Attitudes, Beliefs and Behaviors Regarding Marijuana Use among Occupational Therapists in the United States
Background/Objective: Legalization of marijuana for medical and/or recreational purposes has spurred significant debate among health care professionals in the United States, though research on their opinions and usage is limited. The purpose of this study was to survey one specific health care grouping, occupational therapists, and examine their attitudes, beliefs, and behaviors specific to marijuana use. Methods: Following IRB approval, a national random sample of 500 occupational therapists were postal mailed survey packets which included a cover letter and a multi-page questionnaire. Results: One hundred ninety-five surveys were returned. The majority reported marijuana use was legal in their state for medicinal but not for recreational purposes. Less than ten percent had ever used marijuana for medical reasons; however, two out of five reported they had used marijuana for recreational purposes, though typically not within the previous five years. Reasons for use included to get high and to be sociable. A majority agreed marijuana should be legalized in all states for medical purposes, but conceded this would lead to more people trying it and making it more accessible to minors. Discussion: Discussion addresses these results in relation to general population usage, national legalization trends, and reported health benefits and concerns.
Introduction
Cannabis, commonly referred to as marijuana, is currently the most frequently used illicit drug in the United States, [1] and the second most popular Attitudes, Beliefs and Behaviors Regarding Marijuana use among Occupational Therapists in the United States “substance” after alcohol. Marijuana is known to contain over 400 chemical entities, including an assortment of natural compounds known as phytocannabinoids most notably psychoactive delta-9-tetrahydrocannabinol (d-9- THC), the plant’s main psychoactive ingredient [2]. These compounds interact with at least two specific cannabinoid receptors found in the brain (principally in the basal ganglia and limbic system) and the immune system (with their greatest density in the spleen) to ultimately produce Ann Physiother Occup Ther
the recognized and desired physiological and psychological experiential effects [2, 3, 4]. Marijuana can be consumed in a variety of ways, including: inhalation through smoking or vaporizing (via joints, bongs, or glass pipes); ingested in edible or liquid form (mixed in food, tea, gum); topical (via lotions, oils); and, medicinally (through pills, suppositories, or transdermal patches).5 Results from a recent national survey on drug use and health indicate past year (2017) use of marijuana by residents of the United States (US) aged 18 and older was estimated at 15.3%, up from 14.1% the previous year (2016), a statistically significant increase [1]. Lifetime marijuana use, i.e., inclusion of all individuals who have tried marijuana at some point in their lives, was found to be just short of half the population at 45.2% [1]. Reasons for use include both recreational and medical purposes, with users typically reporting a general sense of euphoria and relaxation, as well as “heightened sensory perception (e.g., brighter colors), laughter, altered perception of time, and increased appetite” [5]. On the other hand, taking too much of the drug or using marijuana with a particularly high potency can potentially lead to a combination of unpleasant effects, including anxiety, fear, hallucinations, and/or paranoia [6].
At the time of this report, 33 states plus the District of Columbia (Washington, DC) have legalized marijuana for medical use purposes. The most frequently cited reason for medical marijuana use, including both prescribed and self-medicated usage, was to combat severe and chronic pain, along with more specific disorders such as arthritis, migraine, cancer, anxiety, sleep disorder/insomnia, spasticity, and mental health conditions [7, 8, 9, 10, 11]. On the other hand, ten states plus the District of Columbia have legalized marijuana for recreational purposes. Common reasons for recreational use include “to feel good/get high, to have a good time with friends, to experiment, and to relax” [12].
Currently, significant debate exists in the US regarding marijuana use [13, 14]. including medical use versus recreational usage, perceptions of marijuana as a “gateway drug”, the potential addictive nature of the drug, and problematic access to marijuana by minors. Moreover, marijuana remains classified through the Controlled Substances Act as a Federal Schedule I Drug connoting it has no accepted medical use and a high potential for abuse [15]. Recent national public opinion has witnessed a steadily growing increase in favor of declassification and overall legalization of the drug [16, 17], though favorable attitudes toward legalization of marijuana for medical purposes tend to be more pronounced than for recreational purposes[18, 19].
Irrespective of the public debate on marijuana use, research specific to attitudes, beliefs, and behaviors regarding marijuana use among health care professionals appears to be severely limited. While the majority of current research focuses on marijuana use by health care students [20, 21, 22, 23, 24], most research on marijuana use by health care professionals, eg., physicians, nurses, and pharmacists, is comparatively dated given recent and evolving trends toward its use [25, 26, 27, 28, 29, 30, 31, 32].
