The Effect of Footwear on Postural Sway in Community Dwelling Older Adults
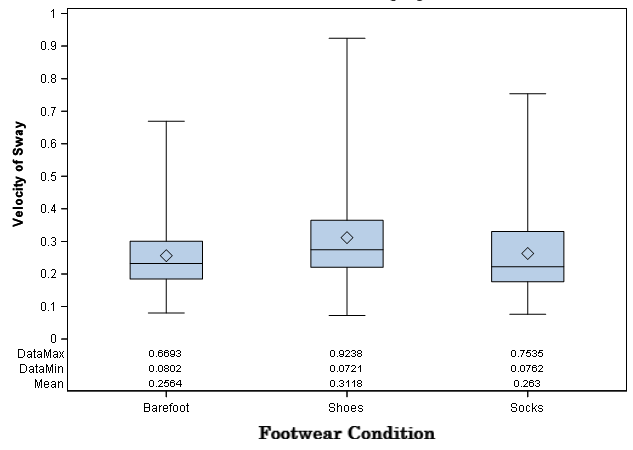
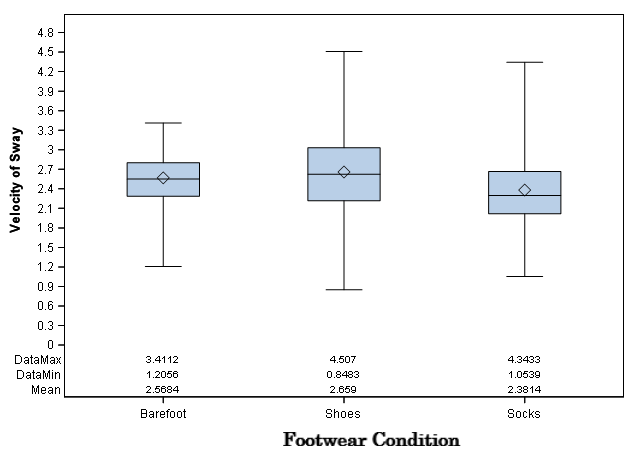
Background and Purpose: Non-slip socks are frequently used in health care settings in an attempt to reduce falls. Increased velocity of postural sway has been shown to relate to increased risk of falling. The influence of footwear on velocity of postural sway has yet to be determined. The purpose of this study was to compare the velocity of postural sway of community-dwelling older adults during a simulated fall while barefoot, wearing athletic type shoes, or wearing non-slip socks. Methods: Postural sway was measured during a simulated fall on 27 ambulatory adults with an average age of 58.07 years using computerized posturography. Subjects underwent three simulated falls in each footwear condition (barefoot, shoes, non-slip socks). Thirteen of the 27 subjects completed a post-study survey to subjectively rank the stability of each footwear condition. Hierarchical linear modeling statistics determined the difference in velocity of sway wearing different types of randomly applied footwear with P≤.05. Results and Discussion: In static standing, the mean velocity of postural sway for barefoot and non-slip socks was 0.26 m/s, athletic shoes was 0.31 m/s; barefoot and non-slip socks demonstrated lower velocity of sway at p-value of P<0.05 when compared to athletic shoes. In dynamic standing during the simulated fall, the mean velocity of postural sway for barefoot was 2.57m/s, athletic shoes was 2.66m/s and non-slip socks was 2.38m/s. Non-slip socks demonstrated lowest velocity of sway at p-value of P<0.001 when compared to athletic shoes. Post-study survey analysis revealed a p-value of 1.000. The p-value of 1.000 for the post study surveys concludes that the subjective rank of the most stable footwear condition did not match objective data. This indicates subjects were unable to subjectively determine which footwear most reduced postural sway. Conclusions: Non-slip socks may be effective at reducing the velocity of postural sway in community-dwelling older adults and may be effective at reducing fall risk
Introduction
There is limited information on the effectiveness of non-slip socks with regards to their ability to reduce falls. It has been determined that footwear characteristics impact balance, but how this is directly related to the rate and risk of falls is unclear [1]. Falls are a devastating health concern in the older adult population. One in 3 community living older adults over the age of 65 who have had at least one fall in a year and 20-30% of people who fall suffer moderate to severe injuries [2]. Injuries that arise from a fall are responsible for increased mortality and morbidity in this population. Velocity of sway involves movement of a person’s center of gravity and is a major factor that contributes to falls leading to increased morbidity and mortality rates. The velocity of sway is defined as the speed at which postural movements are made by an individual in order to maintain a balanced position. It can be measured by the speed of the displacement over the center of mass relative to the base of support over time. Velocity of sway directly impacts balance; therefore, it can be assumed that velocity of sway will affect fall risk due to the fact that decreased balance is correlated with an increased risk of falls [3, 4]. Studies have shown that increased postural sway leads to a higher fall risk; therefore, further demonstrating the assumption that velocity of sway will affect the balance and fall risk [5]. While there is ample information to define falls, and contributing factors to higher fall risk, there is little research that shows the impact that footwear has on balance. Retrospective studies have looked at the type of footwear worn during a fall; results showed that wearing standard socks and being barefoot increases risk of falls where athletic shoes decreases risk of falls [6]. This was additionally supported by a study that showed an altered gait pattern while ambulating in socks [7]. The purpose of non-slip socks, commonly used in many medical settings, are to decrease the risk of falls.
