Covid-19: Natural Immunity Versus Vaccine Immunity Abstract
It should not be necessary to write an article to demonstrate the superiority of natural immunity over vaccine immunity, but it is necessary in view of the many underhanded attacks that tend to make artificial immunity seem more effective. Furthermore, it is officially recommended to vaccinate people who have already been infected with Covid-19. Survivors of the 2003 SARS-CoV have cellular immune memory more than 17 years after infection. Numerous studies have explored humoral (antibody) and cellular immunity to SARS-CoV-2 after Covid-19 infection: it persists for at least one year (and even 14 months) in a robust manner in convalescents and would be of better quality than vaccine immunity: natural antibodies are more potent, have a broader spectrum, and are able to evolve against variants more efficiently than vaccine antibodies. These in vitro studies are confirmed by the protection against reinfections conferred by a primary infection, particularly in early and highly vaccinated countries such as Israel and the United Kingdom. Vaccination of a primo-infected person could also decrease the effectiveness of his natural immunity against future reinfections. Neutralizing antibodies may not be the correct correlate of protection against infection, as high levels of neutralizing antibodies have been found in patients with severe Covid, and vaccinated patients, who are more susceptible to reinfection than primary patients, have antibody levels equivalent to or higher than those observed in primary patients. The neutralizing capacity of these antibodies directed against the membrane spike protein is measured in vitro. This neutralizing capacity may be different in vivo; it may be diminished by the presence of antibodies that facilitate infection; and antibodies are produced against other viral antigens during natural infection. Cellular immunity could be the right correlate of protection and this type of response could be of lower quality in vaccinated subjects. In addition, vaccination of convalescent subjects could be risky: more systemic adverse events are observed in convalescent subjects than in naïve subjects after the first dose of vaccine. Vaccination may decrease the ability to respond to future variants. It could also have a non- specific effect of remodeling the innate immune response by decreasing the potential response to other viruses or cancers and by modifying the course of inflammatory and autoimmune diseases. The natural immunity of a population should therefore be explored before proposing vaccination: up to 50% of the population may have been infected in some countries.
Introduction
It should not be necessary to write this article to demonstrate that natural immunity is superior to vaccine immunity: indeed, since the appearance of life on Earth, natural immunity has been developing in all living beings in response to predators and all this without vaccines! Innate immunity preceded adaptive immunity and allowed us to recognize foreign pathogens, eliminate them and maintain an immune memory [1].
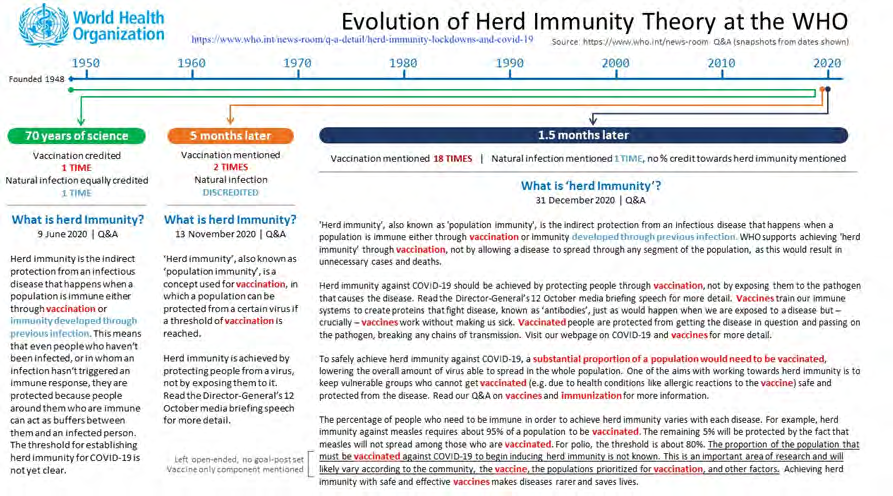
Until June 2020, innate immunity, related to the human innate and adaptive/acquired immune system, was recognized by the WHO as a key component of herd immunity to novel pathogens.
Until November 2020, the WHO admitted that immunity can be provided by infection or by vaccination, on November 13, 2020, the WHO affirms that herd immunity of a population can only be achieved by vaccination and not by natural infection. This is reaffirmed on December 31, 2020 for Covid-19, while recognizing that we do not know the threshold of vaccine coverage to be obtained to achieve this herd immunity. (Only the December 31, 2020 definition is still accessible, https://www.who.int/news-room/q-a-detail/ herd-immunity- lockdowns-and-covid-19, the previous ones are visible on the screenshot below) (Figure 1).
