unigold HIV (Trinity Biotech Plc Bray, Co. Wicklow, Ireland). When both kits show positivity, the patient was regarded as positive for HIV infection and vice versa. However, when test results is discordant, a third kit, which is the Tie breaker, 1/2 Stat Pak (Chembio Diagnostic Systems, New York, USA) was used. The HIV serostatus of the patient was taken as the result of either of the first two kits that agree with that of the third kit [20, 21].
Detection of Treponema Pallidium Using Rapid Diagnostic Method
Treponema pallidium antibody in participant’s sera (if present) was detected using two types of syphilis rapid diagnostic kits: Syphilis labAcon test kit supplied by Biotest Biotech Co., Ltd., Hangzhou, China, as well as Perfect Syphilis test kit supplied by ABBON Health care, Ltd, UK.
Procedure
• Specimens and reagents were brought to room temperature (15-30oC) prior to testing.
• The sealed pouch was opened by tearing along the notch when ready to begin test.
• Participant’s serum sample (60µl-80µl, about 2-3 drops) was added into the sample well on the cassette using a pipette.
• The results were read after 10-15 minutes by observing the pink color move across the Result Window in the center of the test disk.
• Result after 30 minutes was not read.
Interpretation of Results
Positive Result
The presence of two color bands (“T” band and “C” band) within the result window regardless of which band appears first indicates a positive result.
Negative Result
The presence of only one pink colour band within the result window indicates a negative result.
Invalid Result
A total absence of colour in either regions or only one color band appearing on the test region indicates procedure error and/or the test reagent has deteriorated.
Statistical Analysis
Raw data was entered into Microsoft Excel. Statistical analysis was carried out using SPSS Statistics software package (version 18.0). One-way analysis of variance (ANOVA) and Tukey-Kramer Multiple Comparisons Test was used to test for significant differences in the prevalence of Treponema pallidium infection among the women using two types of rapid diagnostic test kits. P values <0.05 was considered significant. The confidence intervals for sensitivity and specificity was computed using the Wilson’s score method. A P value ≤0.05 was considered statistically significant. Statistical analysis outputs were represented using tables and charts.
Results
A total of 240 subjects were enrolled and tested in this study comprising of 120 subjects diagnosed with HIV and 120 HIV negative. Syphilis test was carried on all study subjects using two different kit (LabAcon Kit and Perfect Kit). Table 1 below shows the socio-demographic distribution of study subjects. In respect to age, majority (54.2%) of HIV negative subjects were aged 18-25 years, followed by 26- 33 years (21.7%), 12% were 34-41 years, 7.5% were 42-49 and 4.2% above 50 years. The same table also shows that majority (26.7%) of the HIV positive subjects, were aged between 18-25 and 34-41 years and followed by 26-33 years (24.2%), 20% were 42-49 years and 2.5% above 50 years. In respect to marital status, majority (55.8%) of HIV negative subjects were single, followed by married (38.3%), 1.7% were separated and widow respectively, and 2.5% were divorced. The same table also shows that majority (41.7%) of the HIV positive subjects, were married, followed by singles (40.8%), 14.2% were divorced, 2.5% were widowed and 0.8% separated. As regards religion, majority (74.2%) of HIV negative subject were Christians, followed by Muslim (18.3%), and 7.5% practiced other religion. The same table also shows of majority (49.2%) HIV positive subject, were Christian, 36.7% were Muslims, 7.5% were Traditionalist and 6.7% practiced other religion. On the basis of the educational level of the study participants, majority of them have tertiary education (65.8%), while a small proportion of them have no formal education (5.8%).
The occurrence of syphilis infection in relation to the HIV status of the study participants is presented in Table 2. Five (4.2%) of the HIV negative subjects tested positive by LabAcon RDT Kit, while 3 (2.5%) tested positive by Perfect RDT kit. The occurrence of syphilis infection among HIV positive subjects using LabAcon test Kit was 11.7%, while that of Perfect Test Kit was 9.2%. The occurrence of syphilis infection among HIV positive subjects was significantly higher when compared to their HIV negative counterparts using both test kit (LabAcon test Kit, χ2= 4.806, p-value = 0.028; Perfect test Kit, χ2=5.143, 0.023).
The distribution of symptomatic and asymptomatic syphilis among the study participants is presented in Table 3. All the subjects examined who tested positive to syphilis using both LabAcon and Perfect RDT kits were symptomatic for syphilis regardless of their HIV status.