Occupational Therapy
Occupational therapy (OT) is a recognized health care profession with a unique foundation in mental health, designed to assist people in their recovery from a mental or physical impairment through the use of occupations as a form of rehabilitation. Moreover, OT “is the only profession that helps people across the lifespan to do the things they want and need to do through the therapeutic use of daily activities (occupations) … (and) enable people of all ages to live life to its fullest by helping them promote health, and prevent—or live better with—injury, illness, or disability” [33]. Occupational therapy has been identified by the Centers for Disease Control (CDC) as an appropriate treatment and intervention protocol for a variety of disorders, as well as an alternative treatment for dealing with chronic pain. Nevertheless, the CDC indicates more information is needed to determine if cannabis-based products are any better or worse than OT for treatment of chronic pain [34]. Consequently, it would appear to be relevant for occupational therapists to have some foundational knowledge of the physiological and psychological effects of cannabis in order to make argument as to the positive impact of OT over cannabis. In addition, given the drug’s recognized potential for problematic psycho-sensory effects, it would be incumbent upon OTs as mental healthcare professionals to be able to ascertain the differences between accurate accounts and facts versus erroneous myths of marijuana and marijuana usage. Finally, as with all healthcare professions, it is relevant and important for OT professional associations to know the extent of use of any such substance by its members.
While there has been some limited research on the attitudes and use of marijuana among occupational therapy students [20, 21], research on the topic of marijuana among practicing occupational therapists, including any examination of their beliefs and attitudes toward marijuana use or any assessment of likelihood of use by these health professionals, is essentially non- existent. The purpose of the present study, therefore, was to survey a national sample of occupational therapists in the US to ascertain their attitudes, beliefs, and behaviors specific to marijuana use.
Methods
Participants
The participants included 500 occupational therapists (OTs) randomly selected from membership in the American Occupational Therapy Association (AOTA) without regard to race, gender, or state of residence.
Instrument
The instrument was a self-designed three-page survey containing a series of initial “filter questions” querying whether or not they had ever used marijuana for medical purposes and/or for recreational purposes. If respondents indicated they had used the substance at some time in their life either for either purpose, they were questioned as to when they first tried marijuana, when they experienced their first “high”, and when they last used the substance. This was followed by a series of statements regarding possible reasons for their use of the substance, e.g., “for medical purposes”, “to relax”, “to forget my worries”, with each rated on a five-point scale ranging from “never” a reason to “always” a reason for using it. All participants, regardless of use, responded to a second series of statements targeting attitudes/beliefs regarding marijuana use in general, rated on five-point scales ranging from “strongly disagree” to “strongly agree”. Finally, all responded to a brief series of demographic questions, concerning age, gender, The median age of these occupational therapists (OTs) was 55 years (x 55. , sd . 0), ranging from to 5 years old. The majority of respondents were female (n = 191, 98.5%), as anticipated given the predominant percentage of females in the profession. Approximately one-half (n = 98. 50.5%) reported having a bachelor degree as their terminal occupational therapy degree, followed by master degree (n = 81, 41.8%), and doctorate (n = 15, 7.7%).
occupational therapy academic degree, and whether marijuana was legalized in their state of residence for medical and/or for recreational use.
Procedure
Following approval by the [REDACTED] Institutional Review Board, a list of 500 OTs’ names and addresses was obtained from the AOTA. All participants were postal mailed an identical survey packet which included a cover letter detailing the purpose of the study and how they had been selected as research participants, a copy of the survey questionnaire, and a postage paid return envelope. Follow-up postcards were sent to all participants as a thank-you to those who had completed and returned the survey, and to encourage those who had not done so to consider completing the survey.
Results
Of the 500 surveys mailed, a total of 195 (39%) were returned and included in the initial data analysis. Any discrepancy between this total number and that presented for any specific data analysis is in essence due to non-response by one or more participants for an item.