In a recent publication, the John Hopkins Institute only mentions vaccine immunity in a discussion about the hypothetical herd immunity to be expected against Covid [2].
Immunity Measured in Vitro after Infection with SARS-CoV-2
Studies comparing in vitro (antibody assay, neutralizing activity, memory B and T cells) natural and vaccine immunity seem to show superiority of natural immunity. It seems that vaccination modifies the immune response of convalescents and not necessarily in a good way: it could reduce the subsequent capacity of convalescents to react to future variants. Publications (examples below) show that neutralizing antibodies and memory B (humoral immunity) and T (cellular immunity) cells persist for at least one year in convalescents. Protection against SARS-CoV-2 infection could last for years [6].
Humoral Immunity (Antibodies)
It is normal to observe a drop in circulating antibody levels after an infection, as happens with all infections; otherwise the blood would be thickened by all the antibodies that accumulate over a lifetime. At the same time, the immune memory is built and refined.
“The slight decrease in antibodies observed in convalescent individuals does not reflect a real decline in humoral immunity, but rather a contraction of the immune response, while maturation of antibody affinity occurs and anti-Spike memory B cells persist [7].
Several publications suggest that natural immune memory is even better than vaccine memory. According to Cho, et al. [8] natural antibodies are more potent and broader spectrum than vaccine antibodies. As discussed below, the neutralizing power of plasma measured in vitro is unlikely to be evidence of protection against infection. Antibodies to the RBD (receptor binding domain) of the spike protein and to the whole spike persist for at least 1 year after recovery from Covid, and the level of anti-RBD antibodies correlates with the level of neutralizing antibodies [9].
In vaccinated individuals, antibody levels decrease by 40% per month and by less than 5% per month in convalescents [10].
Cellular Immunity
In recovered COVID-19 patients, SARS-CoV-2-specific CD8+ T-cell responses remained largely intact and could recognize virtually all mutations of the variants studied [11].
In dialysis patients, a German team found better humoral and cellular immunity in convalescents compared with vaccinated patients: this relates to neutralizing antibody levels and T-cell responses directed against the spike protein.
Levels of CD4+ S-reactive T cells, helper T cells, and memory effector cells are higher in convalescents than in vaccines [12].
Most COVID-19 patients induce a broad-based immune defense against SARS-CoV-2 infection, encompassing antibodies and memory B cells recognizing both the RBD and other regions of the spike, broadly specific and polyfunctional CD4+ T cells, and polyfunctional CD8+ T cells. The immune response to natural infection is likely to provide some degree of protective immunity, even against SARS-CoV-2 variants, because CD4+ and CD8+ T-cell epitopes are likely to be conserved [13].
According to a meta-analysis of 18 studies of SARS-CoV-2 epitopes recognized by T cells of Covid-19 convalescents: The high diversity of epitopes not confined to the S protein does not appear to be affected by VOC variants, at least before the arrival of the delta variant [14].
A recent Israeli publication of September 21, 2021, shows the persistence of humoral immunity in convalescents for 14 months, which is not the case in vaccinated individuals. Bypass of innate immunity by mRNA vaccines could affect the ability of the immune system to maintain sufficient levels of long-lived plasma cells [15].
Protection against Reinfection by Infection Acquired Immunity
These in vitro observations of antibody and memory cell levels are well confirmed by looking for reinfections in convalescents: these are very rare.
Numerous publications (see for bibliography the recent BMJ article [16]) show that the rate of reinfection is very low (less than 1%) following a first infection with SARS-CoV-2. The vast majority of these reinfections are not reinfections as such since they are asymptomatic: they are simply nasal carriage of virus without systemic infection. This is not surprising for a cold virus; the nose is an immune sanctuary where blood antibodies do not circulate.
• What is the proportion of people in the world who are naturally immune to infection? There is patchy information: in Kenya in November 2020, more than 1/3 of the population was HIV positive [17]; in India in January 2021, 25% of the population was seropositive18. In China, in Wuhan, the epicenter of the epidemic, a very low rate of seropositivity has been found (less than 4% in April 202019).
Infected persons with few or no symptoms do not develop this type of SARS-CoV-2 specific antibodies, they would have been protected by their cross immunity to common cold coronaviruses [18].