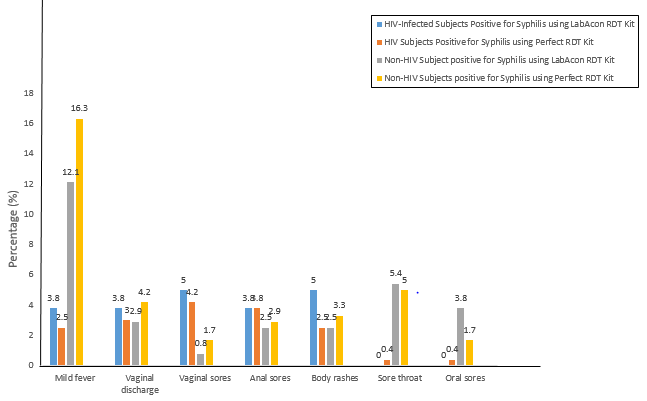
Indications for syphilis among HIV and Non-HIV Study Participants are presented using a histogram (Figures 1 & 2). Majority who indicated mild fever (16.3%) and vaginal discharge (4.2%) were HIV negative subjects and tested positive for syphilis by Perfect RDT Kit. Meanwhile, majority who indicated vaginal sores (4.2%) were HIV positive subjects and tested positive for syphilis using the Perfect RDT Kit. Still, majority who indicated anal sores (3.8%) and body rashes (5.0%) were HIV positive subjects and tested positive for syphilis using LabAcon RDT Kit. Meanwhile, majority who indicated sore throat (5.4%) and oral sores (3.8%) were HIV negative subjects and tested positive for syphilis using the LabAcon RDT Kit.
Risk factors associated with Syphilis infection among the study participants is presented in Tables 1-4. History of sexually transmitted infection and engagement in unprotected sex are significant risk factors associated with the occurrence of syphilis infection among HIV positive subjects; while factors such as sharing underwear with others, history of sexually transmitted infection, number of sexual partners, and recent change of sex partner were significant risk factors associated with syphilis infection among HIV Negative subjects (p<0.05).

| Category | No. of HIV Negative Subjects examined N (%) | HIV Positive Subjects examined | |
|---|---|---|---|
| Age Range | 18-25 | 65 (54.2) | 32 (26.7) |
| Age Range | 26-33 | 26 (21.7) | 29 (24.2) |
| Age Range | 34-41 | 15 (12) | 32 (26.7) |
| Age Range | 42-49 | 9 (7.5) | 24 (20.0) |
| Age Range | >50 | 5 (4.2) | 3 (2.5) |
| Age Range | Total | 120 (100) | 120 (100) |
| Marital Status | Divorced | 3 (2.5) | 17 (14.2) |
| Marital Status | Married | 46 (38.3) | 50 (41.7) |
| Marital Status | Separated | 2 (1.7) | 1 (0.8) |
| Marital Status | Single | 67 (55.8) | 49 (40.8) |
| Marital Status | Widow | 2 (1.7) | 3 (2.5) |
| Marital Status | Total | 120 (100) | 120 (100) |
| Religion | Christianity | 89 (74.2) | 59 (49.2) |
| Religion | Islam | 22 (18.3) | 44 (36.7) |
| Religion | Others | 9 (7.5) | 8 (6.7) |
| Religion | Traditional | 0 (0) | 9 (7.5) |
| Religion | Total | 120 (100) | 120 (100) |
| Tribe | Hausa | 16 (13.3) | 17 (14.2) |
| Tribe | Igbo | 24 (20.0) | 21 (17.5) |
| Tribe | Yoruba | 59 (49.2) | 64 (53.3) |
| Tribe | Others | 21 (17.5) | 18 (15.0) |
| Tribe | Total | 120 (100) | 120 (100) |
| Education | Primary | 13 (10.8) | 26 (21.7) |
| Education | Secondary | 21 (17.5) | 28 (23.3) |
| Education | Tertiary | 79 (65.8) | 46 (38.3) |
| Education | 7 (5.8) | 20 (16.7) | |
| Education | Total | 120 (100) | 120 (100) |
Table 1: Socio-demographic distribution of study subjects (Table 1).