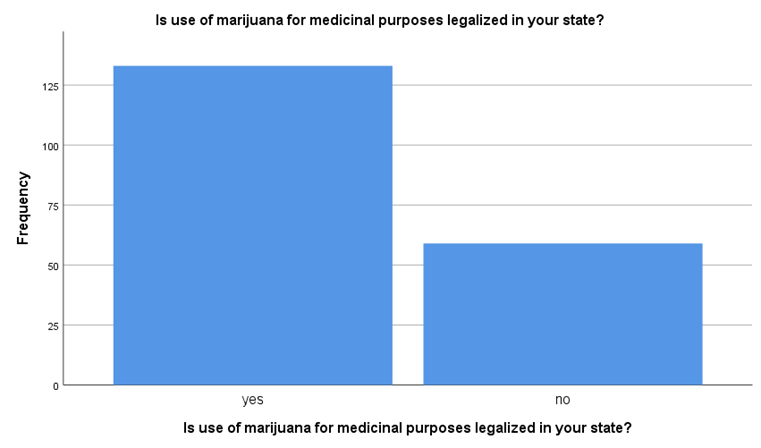
A comparison between those OTs with a bachelor degree (x = 55.46, sd = 9.42) versus those with a post- baccalaureate, i.e., those holding a master degree combined with those having a doctorate, (x = 56.32, sd = 9.11), found no significant difference in regard to mean age (t (191) = - 0.647, p = .518). The participants were asked if marijuana was legal in their state of residence for medical purposes, and if legal for recreational purposes.
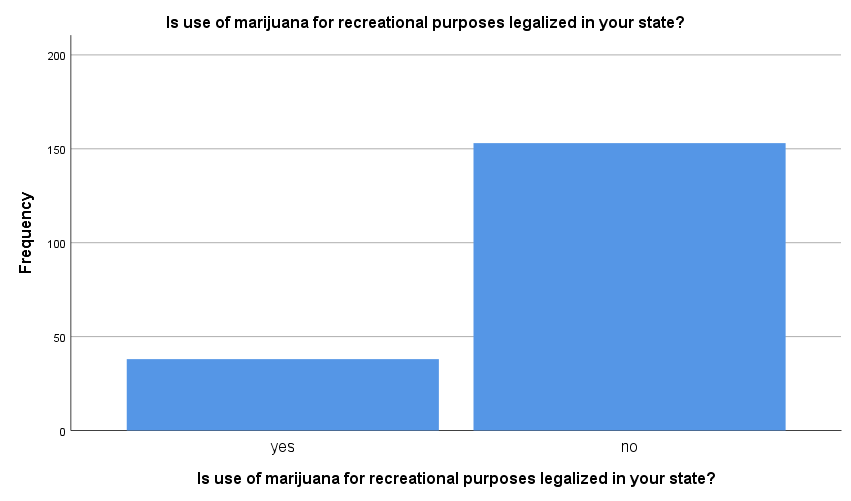
For most respondents (n = 133, 69.3%) marijuana was reported to be legal for medicinal purposes (X2 (1) = 52.521, p < .001). On the other hand, the majority (n = 153, 80.1%) reported that marijuana use was not legal in their state for recreational purposes (X2 (1) = 69.241, p < .001). These breakdowns are presented in Tables 1 & 2 below.
distinctions were found in regard to likelihood of use for medical purposes “and/or” use for recreational purposes, though the majority of participants were found to have used marijuana principally for recreational use alone (n = 71, 86.6%). This contrast is presented in Table 3 below.
| Have you ever used marijuana for recreational purposes? | ||||||||||||||
| Have you ever used marijuana for medical purposes? | ||||||||||||||
| Have you ever used marijuana for medical purposes? | ||||||||||||||
| Total | ||||||||||||||
| yes | no | |||||||||||||
| Have you ever used marijuana for | yes | 11 | 71 | 82 | ||||||||||
| recreational purposes? | no | 3 | 107 | 110 | ||||||||||
| Total | 14 | 178 | 192 |
Table 1: Comparison of likelihood of use of marijuana for medical “and/or” for recreational purposes (X2 (1) = 7.938, p = .005).
Less than ten percent of these OTs (n = 14, 7.2%) stated they had used marijuana for medical purposes (presented in Table 4 below), and had last done so within the past year (n = 8, 61.5%). All but one of these individuals resided in a state where marijuana was legal for medical use purposes. Frequency of use among this grouping varied from no longer using (n = 4, 28.6%), to using monthly or less (n = 5, 35.7), 2-4 times a month (n = 2, 14.3%), or up to 2-3 times a week (n =3, 21.4%).