In France, the HAS estimates that 23% of the population has been infected while only 8% have been detected by PCR or antigenic test [19, 20].
It is estimated that almost half of all Americans have been infected with SARS-CoV-216. By August 2020, 40% of the Malagasy population (estimated from blood donors) would have been seropositive [21]. One obstacle to these seroprevalence studies is that serological tests lack standardization [22].
• Another problem is that one can be immune and not have antibodies (anti-S or other antibodies) According to publications from 2020, people who are infected but have not developed symptoms have a T cell reaction but no antibodies [23] (for a review); this is confirmed in 2021 : Le Bert, et al. [24] search seropositive asymptomatic for anti-NP-IgG antibodies (antibodies to the virus nucleocapsid): all seropositive have a highly functional virus-specific cellular immune response. In addition, individuals who are anti-NP IgG negative also have T cells that react specifically with SARS-CoV-2 antigens. What is a Reinfection?
The CDC defines reinfection as a positive test regardless of symptoms (and unvaccinated people are tested more than vaccinated people, due to the health pass) [25]. The only studies that claim that infection does not protect against reinfection do not clearly define the term reinfection: a positive PCR with a Ct of 35 (low viral load or false positive) without symptoms cannot be defined as reinfection.
The study of reinfections shows that infection provides at least as much protection against infection and probably more than vaccination.
As early as April 2021, F Krammer, et al. [26] proposed that natural immunity was better than vaccine immunity, based on a British study comparing primary infected and vaccinated healthcare workers. Since this publication, the continuation of this SIREN study has concerned reinfections with the delta variant and shows the superiority of natural immunity [27]. Of the 9,831 healthcare workers who were already infected with Covid before the study began, 51 were reinfected between April and July 2021, the period of delta variant circulation. Among these 51 persons, 45 were vaccinated since at least 21 days after dose 1 or 14 days after dose 2, nothing is specified about the 6 remaining persons: either they were not vaccinated or, they were infected in the few days following dose 1 or 2 because of the ADE (antibody dependent enhancement = facilitation of infection by vaccine antibodies): why is it not specified? All in all, infection protects against reinfection, which is not the case with vaccination.
According to a French study, the relative reduction in the incidence of reinfection by SARS- CoV-2 is 96.7% in convalescents Gallais, et al. [28] compared with non-infected people. In young army recruits, reinfections (in HIV-positive individuals) are 5 times rarer than infections in seronegative individuals, and reinfected individuals are most often asymptomatic [29].
Covid epidemic in a gold mine in French Guiana with gamma variant, June 2021 [30]. Key observations: Covid recoveries are not infected (unless they were vaccinated), 15 out of 25 vaccinated are infected (recovered or not), unvaccinated are infected last, so it is possible that the vaccinated have infected the unvaccinated. The vaccinated have a slightly higher viral load than the unvaccinated. No severe form is observed despite the strong presence of risk factors in infected minors.
And finally, we must of course mention the studies carried out in Israel, the country vaccinated the earliest on a large proportion of the population. Gazit, et al. (Israel) [31] reported that never-infected individuals vaccinated against SARS-CoV-2 had a 13.06-fold increased risk of infection with the Delta variant (or 5.96-fold depending on the method of calculation) compared with previously infected individuals. The increased risk was also significant for symptomatic disease. Compared with primary infected individuals, vaccinated individuals not infected with SARS-CoV-2 had a 27-fold increased risk of symptomatic infection (or 7-fold increased risk by calculation) of symptomatic disease. Vaccinated individuals also had a higher risk of COVID-19- related hospitalizations (6.7-fold) than previously infected individuals. This study demonstrated that natural immunity confers longer-lasting and stronger protection against infection, symptomatic illness, and hospitalizations caused by the SARS-CoV-2 Delta variant, compared with immunity induced by the two-dose BNT162b2 vaccine. Those previously infected with SARS-CoV-2 who received a single dose of the vaccine gained additional protection against the Delta variant.
It should be added, of course, as usual, that post- vaccination Covids are excluded since, in infected and vaccinated individuals, they are only counted from 7 days after the injection. The ADE is not taken into account, so the results may be unfavorable to vaccination in the infected, we can’t know!
On the other hand, people who were infected before February 28, 2021 are excluded, so basically the elderly and frail people (vaccinated first from December 2020): the result would be even more unfavorable to the vaccine if they were included.
This study was reported in Science Mag and summarized as follows: Israelis who had an infection were more protected against the Delta variant of the coronavirus than those who received a COVID-19 vaccine [32].