Syphilis Test HIV Negative Subjects N (%)
LabAcon RDT Kit
Perfect RDT Kit
HIV Positive Subjects N (%) Total χ2 (p-value) NEGATIVE 115 (95.5) 106 (88.3) 221 (92.1) 4.806 0.028 POSITIVE 5(4.2) 14 (11.7) 19 (7.9) Total 120 (100) 120 (100) 240 (100) NEGATIVE 117 (97.5) 109 (90.8) 226 (94.2) 5.143 0.023 POSITIVE 3(2.5) 11 (9.2) 14 (5.8) Total 120 (100) 120 (100) 240 (100)
- P<0.05 is considered statistically significant.
Table 2: Occurrence of syphilis infection in relation to the HIV status of the study participants.
| Syphilis Test | HIV Negative Occurrence (%) | HIV Positive Occurrence (%) | Total | ||
|---|---|---|---|---|---|
| LabAcon RDT Kit | Asymptomatic | 0 (0%) | 0 (0%) | 0 (0%) | |
| LabAcon RDT Kit | Symptomatic | 5(100%) | 14 (100%) | 19 (100%) | |
| LabAcon RDT Kit | Total | 5 (100%) | 14 (100%) | 19 (100%) | |
| Perfect RDT Kit | Asymptomatic | 0 (0%) | 0 (0%) | 0 (0%) | |
| Perfect RDT Kit | Symptomatic | 3 (100%) | 11 (100%) | 14 (100%) | |
| Perfect RDT Kit | Total | 3 (100%) | 11 (100%) | 14 (100%) |
Table 3: Distribution of Symptomatic and Asymptomatic Syphilis among the Study Participants.
| Risk Factors | HIV Positive Subjects | HIV Negative Subjects | ||
|---|---|---|---|---|
| χ2 | p-value | χ2 | p-value | |
| Share sanitary facilities with others | 0.052 | 0.819 | 0.248 | 0.618 |
| Share underwear with other | 2.3 | 0.129 | 7.944 | 0.005* |
| Frequency in changing underwear | 1.27 | 0.736 | 0.634 | 0.889 |
| Clean up after toilet | 1.06 | 0.586 | 5.921 | 0.066 |
| History of sexually transmitted infection | 10.76 | 0.002* | 10.763 | 0.001* |
| Engage in unprotected sex | 33.95 | 0.000* | 10.836 | 0.001 |
| Number of sexual partners | 22.56 | 0 | 47.49 | 0.000* |
| Recent change of sex partner | 8.685 | 0.003 | 36.52 | 0.000* |
| No. of sexual intercourse per week | 3.192 | 0.203 | 5.344 | 0.069 |
| Use of contraceptives | 2.43 | 0.118 | 1.162 | 0.281 |
| Frequency of Medical checkup/laboratory test | 3.591 | 0.089 | 1.507 | 0.471 |
Table 4: Risk factors associated with Syphilis infection among the study participants.
Discussion
In this study, the occurrence of syphilis infection among HIV infected subjects using LabAcon test Kit was 11.7%, while that of Perfect Test Kit was 9.2%; both methods showed higher a sero-prevalence rate of syphilis among HIV–infected participants compared to the 5.7% reported by Shimelis, et al. [19] in a study carried out in Southern-Ethiopia. The reason for this disparity may be due to the socio-economic characteristics, as well as the prevailing environmental factors in the geographical local location of the study participants. Another reason may be due to the differences in the sensitivity and specificity of the test kits used.
The 9.2% sero-prevalence recorded in the current study using Perfect Test Kit is slightly lower with previous result in HIV-infected patients in Addis Ababa where an infection rate of 9.8% was reported by Eticha, et al. [22] using the Rapid Plasma Reagin (RPR) and Treponema pallidum haemagglutination assay, for preliminary screening and confirmatory test, respectively. This outcome of this current study conducted in Ogun State, South-West, Nigeria was found to be far lower than the 32.3% reported by Nnoruka, et al. [23] among HIV-syphilis co-infected individuals in Enugu state, South-East, Nigeria. According to National Agency for the Control of AIDS [24], Ogun state has a lower HIV prevalence rate (1.2%) compared to Enugu state (2.1%). This in a way partly explains the lower prevalence rate reported in this study when compared to that of Nnoruka, et al. [23]. This is an indication of a higher susceptibility of HIV patients to syphilis as a result of immunosuppression when compared to HIV negative patients [25]. This can be buttress based on the fact that a lot of HIV infected women in this study engage in unprotected sex and had history of sexually transmitted infection (STI), as evident by significant association using chi-square analysis (p<0.05).