However, there is insufficient evidence as to demonstrate that non-slip socks are actually effective in preventing falls. Problem Statement There is a lack of evidence to support whether or not non-slip socks prevent falls; however, the protocol of many medical settings is to provide all patients, including those who are considered a high fall risk, non-slip socks, despite the lack of evidence to support this decision.
Purpose
The purpose of this study is to determine the velocity of postural sway that the older adult experiences during a simulated fall while wearing footwear designed to reduce falls (non-slip socks) versus while being barefoot or wearing athletic shoes.
Significance of Problem
Falls are a devastating health concern in the older adult population. By determining the velocity of postural sway that occurs while wearing different footwear during a simulated fall, it may be possible to determine the safest footwear option for patients to wear in health care settings to decrease falls.
Review of Literature
Existing literature confirms that falls are correlated to negative outcomes such as injury, mortality, and psychological damage [8, 9, 10]. The use of non-slip socks for the prevention of falls in healthcare facilities has become protocol, despite the lack of evidence to support the use of this footwear. A literature review revealed four studies that investigated the correlation between footwear and risk of falls [1, 6, 11, 12]. Only two of those studies looked specifically at the use of non-slip socks to prevent falls [11, 12]. Chari concluded that an individual has more slip-resistance while being barefoot on an inclined ramp compared to while wearing non-slip socks. This was determined by a sensor that detected the angle at which slippage occurs [11]. In contrast, Hubscher found that wearing non-slip socks was comparable to being barefoot and was better than conventional socks when looking at heel deceleration time using a 1-directional accelerometer to detect slip distance [12].
A double-blind study by Fernie looked at the relationship between postural sway and incidence of falls in an institutionalized geriatric population. The results showed that incidence of falls was significantly higher for individuals who had reported one or more falls during the previous year compared to those without a reported fall [5]. A study by Baczkowicz investigated postural sway as measured by dynamic computerized posturography using the NeuroCom® Balance Master platform and found it was effective in predicting fall risk when compared to the Berg Balance test in combination with a patient’s self- reported history of falls [13]. The Berg Balance test is a 14-point objective measure designed to assess static balance and fall risk in adult populations with known measures of validity and reliability [14]. The Baczkowicz study found that postural sway had significant relation to the Berg and significant relation to the number of self- reported falls [13].
The NeuroCom® Balance Master Platform provides dynamic computerized posturography and can measure the velocity of postural sway. The following studies provide information regarding the measures of reliability and validity in postural sway and with dynamic posturography.
A systematic review concluded that the test-retest reliability for mean velocity when measuring the center of pressure using a bipedal static center of pressure measurement tool varied ranging from .32-.94. Averaging results from 3-5 trials increased the reliability. Researchers concluded that center of pressure measurements can be considered a reliable tool to assess postural stability [15].
A systematic review concluded that the test-retest reliability for mean velocity when measuring the center of pressure using a bipedal static center of pressure measurement tool varied ranging from .32-.94. Averaging results from 3-5 trials increased the reliability. Researchers concluded that center of pressure measurements can be considered a reliable tool to assess postural stability [15]. 1. Force plates demonstrated reproducible measures within .5 degrees, with 24-hour test-retest reliability at (.52-.96) [16]. 2. A research study used the NeuroCom® Smart Balance Master computerized posturography to investigate the relationship between postural control and ability to complete functional tasks. They concluded that postural control has a significant correlation with a person’s ability to cross streets, climb stairs, and exit a car [16]. 3. Another study found that reactive voluntary postural sway is a strong determinant of fall risk for healthy community dwelling older adults in a study that used center of pressure measurements to assess postural sway [17].