Meta-analysis of natural immunity data (September 21, 2021) [33] Natural immunity is equivalent to or superior to vaccination in protecting against Covid: no study concludes that vaccine protection is superior to natural immunity with statistical certainty, but observational studies have confirmed the benefit of protection by natural immunity.
The benefit of vaccinating people who have already contracted Covid is zero or very small (3 out of 4 studies find no benefit of vaccinating convalescents and the additional protection found by pooling all studies is 0.004%).
• Vaccine immunity is classically associated with the titer of neutralizing antibodies in vitro, but are neutralizing antibodies the right correlate of protection?. There are conflicting results on the persistence of neutralizing antibodies after infection: in some studies these antibodies persist for at least one year, in others their level decreases rapidly, perhaps due to the methods used, which differ from one study to another?.
To measure the neutralizing power of a serum in vitro, these studies use either live viruses cultured on different types of cells, or reconstituted pseudoviruses carrying mutated spike proteins of SARS-CoV-2 on their surface.
According to a meta-analysis [34], the levels of neutralizing antibodies induced by mRNA vaccines against SARS-CoV-2 variants were similar to or higher than those obtained from naturally infected individuals. This is not consistent with the low rate of reinfection in primary infected versus vaccinated individuals, as seen above in the United Kingdom [27] reinfections with the delta variant in health care workers are only in fully or partially vaccinated individuals.
According to numerous studies, the level of neutralizing antibodies and their spectrum against the variants is significantly increased after vaccination in previously infected individuals [35].
According to Stamatos [36], vaccination can increase the level of neutralizing antibodies against variants in primary infected individuals up to 1000-fold. According to Reynods, et al. [37], naive vaccines have a similar antibody response to that of naturally infected individuals but T cell responses are more limited and sometimes absent.
On the contrary, according to Havervall, et al. [38] the levels of neutralizing antibodies to wild-type and mutant strains 12 months after natural infection are lower than in vaccines.
According to Planas, et al. [39] convalescent sera lose their ability to neutralize the delta variant in vitro over time. A single dose of vaccine yields almost no neutralizing antibodies to the delta variant, regardless of the vaccine.
In summary, vaccination would result in higher levels of neutralizing antibodies than natural infection, which contradicts the different rates of reinfection observed between infected and vaccinated individuals: are neutralizing antibodies the right correlate of protection?.
According to Prof. La Scola in a video, the presence of high levels of neutralizing antibodies in vaccinated individuals does not prevent them from being infected [40]. There is a correlation between antibody levels measured by Elisa and serum neutralization but no correlation between in vitro neutralizing antibody levels and protection against infection: “In this study, 5% of the vaccinated individuals became infected, compared with only 0.23% of those who had Covid-19 disease, so the effect of cellular immunity is not objectified by serum neutralization; indeed, most of the vaccinated individuals have a high level of antibodies. This is confirmed by other publications [16].
The neutralizing Ac acquired after infection varies greatly depending on the variant that caused the infection; mRNA vaccines induce higher levels of neutralizing antibodies than the infection [41] and yet the infection protects better than the vaccine and severe Covid patients may have high levels of neutralizing antibody.
The theoretical explanation for this lack of correlation between in vitro neutralizing antibodies and protection could be found here: virus neutralization is studied in vitro, under conditions totally different from what happens in vivo, and may not reflect what happens in the body [42].
Immune Memory Concerns other Epitopes than those of the Spike
Almost all of the studies concern anti-spike antibodies, however, The majority of epitopes targeted by CD8+ are found in the internal proteins of the virus or in the NSPs
[non-structural proteins, which do not include the spike protein] [43].
Protection from infection is likely due as much to immune memory as to persistence of high antibody levels [44].
• Neutralizing antibodies may lose their properties in the presence of facilitating antibodies produced by vaccination. The present article cannot elaborate on this subject, which has been discussed in recent publications [45].
The role of mucosal immunity, which is stimulated by natural infection and not by IM vaccination, should also be mentioned: “Almost all studies of the immune response in COVID-19 have focused exclusively on serum antibodies and systemic cell-mediated immunity, including innate responses. Mucosal immunity and secretory and circulating IgA antibodies play an important role in COVID-19, and it is important to elucidate this in order to understand in particular the asymptomatic and mild states of infection, which appear to represent the majority of cases [46].