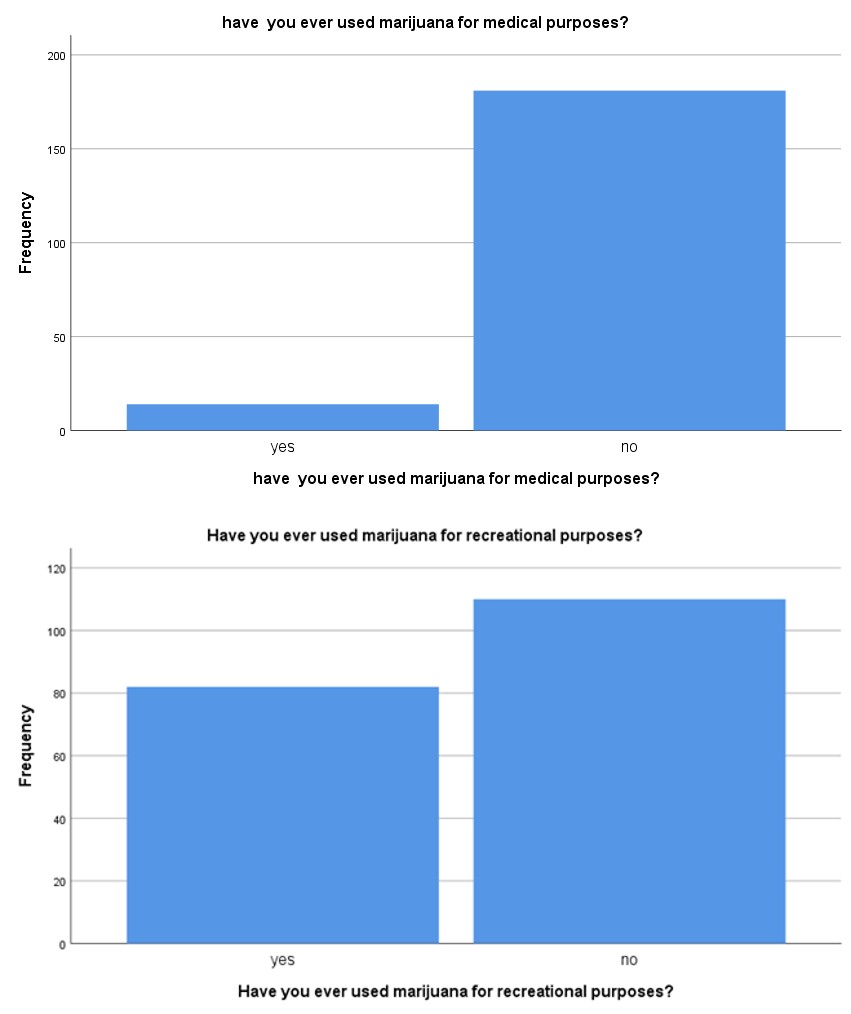
Conversely, a noteworthy percentage of respondents (n = 82, 42.7%) reported they had used marijuana at some time in their lives for recreational purposes, though the majority (n = 100, 57.3%) had not. This is presented in Table 5 below. For most users (n = 69, 86.3%), however, this was not anytime in the past five years, and more likely to have taken place over 20 years prior (n = 59. 73.8%), though a small percentage did indicate use in the recent past year (n = 6, 7.5%), or in the previous 1-5 years (n = 5, 6.3%). Interestingly, the majority of those OTs who used marijuana for medical purposes also admitted using it for recreational purposes (n = 11, 78.6%). Three-quarters (n = 60, 74.1%) of those who used marijuana for recreational purposes did so in a state where marijuana was legal for medical purposes, but not necessarily for recreational purposes.