The devastating effects of falls on the older adult population makes fall prevention a necessary endeavor. Non-slip socks have been assumed to prevent falls in healthcare facilities without adequate evidence to support their use. Postural sway has been reported to significantly increase with increased incidence of falls. The literature indicates that use of the NeuroCom® Balance Master Platform dynamic computerized posturography is effective in detecting postural sway and risk of falls. Therefore, the NeuroCom® was used in this study to determine the differences in postural sway during a simulated fall in healthy older adults while wearing non- slip socks, athletic shoes, and while barefoot.
Methods
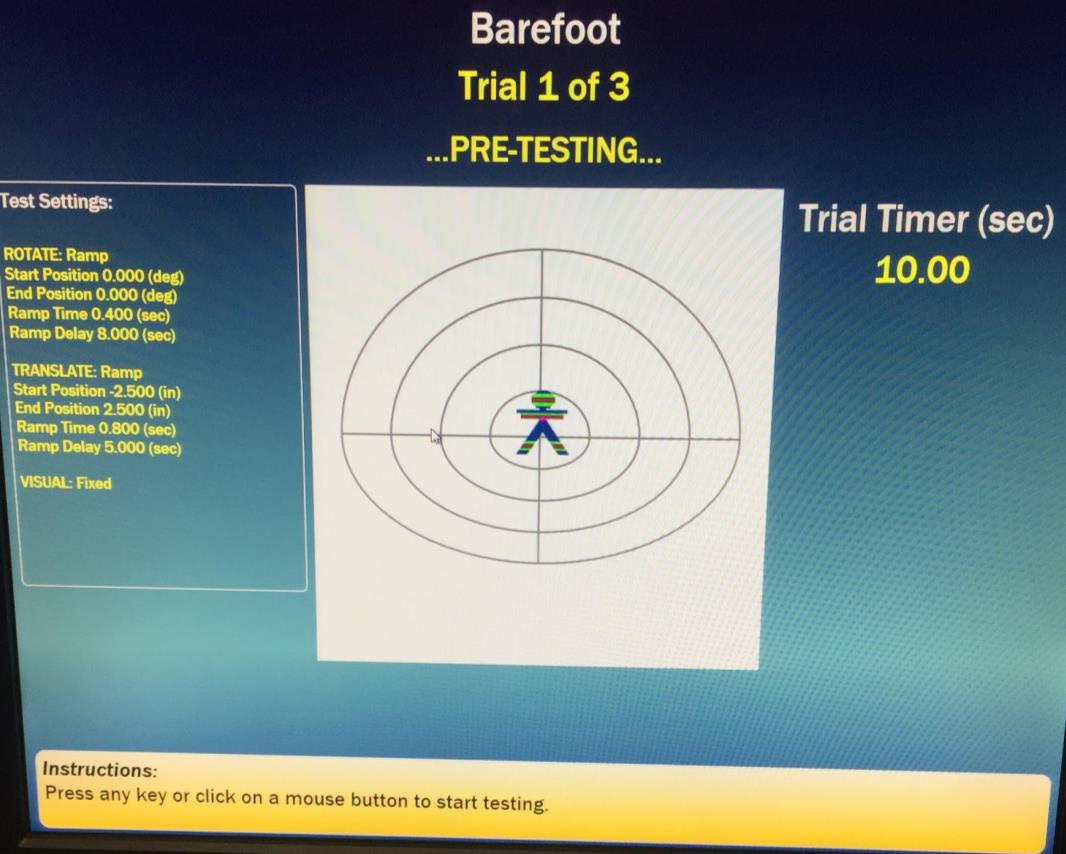
This study was designed to mitigate risk while finding an efficient and effective way to measure velocity of postural sway during a simulated fall while barefoot, while wearing non-slip socks and while wearing athletic shoes. Subjects were recruited using a sample of convenience through local connections and flyers. The subjects agreed to the mild risks of being harnessed while standing on the NeuroCom platform during a simulated a fall. Risk was minimized by asking the subjects to wear comfortable pants for testing and by securing the harness in the appropriate manner.