“Vaccination of never-infected persons may not induce strong humoral immunity in the respiratory mucosa, because neutralizing antibodies to SARS-CoV-2 are rarely detected in nasal swabs from vaccinated persons. If it turns out that current vaccination strategies fail to elicit robust humoral and cell-mediated immune responses in the respiratory tract, then strategies to better elicit SARS-CoV-2-specific B and T cells in the mucosa of never-infected individuals should be considered-for example, by implementing intranasal mRNA immunization, which is more likely to induce sterilizing immunity [47].
• Protection against Covid may also be due to cross- immunity to common cold coronaviruses [23] A recent study shows that children have SARS-CoV-2 reactive cells in their tonsils, even though they have not been exposed to the virus, so pre-existing cellular cross-immunity may explain their resistance to Covid [48].
• Is it appropriate to vaccinate Covid convalescents? The case of long Covid [49]. Two theories explain long covids: either the virus persists and causes chronic inflammation, or it is autoimmunity through the production of autoantibodies against viral proteins with similarities to human proteins. Vaccination can aggravate this phenomenon but also improve it, we do not know this in advance.
mRNA vaccines aberrantly direct T-cell responses in patients with neurological sequelae of Covid infection (Covid long): is it appropriate to vaccinate them? [50].
• Adverse effect of vaccine on ability to respond to new variants Vaccination of convalescent subjects may be risky: convalescent subjects have more systemic adverse events than naïve subjects after the first dose of vaccine [51]. In addition; vaccination does not improve the ability to respond to new variants and may even be harmful.
One study found somewhat contradictory results: vaccination increased humoral and memory response in convalescents by 30 to 50 times. The neutralizing activity in unvaccinated convalescents is weakened against the variants (the delta variant is not tested) but increased after vaccination in convalescents.
The neutralization spectrum of antibodies collected in convalescents broadens with time and after one year the potency and neutralization spectrum are increased against the variants Vaccination does not broaden the spectrum of clonal expansion compared to unvaccinated convalescents after one year. RBD-binding antibody affinity is not increased by vaccination after one year, no difference in neutralizing effect is observed [52].
The second dose of BNT162b2 vaccine results in a reduction in cellular immunity in persons who have recovered from COVID-19, suggesting that a second dose, according to the current standard vaccination regimen, may not be necessary in persons previously infected with SARS- CoV-2: the second dose of vaccine not only does not enhance humoral immunity, but also determines a contraction of the spike-specific T-cell response [53].
The natural immunity of the infected is hampered by a subsequent anti-Covid vaccination Vaccination of convalescents reduces the ability to produce broad- spectrum antibodies against future variants; unvaccinated convalescents have this ability [54].
The affinity of natural antibodies increases more with time than that of vaccine antibodies. After vaccination of primary patients, the level of neutralizing antibodies increases, but not the potency of these antibodies or the ability to evolve to broad-spectrum protection thereafter. This is also true for the delta variant.
The difference in memory cell compartments in response to infection or vaccination (mRNA) is consistent with the greater level of protection conferred by natural infection with the variants.
A relative reduction in reactivity of sera with the B.1.1.7 variant compared to the Wuhan-1 variant is seen after the second booster immunization. These data allow comparison of the different vaccines in terms of anti-S antibody production and call into question the value of repeated immunization with the same S protein sequence. In convalescents, vaccination caused a relative loss of recognition of the B.1.1.7 variant beginning as early as 15 days after the first dose of Pfizer and worsening thereafter [55]. The CD4+ T cell response is decreased in convalescents after vaccination compared to naïve individuals: vaccination is thought to damage the T cell response. After vaccination, the magnitude of the immune response appears to be lower in convalescents than in naïve individuals [56].
Pfizer’s vaccine could reshape the innate immune response to other pathogens. It would induce immune tolerance that could either be beneficial in Covid-19 characterized by hyperinflammation or be deleterious by decreasing the response to other viral infections [and cancers]. This vaccine could also interfere with other vaccinations such as influenza, which is likely to be given at the same time in early fall [57].
This reprogramming of immune immunity could be long-lasting due to epigenetic phenomena: “Training” of the innate immune response plays an important role both in diseases where host defense is impaired, such as cancers, and in auto inflammatory and autoimmune diseases, in which an exacerbated “trained” immunity phenotype could contribute to the pathogenesis of the disease. The impact of immune training, and more generally of epigenetic rewiring in the various priming, adaptation, or tolerance processes during disease, deserves further study [58].