Since HIV and syphilis are both sexually transmissible infections, their association in the same individual is not unusual. HIV infection may alter primary manifestations of syphilis, leading to an atypical presentation of symptoms. Lesions fitting the classic descriptions of painless, solitary ulcers with indurations only occur in 31% of patients with syphilis. As many as 13 out of 14 HIV positive patient engaged in unprotected in unprotected sex, a rate higher than that of similar study by Forbi, et al. [26] in north Central Nigeria where one in three HIV-infected people continue to have unprotected sex after knowing that they are HIV-positive, and unprotected sex often occurs with unknown sero-status or HIV-negative individual.
Results of several epidemiological studies showed that the prevalence of syphilis in Nigeria ranged from 0.125% to 4.1% among pregnant women and commercial sex workers. It is likely that the prevalence of syphilis in Nigeria could be in the same range regardless of occupation in different segments of the Nigerian population.
The rate of syphilis infection in Nigeria is lower compared to other countries in the West-African sub-region. For example, the syphilis-seroprevalence rate of 11%, 20%, and 23.8% has been reported in Ghana, Sierra Leone, and Senegal respectively [27]. The unofficially-unrestricted sales of drug in buses, streets, and markets in Nigeria result in an extensive use of antibiotics, especially ampicillins which can stop syphilis. This could result in the development of antibiotic resistance and efficient transmission of T. palladium, leading to the eventual increase in the number of seropositive individuals over time.
With regard to the HIV-negative subjects examined in this study, the sero-prevalence distribution of syphilis infection using LabAcon Test Kit (4.2%) and that of Perfect Test Kit (2.5%) was found to be much lower compared to the study done by Aboyeji, et al. [27], where 11%, 20%, and 23.8% was reported in Ghana, Sierra Leone, and Senegal, respectively. In another previous study, a much lower prevalence rate of 1.3% was reported among HIV-negative patients in Addis Ababa by Eticha, et al. [22] using the Rapid Plasma Reagin (RPR) and Treponema pallidum haemagglutination assay, for preliminary screening and confirmatory test, respectively. The reason for this discrepancy is also not unconnected to the differences in geographical location of the study participants, as well as the type of test kits employed.
In this study, the sero-prevalence of syphilis infection among HIV-negative subjects examined using LabAcon Kit was 4.2%, while that of Perfect Test Kit was 2.5%. The difference was statistically significant (P=0.028).
On the other hand, it was 11.7% and 9.2%, respectively among HIV-positive subjects. The difference was also statistically significant (P=0.023). In both cases, the Perfect test kit with a sensitivity of 73.7%, demonstrated a reduced detection capability compared to LabAcon test kit. Hence, the latter appear to be more effective and therefore has a higher performance rate in the laboratory diagnosis of syphilis infection. Generally, the specificity of VDRL test may be compromised in HIV infected patients [28, 29, 30, 31]. Many patients with HIV infection have both anticardiolipin-lecithin antibodies and polyclonal gammapathy, which could result in biological false positive results [32]. This is contrary to the result of this study after using Perfect kit with sensitivity of 73.7% and 100% specificity, with however no false positive result. This is in agreement with reliability result on a non- treponemal tests kit with sensitivity of 70%, depending on the stage of disease. The sensitivity of the test approaches 100 percent during the secondary phase of the disease. The specificity of the non-treponemal tests can be used for a rapid and exact quantitative titration of reactive serum samples [33].
All syphilis infected individual in this study were symptomatic regardless of their HIV status. Histories of sexually transmitted infection and engagement in unprotected sex are significant risk factor of syphilis infection among HIV infected subjects. It was observed in this study that HIV subjects with history of sexually transmitted infection had 3.769 times likelihood of having syphilis. While those that engaged in unprotected sex had 0.788 times risk of contracting syphilis. Every other factors in this study was not significantly associated (p>0.05).
Conclusion
In this study, the occurrence of syphilis infection among HIV infected subjects using LabAcon Test Kit was 11.7%, while that of Perfect Test Kit was 9.2%; both methods showed higher occurrence of syphilis among HIV-positive subjects than in their HIV-negative counterparts. All participants in this study with syphilis were symptomatic regardless of their HIV status.