Each subject served as their own control in this study allowing for a repeated measures design for data analysis. The advantage of this design is that individual differences between participants were removed as a potential confounding variable. Also, the repeated measures design required fewer participants, since data for all conditions was derived from the same group of participants.
Study Site and Subjects
All research data collection took place at Grand Valley State University. The NeuroCom is a stationary machine and required testing in the Biomechanics and Motor Performance Laboratory at Grand Valley State University.
Inclusion criteria for this study included adults age 50 and older who were able to walk independently in the community without assistive devices. All participants were asked to wear closed athletic type shoes of their choice.
Subjects were excluded if they were unable to pass a cognitive screen. This was determined by the St. Louis University Mental Status (SLUMS) exam with a minimum score of 25/30. The SLUMS is a 30-point, 11 question screening questionnaire that tests orientation, memory, attention, and executive function and has known measures of validity and reliability [18]. Also excluded were any subjects with neurologic diagnoses including cerebral vascular accident, Multiple Sclerosis, and Parkinson disease, severe arthritis or musculoskeletal injury within the past year including fracture, ligament tears, and severe muscle sprains. Other exclusions included uncontrolled hypertension or active uncontrolled cardiac disease in the past year and/or blood pressure reading above 140/90 mmHg or below 90/60 mmHg at time of testing, known sensory deficits, weight exceeding 450 lbs., blindness and inability to understand or speak English. Non-English speakers were exempt from this study because it was designed to be representative of the recruiting area and demographic; there are limited non-English speakers in the area where the study was conducted. The study protocol was reviewed and accepted by the Human Research Review Committee at Grand Valley State University.
Population
The target population included healthy older adults age 50 and above who meet the study criteria. The participation pool was a sample of convenience (See Table 1 for participant demographics). Subjects were recruited via flyers and word of mouth from Grand Valley State University. A power analysis was performed indicating the need for 12-28 subjects to achieve statistically significant results with the alpha level at P≤.05. The literature review determined that frail, older adults are at the highest risk for falls and have the most negative outcomes following a fall. Given that information, the ideal population would be frail, older adults; however, given the significant barriers to studying this population, this study focused on healthy, older adults to get an initial baseline for velocity of postural sway while wearing non- slip socks, athletic shoes, and while barefoot.
| Min | Max | Mean | SD | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age (years) | 50 | 89 | 58.07 | 8.76 | ||||||||
| Height (cm) | 52.4 | 195.58 | 172.07 | 12.4 |
Table 1: Participant Demographics.
Equipment and Instruments
- Blood pressure cuff: Standard procedure was used to take blood pressure of each subject using a manual blood pressure cuff. This information was used to determine if blood pressure was within exclusion criteria and to exclude participants with high or low blood pressure.
- Stethoscope: Used in conjunction with blood pressure cuff to obtain blood pressure measurements.
- Tape measure: Flexible tape measure that measures lengths up to 7’ to collect heights of participants utilizing cm measurement scale.
- NeuroCom Balance Master Platform: This computerized posturography unit was used measure velocity of sway for participants during backward perturbations created by the force plate.
- SLUMS: Printed handout of test was utilized to determine if participants meet cognitive exclusion criteria.
- Health Intake Form: A written document was created by researchers to gather information needed to determine if participants meet inclusion and exclusion criteria. Participants were given the form and asked to complete this form with assistance for interpretation of the form made available as needed.
- Excel-Data collected by NeuroCom Balance Platform software system was uploaded to excel without patient identifiers.
The formula ABS(FP.COGy(1)- FP.COGy(0))/0.01sec was used to create 9 data points indicating average velocity of sway of the Center of Gravity (COG) for each of the 3 trials under each of the 3 conditions (ABS = absolute value, FP.COGy(
Procedures
All data collection was performed by the NeuroCom software. The data was then transferred to Excel where the results were inputted into a formula to determine velocity of postural sway in degrees per second using a specific formula as explained in the data analysis section.