Conclusion
Natural immunity to Covid-19 (i.e., obtained after natural infection with the virus) is therefore certainly robust and durable. Work on post-vaccination immunity is mainly concerned with so-called “neutralizing” antibodies in vitro. The levels of these antibodies may not be a good correlate of protection because studies often find higher levels of antibodies after vaccination than after infection. However, reinfections are much more frequent in vaccinated patients than in convalescents. Protection against Covid-19 could rather depend on immune memory (due to memory T and B cells that persist long after infection) and seems to be of better quality than that conferred by vaccines.
In addition, vaccination of convalescent subjects could be risky: more systemic adverse events are observed in convalescent subjects than in naïve subjects after the first dose of vaccine. Vaccination may decrease the ability to respond to future variants. It could also have a non- specific effect of remodeling the innate immune response by decreasing the potential response to other viruses or to cancers and by modifying the course of inflammatory and autoimmune diseases.
References
-
Tsakou Ngouafo L, Paganini J, Kaufman J, Pontarotti P (2020) Origins of the RAG transposome and the MHC. Trends Immunol 41(7): 561-571.
-
Rethinking Herd Immunity and the Covid-19 Response End Game.
-
Callow KA, Parry HF, Sergeant M, Tyrrell DA (1990) The time course of the immune response to experimental coronavirus infection of man. Epidemiol Infect 105(2): 435-446.
-
Ng OW, Chia A, Tan AT, Jadi RS, Leong HN (2016) Memory T cell responses targeting the SARS coronavirus persist up to 11 years post-infection. Vaccine 34(17): 2008- 2014.
-
Le Bert N, Tan AT, Kunasegaran K, Tham CYL, Hafezi M (2020) SARS-CoV-2-specific T cell immunity in cases of COVID-19 and SARS, and uninfected controls. Nature 584(7821): 457-462.
-
Huang AT, Garcia-Carreras B, Hitchings MDT, Yang B, Katzelnick LC, et al. (2020) A systematic review of antibody mediated immunity to coronaviruses: kinetics, correlates of protection, and association with severity. Nat Commun 11: 4704.
-
Dan JM, Mateus J, Kato Y, Hastie KM, Yu ED, et al. (2021) Immunological mem- ory to SARS-CoV-2 assessed for up to 8 months after infection. Science 371(6529): eabf4063.
-
Alice C, Muecksch F, Schaefer-Babajew D, Wang Z, Finkin S, et al. (2021) Anti- SARS-CoV-2 Receptor Binding Domain Antibody Evolution after MRNA Vaccination. bioRxiv.
-
Chengqian F, Shi J, Fan Q, Wang Y, Huang H, et al. (2021) Protective Humoral and Cellular Immune Responses to SARS-CoV-2 Persist up to 1 Year after Recovery. Nature Communications 12(1).
-
Israel A, Shenhar Y, Green L, Merzon E, Cohen AG, et al. (2021) Large-scale study of antibody titer decay following BNT162b2 mRNA vaccine or SARS-CoV-2 infection. medRxiv.
-
Redd AD, Nardin A, Kared H, Bloch EM, Pekosz A, et al. (2021) CD8+ T cell responses in COVID-19 convalescent individuals target conserved epitopes from multiple prominent SARS-CoV-2 circulating variants. medRxiv 2021.02.11.21251585.
-
Blazquez-Navarro A, Safi L, Meister TL, Pfaender S, Roch T, et al. (2021) Superior cellular and humoral immunity toward SARS-CoV-2 reference and alpha and beta VOC strains in COVID-19 convalescent as compared to the prime boost BNT162b2 vaccinated dialysis patients. Kidney international 100(3): 698-700.
-
Cohen KW, Linderman SL, Moodie Z, Czartoski J, Lai L, et al. (2021) Longitudinal analysis shows durable and broad immune memory after SARS-CoV-2 infection with persisting antibody responses and memory B and T cells. medRxiv 2021.04.19.21255739.
-
Abdul Quadeer A (2021) Landscape of epitopes targeted by T cells in 852 individuals recovered from COVID-19: Meta-analysis, immunoprevalence, and web platform. Cell reports medicine 2(6).
-
Markovitch D (2021) The longitudinal kinetics of antibodies in COVID-19 recovered patients over 14 months.
-
BMJ (2021) Vaccinating people who have had covid-19: why doesn’t natural immunity count in the US?. BMJ pp: 374.