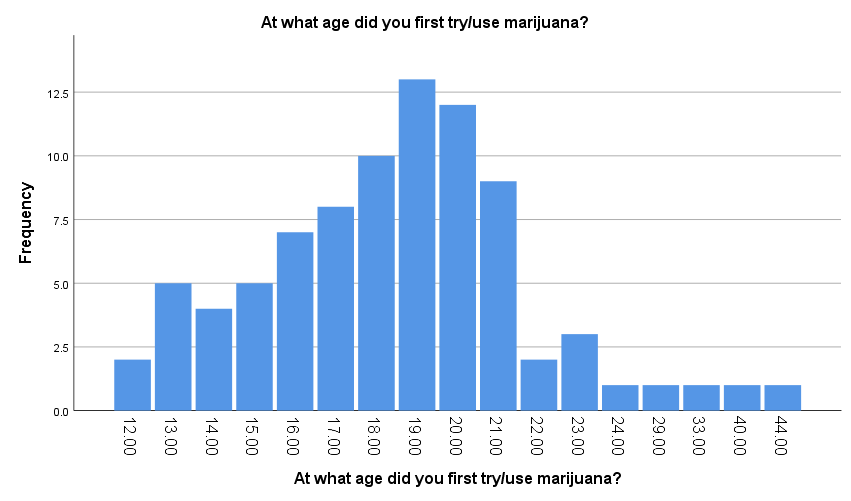
For those who did report using marijuana (n = 85) for either medical or recreational purposes, the median age of reported first use was years (x . , sd . ), varying from 12 to 44 years of age, though the majority (n = 59, 69.4%) reported they were between 16 and 21 years of age, followed by a significant decline of likelihood
- of first use after age 21. Mean age of experiencing first
- “high” mirrored age of first use (median years). A breakdown for year of first use is presented in Table 6 below.
Table 2: Age of first use of marijuana.
of users indicating “Frequently” and “Always”. Most likely reasons to use were: because it’s fun; to be sociable; to get a high; because it makes me feel good; and, to relax. Least likely reasons included: to stop me from feeling so hopeless; to turn off negative thoughts about myself; because it helps me when I’m feeling depressed; to help me feel more positive about things in my life; and, to forget painful memories. Frequency percentages for response categories for each of these reasons for use are presented in Table 7 below.
| Reason | N | I | O | A | F | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| For medicinal reasons | 83.8 | 6.3 | 6.3 | 2.5 | 1.3 | ||||||||||||
| To relax | 58.5 | 9.8 | 19.5 | 8.5 | 3.7 | ||||||||||||
| Because I like the feeling | 58.5 | 8.5 | 15.9 | 11 | 6.1 | ||||||||||||
| As a way to celebrate | 61.7 | 11.1 | 18.5 | 8.6 | 0.0 | ||||||||||||
| Because it is what most of my friends do when we get together | 62.5 | 8.8 | 17.5 | 10.0 | 1.3 | ||||||||||||
| To forget my worries | 81.3 | 11.3 | 5.0 | 1.3 | 1.3 | ||||||||||||
| Because it is exciting | 76.3 | 11.3 | 10. | 2.5 | 0.0 | ||||||||||||
| To be sociable | 53.8 | 10. | 16.3 | 16.3 | 3.8 | ||||||||||||
| Because I feel more self-confident or sure of myself | 86.3 | 8.8 | 2.5 | 2.5 | 0.0 | ||||||||||||
| To get a high | 56.3 | 7.5 | 17.5 | 15.0 | 3.8 | ||||||||||||
| Because it is something to do on special occasions | 76.3 | 8.8 | 10.0. | 5.0 | 0.0 | ||||||||||||
| Because it helps me when I am feeling nervous | 81.3 | 8.8 | 7.5 | 2.5 | 0.0 | ||||||||||||
| Because it is fun | 52.5 | 10.0 | 17.5 | 15.0 | 5.0 | ||||||||||||
| Because it makes a social gathering more enjoyable | 65.0 | 16.3 | 7.5 | 10.0 | 1.3 | ||||||||||||
| To cheer me up when I am in a bad mood | 87.5 | 5.0 | 5.0 | 2.5 | 0.0 |
Table 3: Frequency (%) responses for reasons for marijuana use.