Subjects were initially screened via a telephone script, then asked to schedule a time to undergo further screening at the data collection site. Researchers verified that each subject was able to walk independently without an assistive device. Subjects were required to sign a written informed consent form. Subjects then had their height measured and were asked to complete health history intake forms with self-reported weight. Blood pressure and heart rate were taken. They were then asked to complete the Saint Louis University Mental Status (SLUMS) exam. With this information, it was determined if the subject was appropriate to continue with the study. If so, the participant was then assisted into the NeuroCom harness and asked to stand on the force platform. The participant’s feet were placed and the harness adjusted following the procedural standards found in the NeuroCom equipment manual. A pre- determined script was used during testing to maintain consistency of verbal cues. The subject experienced a simulated perturbation on the NeuroCom. While the subject was standing on the force platform, the platform slowly moved backward. Then, once the testing began, the platform moved quickly forwards simulating a slip on a level surface. This was repeated 3 times in each type of footwear. The subject was securely in the harness during all of the testing and was additionally guarded by another person standing close-by who could quickly unharness the subject and/or help them re-balance if the subject needed assistance while in the harness. The participant was given standard 2-minute rest break after each footwear condition with the option to take rest breaks or stop at any time. All subjects were asked how they were feeling and if they wished to continue after each trial. After the Neurocom® trials, 13 of the 26 subjects were asked to complete a validated survey to rank how stable they felt under each condition; one being most stable to three being least stable. The order of the footwear listed on the survey was randomized for each participant to eliminate bias. Participant’s subjective ranking of stability during the three footwear conditions was then later compared to the objective information from the NeuroCom® to determine the level of agreement. The survey was not administered to all subjects because it was added after the 12th subject was tested. This time was needed to complete survey validation.
Data was analyzed by the Grand Valley State University Statistical Consulting Center. Velocity of Postural Sway data was processed in SAS Version 9.4
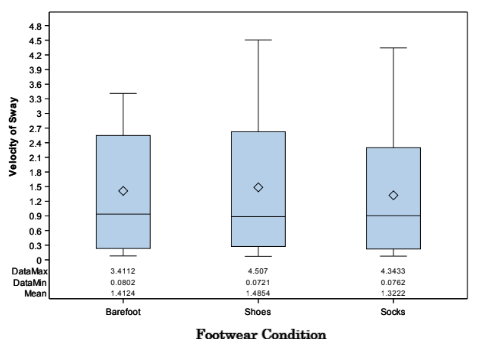
and non-slip socks were found to be statistically different (p < 0.05) with a lower average velocity of postural sway (Table 2). With non-slip socks as the reference condition, barefoot was not statistically different in terms of velocity of postural sway during static standing (Table 3). For dynamic standing (when the platform simulated the fall) with shoes as the reference, non-slip socks were found to be significantly different (p < 0.001) with a lower velocity of postural sway (Table 5). Barefoot was not found to be significantly different than shoes during dynamic standing (Table 6). For the combined data with shoes as the reference neither barefoot nor non-slip socks were determined to be significantly different in terms of velocity of sway during dynamic standing (Table 8). For combined data with non-slip socks as the reference neither barefoot or shoes were determined to be significantly different in terms of velocity of sway (Table 9). Results from the Generalized McNemar’s test had a p- value of 1.000. Figure2,3,4
- Data was collected from 26 participants ranging from
- 51 to 89 of age with a mean of 58.07 years. There were 16 females and 10 males included. For static standing with athletic shoes as the reference condition, both barefoot
- Condition
- N Minimum Lower
- Quartile MaximumMean Std DEV Lower 90%
- N= total number of trials for all 27 participants (27 participants X 3 trials = 81)
- Condtion
- Estimate
- Std Error
- DF t-value
- Pr > I t I
- Alpha
- Lower
- Upper
- Barefoot
- -0.05529
- 0.01769
- 160
- -3.13
- 0.0021
- 0.05
- -0.09032
- -0.02046
- Socks
- -0.04876
- 0.01769
- 160
- -2.76
- 0.0065
- 0.05
- -0.08369
- -0.01383
- Shoes
- 0
- -
- -
- -
- -
- -
- -
- -
- Condition N Minimum
- Lower
- Quartile Median Upper
- Quartile Maximum Mean Std DEV Lower 95% of
- Variation
- Barefoot 81
- 1.21
- 2.29
- 2.55
- 2.8
- 3.41
- 2.57
- 0.41
- 2.48
- 2.66
- 15.95
- Shoes
- 81
- 0.85
- 2.22
- 2.62
- 3.03
- 4.51
- 2.66
- 0.67
- 2.51
- 2.81
- 25.2
- Socks
- 81
- 1.05
- 2.02
- 2.3
- 2.67
- 4.34
- 2.38
- 0.51
- 2.26
- 2.5
- 22.29
Table 2: Dynamic Standing.