Limitation of study
The study used rapid diagnostic test kits to detect the presence of Treponema pallidium infection among HIV and Non-HIV infected female individuals in Ogun state. Detection using advanced techniques like Polymerase Chain Reaction (PCR) was not possible due to cost and lack of facility for it.
Recommendations
- Routine screening for syphilis should be carried out among HIV infected women, since they are very susceptible to infection holding to the fact that they are immune-compromised.
- Test kit used in the screening of syphilis infection among HIV infected individuals should be validated periodically for their reliability.
- Public awareness on the essence of screening for STIs (including syphilis) among HIV infected individual especially women is on the slack and should be advocated.
- More public awareness to discourage women from engaging in unprotected sex should be intensified.
References
-
WHO (2011) World Health Organization, Prevalence and incidence of selected sexually transmitted infections Chlamydia trachomatis, _Neisseria gonorrhoeae_, syphilis and _Trichomonas vaginalis_: methods and results used by WHO to generate 2005 estimates.
-
LaFond RE, Lukehart SA (2006) Biological basis for syphilis. Clinical microbiology reviews 19(1): 29-49.
-
De Voux A, Kidd S, Grey JA, Rosenberg ES, Thomas LG, et al. (2017) State-specific rates of primary and secondary syphilis among men who have sex with men, United States, 2015. MMWR Morb Mortal Wkly Rep 66(13): 349-354.
-
CDC (2017) Centers for Disease Control and Prevention, 2016 sexually transmitted diseases surveillance.
-
Norris SJ, Cox DL, Weinstock GM (2001) Biology of Treponema pallidum: correlation of functional activities with genome sequence data. Journal of Molecular Microbiology and Biotechnology 3(1): 37-62.
-
Giacani L, Lukehart SA (2014) The endemic treponematoses. This is a contemporary review of the origins, global epidemiology, and clinical features of the novenereal treponematoses and their continuing threat to worldwide health. Clinical Microbiology Reviews. 27(1): 89-115.
-
Sena AC, Pillay A, Cox DL, Radolf JD (2015) Treponema pallidium In: Manual of Clinical Microbiology. Jorgensen JH, et al. (Eds.), ASM Press, Washington DC, USA, pp: 1055–1081.
-
Radolf JD, Tramont EC, Salazar JC (2014) In: Mandell, Douglas and Bennett’s Principles and Practice of Infectious Diseases. Bennett JE, Dolin R, Blaser MJ, et al. (Eds.), Churchill Livingtone Elsevier, Philadelphia pp: 2684-2709.
-
Clark T, Jeanne J, Sheffield S (2018) Treponema pallidium. In: 2nd (Edn.), pp: 688-692.
-
Mutua FM, M’imunya JM, Wiysoge CS (2012) Genital ulcer disease treatment for reducing sexual acquisition of HIV. Cochrane Database Syst Rev 8: CD007933.
-
Hosseini M, SeyedAlinaghi S, Kheirandish P, Esmaeli Javid G, Shirzad H, et al. (2010) Prevalence and correlates of co-infection with human immunodeficiency virus and hepatitis C virus in male injection drug users in Iran. Arch Iran Med 13(4): 318-323.
-
Wang YJ, Chi CY, Chou CH, Ho CM, Lin PC, et al. (2012) Syphilis and neurosyphilis in human immunodificiency virus-infected patients: A retrospective study at a teaching hospital in Taiwan. J Microbiol Immunol Infect 45(5): 337-342.
-
Blank LJ, Rompalo AM, Erbelding EJ, Zenilman JM, Ghanem KG (2011) Treatment of syphilis in HIV-infected subjects: a systematic review of the literature. Sexually Transmitted Infections 87: 9-16.
-
Zetola NM, Klausner JD (2007) Syphilis and HIV infection: an update. Clin Infect Dis 44(9): 1222-1228.
-
White RG (2004) Can population differences explain the contrasting results of the Mwanza, Rakai, and Masaka HIV/sexually transmitted disease intervention trials? A modeling study. J Acquir Immune Defic Syndr 37: 1500- 1513.
-
Douglas JM (2009) Penicillin treatment of syphilis: clearing away the shadow on the land. JAMA 301: 769- 771.