| To be liked | 86.3 | 10.0 | 2.5 | 1.3 | 0.0 |
|---|---|---|---|---|---|
| To numb my (physical) pain | 87.5 | 3.8 | 6.3 | 2.5 | 0.0 |
| To numb my (personal/emotional) pain | 88.8 | 5.0 | 3.8 | 1.3 | 1.3 |
| Because it helps when I am feeling depressed | 88.8 | 8.8 | 2.5 | 0.0 | 0.0 |
| So that others won’t kid me about not using | 86.3 | 7.5 | 5.0 | 1.3 | 0.0 |
| To reduce my anxiety | 85.0 | 5.0 | 5.0 | 3.8 | 1.3 |
| To stop me from dwelling on things | 90.0 | 5.0 | 5.0 | 0.0 | 0.0 |
| To turn off negative thoughts about myself | 92.5 | 5.0 | 2.5 | 0.0 | 0.0 |
| To help me feel more positive about things in my life | 92.5 | 3.8 | 2.5 | 1.3 | 0.0 |
| To stop me from feeling so hopeless | 92.5 | 5.0 | 2.5 | 0.0 | 0.0 |
| Because my friends pressure me to use | 87.5 | 7.5 | 5.0 | 0.0 | 0.0 |
| To fit in with a group I like | 83.8 | 7.5 | 7.5 | 1.3 | 0.0 |
| Because it makes me feel good | 60.0 | 7.5 | 17.5 | 10.0 | 5.0 |
| To forget painful memories | 93.8 | 2.5 | 2.5 | 0.0 | 1.3 |
| So I won’t feel left out | 80.0 | 10.0 | 7.5 | 2.5 | 0.0 |
Table 4: Frequency (%) responses for reasons for marijuana use.
(N = Never; I = Infrequently; O = Occasionally; F = Frequently; A = Always) Table 7: Frequency (%) responses for reasons for marijuana use.
Finally, all participants, regardless of whether they have ever used marijuana or not were asked to indicate their degree of disagreement/agreement with a series of twelve statements regarding marijuana use. Responses were made on five-point scales ranging from: 1= strongly disagree, 2 = disagree, 3 = neutral, 4 = agree, 5 = strongly agree. Frequencies for each of these statements is
| Statement | SD | D | N | A | SA | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Marijuana should be legalized in all states for medicinal purposes. | 4.7 | 2.6 | 9.8 | 28.5 | 54.4 | ||||||||||||
| Marijuana should be legalized in all states for recreational purposes | 29.8 | 12.6 | 30.4 | 10.5 | 16.8 | ||||||||||||
| Marijuana is less harmful than alcohol. | 21.2 | 18.1 | 38.3 | 10.9 | 11.4 | ||||||||||||
| Marijuana use reduces motivation. | 2.6 | 10.9 | 40.1 | 33.3 | 13 | ||||||||||||
| Edible marijuana is safer than smoking marijuana. | 12.2 | 17 | 52.7 | 15.4 | 2.7 | ||||||||||||
| Legalizing recreational marijuana would make it readily accessible to minors | 8.3 | 20.7 | 18.1 | 33.7 | 19.2 | ||||||||||||
| Legalizing recreational marijuana would lead to more people trying it | 4.1 | 8.3 | 17.6 | 44 | 25.9 | ||||||||||||
| Marijuana is addictive. | 5.7 | 12.4 | 32.1 | 34.2 | 15.5 | ||||||||||||
| Marijuana is less harmful than tobacco. | 18.2 | 25 | 35.4 | 14.1 | 7.3 | ||||||||||||
| Marijuana has few if any side effects. | 16.1 | 41.7 | 28.1 | 13.5 | 0.5 | ||||||||||||
| Marijuana is damaging to the brain. | 4.2 | 9.9 | 37 | 36.5 | 12.5 | ||||||||||||
| Marijuana serves as a gateway drug to stronger drug use. | 8.3 | 17.6 | 32.1 | 25.9 | 16.1 |
Table 5: Frequency (%) responses toward statements regarding marijuana use.
| Item | Used | Never Used | ||||||
|---|---|---|---|---|---|---|---|---|
| Marijuana should be legalized in all states for medical purposes (t (189) = 2.754, p = .006); | 4.48 | 4.07 | ||||||
| Marijuana should be legalized in all states for recreational purposes (t (187) = 6.935, p < .001); | 3.44 | 2.14 | ||||||
| Marijuana is less harmful than alcohol (t (189) 6.528, p < .001); | 3.33 | 2.26 | ||||||
| Edible marijuana is safer than smoking marijuana (t (184) = 2.572, p = .011); | 2.99 | 2.63 | ||||||
| Legalizing marijuana would make it readily accessible to minors (t (189) = - 3.438, p = .001); | 3.02 | 3.62 | ||||||
| Marijuana is addictive (t (189) = - 3.807, p < .001); | 3.10 | 3.67 | ||||||
| Marijuana is less harmful than tobacco (t (188) = 2.826, p = .005); | 2.93 | 2.46 | ||||||
| Marijuana serves as a gateway drug to stronger drug use (t (189) = - 5.598, p < .001); | 2.75 | 3.64 |
Table 6: Mean tem responses between those who used marijuana (USED) and those who had never used (Never Used).