| Condition | Estimate | Std Error | DF | t-value | Pr > t | Alpha | Lower | Upper | |||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Barefoot | -0.00663 | 0.01455 | 160 | - | 0.37 | 0.7082 | 0.05 | -0.042 | 0.0283 | ||||||||||||||||||||||||||||||||||
| Shoes | 0.04876 | 0.01769 | 160 | 2.76 | 0.0065 | 0.05 | 0.0138 | 0.0837 | |||||||||||||||||||||||||||||||||||
| Socks | 0 | - | - | - | - | - | - | - |
Table 4: Dynamic Standing. N= total number of trials for all 27 participants (27 participants X 3 trials = 81)
| Condition | N | Minimum | Lower Quartile | Median | Upper Quartile | Maximum | Mean | Std DEV | Lower 90% CL for Mean | Upper 95% CL for Mean | Coefficient of Variation |
Table 3: Dynamic Standing with Non-slip Socks as Reference.
- Condition
- Estimate
- Std Error
- DF t-value
- Pr > I t I
- Alpha
- Lower
- Upper
- Barefoot
- -0.0906
- 0.07546
- 160
- -1.2
- 0.2318
- 0.05
- -0.2396
- 0.05845
- Socks
- -0.2776
- 0.07546
- 160
- -3.68
- 0.0003
- 0.05
- -0.4267
- -0.1286
- Shoes
- 0
- -
- -
- -
- -
- -
- -
- -
Table 5: Dynamic Standing with Shoes as Reference.
Condition Estimate Std Error DF t-value Pr > I t I Alpha Lower Upper Barefoot 0.187 0.07546 160 2.48 0.0142 0.05 0.038 0.3361 Shoes 0.2776 0.07546 160 3.68 0.0003 0.05 0.1268 0.4267 Socks 0 - - - - - - - Table 7: Dynamic Standing with Non-slip Socks as Reference.
| Median e | Coefficien of n Variation | t | ||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Q | Lower | Upper Quartile | Lower 95% CL for Mean | Upper 95% CL for Mea | ||||||||||||||||||||||||
| Condition | N M | inimum | Maximu | m | Mea | n | St | d DEV | ||||||||||||||||||||
| uartil | ||||||||||||||||||||||||||||
| Barefoot | 162 | 0.0 | 8 | 0.23 | 0.94 | 2.55 | 3.41 | 1.41 | 1.2 | 1.2 | 3 | 1.6 | 84.8 | |||||||||||||||
| Shoes | 162 | 0.0 | 7 | 0.27 | 0.89 | 2.62 | 4.51 | 1.49 | 1.27 | 1.2 | 9 | 1.68 | 85.7 | |||||||||||||||
| Socks | 162 | 0.0 | 8 | 0.22 | 0.9 | 2.3 | 4.34 | 1.32 | 1.13 | 1.1 | 5 | 1.5 | 8 | 5.47 |
Table 6: Combined Data (static and dynamic standing). N= total number of trials for all 27 participants (27 participants X 6 tria
Table 8: Combined Data (static and dynamic standing). N= total number of trials for all 27 participants (27 participants X 6 trials = 162) Condition Estimate Std Error DF t-value Pr > I t I Alpha Lower Upper Barefoot -0.07299 0.09441 160 -0.55 0.5854 0.05 -0.337 0.1907 Socks -0.1632 0.1335 160 -1.22 0.2234 0.05 -0.427 0.1005 Shoes 0 - - - - - - - Table 9: Combined Data with Shoes as Reference.