-
Lukehart SA (2004) Macrolide resistance in Treponema pallidum in the United States and Ireland. N Engl J Med 351: 154-158.
-
Pourhoseingholi MA, Vahedi M, Rahimzadeh M (2013) Sample size calculation in Medical studies. Gastroenterology and Hepatology from Bed to Bench 6(1): 14-17.
-
Shimelis T, Kinfe L, Ambachew H, Tadesse E (2015) Syphilis among people with HIV infection in southern Ethiopia: sero-prevalence and risk factors. BMC Infectious Diseases 15: 189.
-
Olayanju AO, Afolabi T, Ezigbo ED, Enitan SS, Oluwatayo BO (2018) Assessment of Antiphospholipid Antibodies, CD4 Count and Some Haematological Parameters in HIV Patients attending a Tertiary Health Institution in South-Western Nigeria. International Blood Research & Reviews 8(2): 1-14.
-
Digban AK, Osula I, Adesina EB, Aghatise K, Enitan SS (2017) Assessment of CD4 count and some haematological parameters of HIV positive patients co- infected with Hepatitis B virus in Osun State, Nigeria. International Blood Research & Reviews 7(4): 1-13.
-
Eticha BT, Sisay Z, Alemayehu A, Shimelis T (2013) Seroprevalence of syphilis among HIV-infected individuals in Addis Ababa, Ethiopia: a hospital-based cross-sectional study. BMJ open 3(4): e002566.
-
Nnoruka EN, Ezeoke ACJ (2005) Evaluation of syphilis in patients with HIV infection in Nigeria. Tropical Medicine & International Health 10(1): 58-64.
-
National Agency for the Control of AIDS (NACA) (2020) Nigeria Prevalence Rate for HIV/AIDS.
-
Forbi JC, Agwale SM (2009) Inverted CD4+/CD8+ ratio associated with AIDS event and death in HIV-1 infected individuals in Nasarawa State, Nigeria. Tanzania journal of health research 11(3): 144-148.
-
Aboyeji AP, Nwabuisi C (2003) Prevalence of sexually transmitted diseases among pregnant women in Ilorin, Nigeria. Journal of Obstetrics and Gynaecology 23(6): 637-639.
-
Augenbraun MH, DeHovitz JA, Feldman J, Clarke L, Landesman S, et al. (1994) Biological false-positive syphilis test results for women infected with human immunodeficiency virus. Clinical infectious diseases 19(6): 1040-1044.
-
Rompalo AM, Cannon RO, Quinn TC, Hook III EW (1992) Association of biologic false-positive reactions for syphilis with human immunodeficiency virus infection. Journal of Infectious Diseases 165(6): 1124-1126.
-
Rusnak JM, Butzin C, McGlasson D, Blatt SP (1994) False-positive rapid plasma reagin tests in human immunodeficiency virus infection and relationship to anti-cardiolipin antibody and serum immunoglobulin levels. Journal of Infectious Diseases 169(6): 1356-1359.
-
Drabick J, Tramont E (1990) Utility of the VDRL test in HIV-seropositive patients. The New England journal of medicine 322(4): 271.
-
Bala K, Uma C, Ritu A, Nidhi G, Narinder K (2009) Seroprevalence of syphilis in apparently healthy population: a five-year study. Journal of Infectious Diseases and Antimicrobial Agents 26(2): 55-59.
-
Pope V, Norris SJ, Johnson RE (2007) Treponema and other human host-associated spirochetes. In: Murray PR, Baron EJ, Jorgensen JH, Landry ML, Pfaller MA, et al. (Eds.), Manual of clinical microbiology 9th (Edn.), ASM Press, Washington, DC 1: 987-1003.
- Are the Vaccines the Only Solution to Prevent the COVID-19 Pandemic? Part Two
- Clinical Characteristics of Women in this New Global Immunodeficiency
- Cell Dynamics in HIV Pathogenesis: Insights and Implications
- Determination of the CDR (CDR1, CDR2) « Complementary- Determining Region Invertebrate Primitive Antibody from Sea Star »
- Prioritizing Care for High-Risk COVID-19 Patients in the EU: 10 Civic Recommendations to the Institutions
- Comprehensive Insights into ModRNA Vaccines: Persistent PP-Spike Recombinant Protein, Hyperimmune/Inflammatory Reactions, Thrombotic Vasculopathy, Chronic Organ Complications and Excess Deaths