-
Ngere IA (2021) High Seroprevalence of SARS-CoV-2 Eight Months After Introduction in Nairobi, Kenya.
-
Murhekar MV (2021) SARS-CoV-2 seroprevalence among the general population and healthcare workers in India, December 2020-January 2021. 108:145-155.
-
Xu X, Sun J, Nie S (2020) Seroprevalence of immunoglobulin M and G antibodies against SARS-CoV-2 in China. Nat Med 26: 1193-1195.
-
HAS (2021) Covid-19: TRODs to optimize the use of available vaccine doses.
-
Schoenhals M, Rabenindrina N, Rakotondramanga JM, Dussart P, Randremanana R, et al. (2021) SARS- CoV-2 antibody seroprevalence follow-up in Malagasy blood donors during the 2020 COVID-19 Epidemic. EBioMedicine, Elsevier 68: 103419.
-
Theel ES (2020) The Role of Antibody Testing for SARS-CoV-2: Is There One?. J Clin Microbiol 58(8): e00797-e00820.
-
Banoun H (2020) COVID19: Cross-Immunity with Other Coronaviruses, Immunopathological Phenomena. pp: 8.
-
Bert NL (2021) Highly functional virus-specific cellular immune response in asymptomatic SARS-CoV-2 infection. J Exp Med 218(5): e20202617.
-
Cavanaugh AM (2021) Reduced Risk of Reinfection with SARS- CoV-2 After COVID-19 Vaccination-Kentucky, May–June 2021. MMWR 70(32): 1081-1083.
-
Krammer F (2021) Correlates of protection from SARS- CoV-2 infection. 379(10283): 1421-1432.
-
(2021) Investigation of SARS-CoV-2 variants: technical briefings.
-
Floriane G, Gantner P, Bruel T, Velay A, Planas D, et al. (2021) Evolution of Antibody Responses up to 13 Months after SARS-CoV-2 Infection and Risk of Reinfection. EBioMedicine 71(103561).
-
Letizia AG (2021) SARS-CoV-2 seropositivity and subsequent infection risk in healthy young adults: a prospective cohort study. Respiratory Medicine 9(7): 712-720.
-
Vignier N (2021) Breakthrough Infections of SARS-CoV-2 Gamma Variant in Fully Vaccinated Gold Miners, French Guiana, 2021. CDC 27(10).
-
Sivan G, Shlezinger R, Perez G, Lotan R, Peretz A, et al. (2021) Comparing SARS-CoV-2 Natural Immunity to Vaccine-Induced Immunity: Reinfections versus Breakthrough Infections. medRxiv.
-
Wadman M (2021) Having SARS-CoV-2 once confers much greater immunity than a vaccine—but no infection parties, please.
-
Shenai MB (2021) Equivalency of Protection from Natural Immunity in COVID-19 Recovered Versus Fully Vaccinated Persons: A Systematic Review and Pooled Analysis. medRxiv.
-
Chen X, Chen Z, Azman AS, Sun R, Lu W, et al. (2021) Neutralizing antibodies against SARS-CoV-2 variants induced by natural infection or vaccination: a systematic review and pooled meta-analysis. Clin Infect Dis pp: ciab646.
-
Crotty S (2021) Hybrid immunity. Science 327(6549): 1392-1393.
-
Stamatatos L (2021) mRNA vaccination boosts cross- variant neutralizing antibodies elicited by SARS-CoV-2 infection. Science pp: eabg9175.
-
Reynolds CJ (2021) Prior SARS-CoV-2 infection rescues B and T cell responses to variants after first vaccine dose. Science 372: 6549.
-
Havervall S (2021) Neutralization of VOCs including Delta one year post COVID-19 or vaccine. medRxiv.
-
Planas D, Veyer D, Baidaliuk A, Staropoli I, Benhassine FG, et al. (2021) Reduced sensitivity of SARS-CoV-2 variant Delta to antibody neutralization. Nature 596: 276-280.
-
Séroneutralisation SARS-CoV-2: effets sur les variants.
-
Jaafar R, Boschi C, Aherfi S, Bancod A, Bideau ML, et al. (2021) High individual heterogeneity of neutralizing activities against the original 4 strain and 9 different variants of SARS-CoV-2. Research Square, pp: 1-46.
-
Banoun H (2021) The role of antibodies in the light of the theory of evolution. Afr J Biol Sci 3(3): 1-9.