| Condition | Estimate | Std Error D | F t-value | Pr > I t I | Alpha | Lower | Upper | |||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Barefoo | t | 0.0902 | 0.133 | 5 1 | 60 0. | 68 | 0 | .500 | 3 | 0 | .05 | -0.1735 | 0 | .3539 | ||||||||||||||||
| Shoes | 0.1632 | 0.133 | 5 1 | 60 1. | 22 | 0 | .223 | 4 | 0 | .05 | -0.1005 | 0 | .4269 | |||||||||||||||||
| Socks | 0 | - | - | - | - | - | - | - |
Table 7: Combined Data with Socks as Reference
| Survey Ranking | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Objective Ranking | 1 | 2 | 3 | Total | ||||||||||||||||
| 1 | 3 ( | 23.08 | ) | 5 (38.46 | ) | 5 | (38.46) | 13 | ||||||||||||
| 2 | 5 ( | 38.46 | ) | 4 (30.77 | ) | 4 | (30.77) | 13 | ||||||||||||
| 3 | 5 ( | 38.46 | ) | 4 (30.77 | ) | 4 | (30.77) | 13 | ||||||||||||
| Total: | 13 | 13 | 13 | 39 |
Table 8: Combined Data with Socks as Reference
Table: 11
| Test Symmetry | ||||||||
|---|---|---|---|---|---|---|---|---|
| Statistic (S) | 0 | |||||||
| DF | 3 | |||||||
| Pr > | S | 1 |
Table 9: Combined Data with Socks as Reference
Table 11-13: Generalized McNemar’s Test Output.
| Kappa Statistics | ||||||
|---|---|---|---|---|---|---|
| Value | ASE | 95% Confidence Limit | s | |||
| Simple Kappa | -0.0769 | 0.1081 | 0.1 | 349 | ||
| Weighted Kappa | -0.0962 | -0.335 | 0.1 | 426 |
Table 10: Combined Data with Socks as Reference
Table: 13
Discussion
The purpose of this study was to determine the velocity of postural sway that older adults experience during a simulated fall while wearing footwear designed to reduce falls (non-slip socks) versus while being barefoot and wearing athletic shoes. By comparing these different types of footwear commonly worn in medical settings we hoped to reinforce or advise against the use of non-slip socks as a method of reducing falls. In this study, there was statistically lower velocity of postural sway while wearing socks as compared to shoes. These statistically significant differences in velocity of postural sway demonstrate that non-slip socks may lower the velocity of postural sway thereby reducing fall risk in populations over the age of 50 when encountering a simulated posterior perturbation.
Limitations
There are certain limitations in this study. First, the authors wish to acknowledge that the portions of the literature review and methods were previously published in a pilot study entitled “The Effects of Footwear on Postural Sway: A Pilot Study” [19]. Additionally, this study has a small sample size of healthy older adults over the age of 50 so should not be generalized to the population of health older adults over 50 years of age. Also, measurements were made without blinding of the researcher to the experimental group, which has the potential for bias. This potential bias was minimized by random assignment of footwear for participants and by following of a standardized protocol. The potential for a learning effect was also minimized through the use of randomization of condition assignment and methods of statistical analysis which accounted for this possibility. There was no attempt to control the type of athletic footwear worn by subjects. Certainly, brand new shoes may have a different coefficient of friction than shoes previously worn. Unlike the athletic shoes, every participant wore the Posey® non-slip socks for the study. However, not all non-slip hospital socks are made with identical pattern and level of friction and may not have given us the same results as the Posey® non-slip socks. Another factor that may have impacted results is that lack of a practice trial on the Neurocom® before data collection started. Incorporating a practice trial could have helped mitigate a learning effect that participants may have experienced during the participant’s first condition. This study tried to decrease the impact of a learning effect by randomizing the order of the footwear conditions, but regardless of the order of conditions there may have been a learning effect. For each trial of the study, the perturbation by the NeuroCom® occurred at five seconds. Participants watched the screen in front of them to monitor their center of mass which also displayed a trial timer. This could have allowed patients to anticipate and alter their postural set prior to the perturbation at five seconds. One participant commented on the predictability of the perturbation due to the visibility of the trial timer. Another limitation of this is study is the age of participants. The mean age was 58.07. This is on the low end of the target age range which limits the generalizability of the results. Finally, this study lacks a control group or healthy young adult population comparison which limits the ability to generalize and apply the results to a more universal population.
Conclusions
The findings of this study indicate that non-slip socks decrease velocity of sway in a simulated fall in healthy ambulatory older adults over 50 years of age and may help prevent falls in this population. Balance decline and increased fall risk are significant health concerns in the geriatric population. Further research should be done to investigate different brands of non-slip socks and to look at the effect of footwear on velocity of postural sway while ambulating.
References
-
Menz HB, Morris ME, Lord SR (2006) Footwear characteristics and risk of indoor and outdoor falls in older people. Gerontology 52(3): 174-180.