-
Kared H, Redd AD, Bloch EM, Bonny TS, Sumatoh H, et al. (2021) SARS-CoV-2–specific CD8+ T cell responses in convalescent COVID-19 individuals. J Clin Invest 131(5): e145476.
-
Mentesh AV, Dror Y, Kaspa RT, Markovitch D, Kournos T, et al. (2020) SARS-CoV-2 specific memory B cells frequency in recovered patient remains stable while antibodies decay over time. MedRxiv, pp: 1-25.
-
Liu Y, Soh WT, Kishikawa JI, Hirose M, Nakayama EE, et al. (2021) An infectivity-enhancing site on the SARS-CoV-2 spike protein targeted by antibodies. Cell 184(13): 3452- 3466.
-
Yahi N, Chahinian H, Fantini J (2021) Enhancing anti- SARS-CoV-2 antibodies recognize both the original Wuhan/D614G strain and Delta variants. A potential risk for mass vaccination ?. Journal of Infection, pp: 1-2.
-
Liu Y, Arase N, Kishikawa JI, Hirose M, Li S, et al. (2021) The SARS-CoV-2 Delta variant is poised to acquire complete resistance to wild-type spike vaccines. BioRxiv, pp: 1-31.
-
Amanat F, Thapa M, Lei T, Sayed Ahmed SM, Adelsberg DC, et al. (2021) The plasmablast response to SARS- CoV-2 mRNA vaccination is dominated by non- neutralizing antibodies that target both the NTD and the RBD. MedRxiv pp: 1-29.
-
Russell MW, Moldoveanu Z, Ogra PL, Mestecky J (2020) Mucosal Immunity in COVID-19: A Neglected but Critical Aspect of SARS-CoV-2 Infection. Front Immunol 11: 611337.
-
Neidleman J, Luo X, McGregor M, Xie G, Murray V, et al. (2021) mRNA vaccine-induced T cells respond identically to SARS-CoV-2 variants of concern but differ in longevity and homing properties depending on prior infection status. Elife 10: e72619.
-
Niessl J, Sekine T, Lange J, Konya V, Forkel M, et al. (2021) Identification of resident memory CD8+ T cells with functional specificity for SARS-CoV-2 in unexposed oropharyngeal lymphoid tissue. Sci Immunol 6(64): eabk0894.
-
(2021) What’s causing long COVID?. Interview with Akiko Iwasaki, Yale University. The Naked Scientists.
-
Visvabharathy L, Hanson B, Orban Z, Lim PH, Palacio N, et al. (2021) Neuro-COVID long-haulers exhibit broad dysfunction in T cell memory generation and responses to vaccination. medRxiv, pp: 1-49.
-
Krammer F, Srivastava K, Alshammary H, Amoako AA, Awawda MH, et al. (2021) Antibody Responses in Seropositive Persons after a Single Dose of SARS-CoV-2 mRNA Vaccine. NEJM 384: 1372-1374.
-
Mathioudakis AG, Ghrew M, Ustianowski A, Ahmad S, Borrow R, et al. (2021) Self-Reported Real-World Safety and Reactogenicity of COVID-19 Vaccines: A Vaccine Recipient Survey. Life 11(3): 249.
-
Lydia H, Delgado P, Romero Pinedo S, Quesada M, Balabanov I, et al. (2021) Decreased Breadth Of The Antibody Response To The Spike Protein Of Sars-Cov-2 After Vaccination. medRxiv.
-
Neidleman J (2021) mRNA vaccine-induced T cells respond identically to SARS-CoV-2 variants of concern but differ in longevity and homing properties depending on prior infection status. bioRxiv.
-
Föhse FK (2021) The BNT162b2 mRNA vaccine against SARS-CoV-2 reprograms both adaptive and innate immune responses.
- Are the Vaccines the Only Solution to Prevent the COVID-19 Pandemic? Part Two
- Clinical Characteristics of Women in this New Global Immunodeficiency
- Cell Dynamics in HIV Pathogenesis: Insights and Implications
- Determination of the CDR (CDR1, CDR2) « Complementary- Determining Region Invertebrate Primitive Antibody from Sea Star »
- Prioritizing Care for High-Risk COVID-19 Patients in the EU: 10 Civic Recommendations to the Institutions
- Comprehensive Insights into ModRNA Vaccines: Persistent PP-Spike Recombinant Protein, Hyperimmune/Inflammatory Reactions, Thrombotic Vasculopathy, Chronic Organ Complications and Excess Deaths