-
Stevens JA, Ballesteros MF, Mack KA, Rudd RA, DeCaro E, et al. (2012) Gender differences in seeking care for falls in the aged medicare population. Am J Prev Med 43(1): 59-62.
-
Doheny EP, McGrath D, Greene BR, Walsh L, McKeown D, et al. (2012) Displacement of centre of mass during quiet standing assessed using accelerometry in older fallers and non-fallers. In: Conf Proc IEEE Eng Med Biol Soc 2012: 3300-3303.
-
Baczkowicz D, Szczegielniak J, Proszkowiec M (2008) Relations between postural stability, gait and falls in elderly persons--preliminary report. Ortop Traumatol Rehabil 10(5): 478-485.
-
Fernie GR, Gryfe CI, Holliday PJ, Llewellyn A (1982) The relationship of postural sway in standing to the incidence of falls in geriatric subjects. Age Ageing 11(1): 11-16.
-
Koepsell TD, Wolf ME, Buchner DM (2004) Footwear style and risk of falls in older adults. J Am Geriatr Soc 52(9): 1495-1501.
-
Tsai YJ, Lin SI (2013) Older adults adopted more cautious gait patterns when walking in socks than barefoot. Gait Posture 37(1): 88-92.
-
Rubenstein LZ (2006) Falls in older people: Epidemiology, risk factors and strategies for prevention. Age and Ageing 35(2): 37-41.
-
WHO (2007) WHO Global Report on Falls Prevention in Older Age.
-
Li F, Fisher KJ, Harmer P, McAuley E, Wilson NL, et al. (2003) Fear of falling in elderly persons: association with falls, functional ability, and quality of life. J Gerontol B Psychol Sci Soc Sci 58(5): 283-290.
-
Chari S, Haines T, Varghese P (2009) Are Non-Slip Socks Really “Non-Slip”? An Analysis of Slip Resistance BMC Geriatr 9: 39.
-
Hubscher M, Thiel C, Schmidt J, Bach M, Banzer W, et al. (2011) Slip resistance of non-slip socks - An accelerometer-based approach. Gait Posture 33(4): 740-742.
-
Baczkowicz D, Szczegielniak J, Proszkowiec M (2008) Relations between postural stability, gait and falls in elderly persons--preliminary report. Ortop Traumatol Rehabil 10(5): 478-485.
-
Berg KO, Maki BE, Williams JI, Holliday PJ, Wood- Dauphinee SL, et al. (1992) Clinical and laboratory measures of postural balance in an elderly population. Arch Phys Med Rehabil 73(11) 1073- 1080.
-
Ruhe A, Fejer R, Walker B (2010) The test-retest reliability of centre of pressure measures in bipedal static task conditions --a systematic review of the literature. Gait Posture 32(4): 436-445.
-
Topp R, Mikesky A, Thompson K(1998) Determinants of four functional tasks among older adults: an exploratory regression analysis. J Orthop Sports Phys Ther. 27(2): 144-153.
-
Tucker MG, Kavanagh JJ, Morrison S, Barrett RS (2010) What Are the Relations Between Voluntary Postural Sway Measures and Falls-History Status in Community-Dwelling Older Adults? Arch Phys Med Rehabil 91(5): 750-758.
-
Feliciano L, Horning SM, Klebe KJ, Anderson SL, Cornwell RE, et al. (2013) Utility of the SLUMS as a cognitive screening tool among a nonveteran sample of older adults. Am J Geriatr Psychiatry 21(7): 623- 630.
-
Goehring M, Bringer N, Broders J, Young E (2018) The Effects of Footwear on Postural Sway: A Pilot Study. Physical & Occupational Therapy in Geriatrics 36(2- 3).
- Electrolyte Considerations for Athletes
- Comprehensive Rehabilitation in Adults with Diabetic Peripheral Neuropathy: A Literature Review on Frequency, Intensity, and Duration Parameters
- Exercise Duration and Its Association with ADHD Symptom Severity in Children and Adolescents: A Parent-Reported Survey Study
- Adaptation of the Adult Neurophysiology of Pain Questionnaire for Use in Pediatrics
- A Non-Pharmacological Multidisciplinary Pain Program within a Hospital Wellness Program: A Mixed Methods Study
- The Effect of Frenkel's Exercise with PNF on Functional Reach in Stroke Survivors: A Randomized Control Trial