Several item statement ratings were found to be significantly related to agreement ratings for marijuana should be legalized for medical purposes. These included: marijuana should be legalized for recreational purposes (r (191) = .523, p < .001); marijuana is less harmful than alcohol (r (192) = .407, p < .001); marijuana serves as a gateway drug (r (192) = -. 385, p < .001); marijuana is less harmful than tobacco (r (191) = .320, p < .001); and, marijuana is addictive (r (192) = -.316, p < .001). Similarly, several items were found to be significantly related to ratings for marijuana should be legalized for recreational purposes, including: marijuana serves as a gateway drug (r (190) = -.627, p < .001); marijuana is less harmful than alcohol (r (190) = .588, p < .001); marijuana should be legalized for medical purposes (r (191) = .523, p < .001); legalizing marijuana would make it readily accessible to minors (r (190) = -.510, p < .001); marijuana is addictive (r (190) = -.493, p < .001); legalizing marijuana would lead to more people trying it (r (190) =.421, p < .001); and, marijuana is less harmful than tobacco (r (189) = .404, p < .001).
Multiple regression analyses found that a combination of three variables accounted for a significant percent of the response variance (R2 = .316) for marijuana should be legalized for medical purposes (F (3, 176) = 27.046, p < .001). Those variables included marijuana should be legalized for recreational purposes, legalizing marijuana would make it readily accessible to minors, and marijuana is less harmful than alcohol. The unstandardized coefficients within the predictor model were: 2.239 (constant) + .384 (legalized for recreational purposes) + .163 (readily accessible to minors) + .152 (less harmful than alcohol).
Similarly, analyses found that a combination of four variables accounted for a significant percent of the variance (R2 = .596) for agreement ratings for marijuana should be legalized for recreational purposes (F (4, 175) = 64.443, p < .001). Those variables included marijuana serves as a gateway drug to stronger drug use, marijuana should be legalized for medical purposes, legalizing marijuana would make it readily accessible to minors, and marijuana is less harmful than alcohol. The unstandardized coefficients within this model were: 2.582 (constant) -.389 (gateway drug) + .399 (legalizing for medical purposes) - .273 (readily accessible to minors) + .229 (less harmful than alcohol).
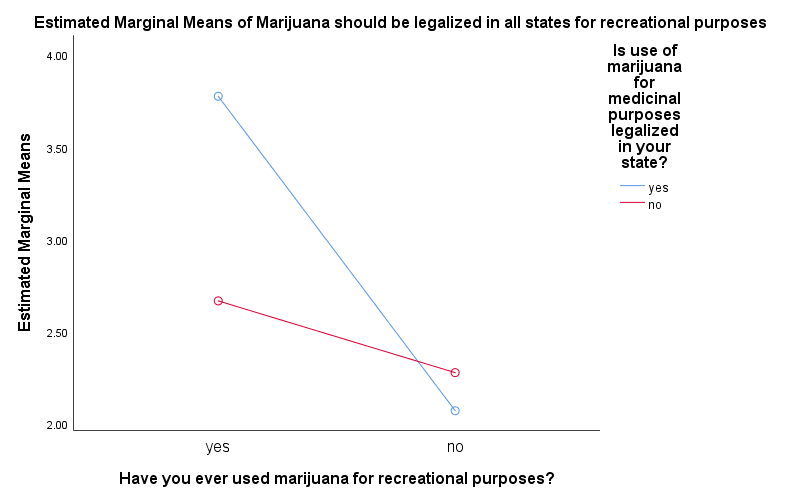
A two-way ANOVA was utilized to compare whether or not one had ever used marijuana for recreational purposes and whether marijuana was legal in their state for medical purposes in respect to agreement ratings for marijuana should be legalized for recreational purposes. A significant interaction effect was found (F (1, 181) = 10.668, p = .001). This effect is presented in Figure 1 below. Those who had used marijuana for recreational purposes and were living in a state where marijuana was legal for medical purposes were most likely to agree that marijuana should be legalized for recreational purposes (x = 3.776), while lowest ratings were recorded for those who had not tried marijuana and living in a state where marijuana for medical purposes was legal (x = 2.071).
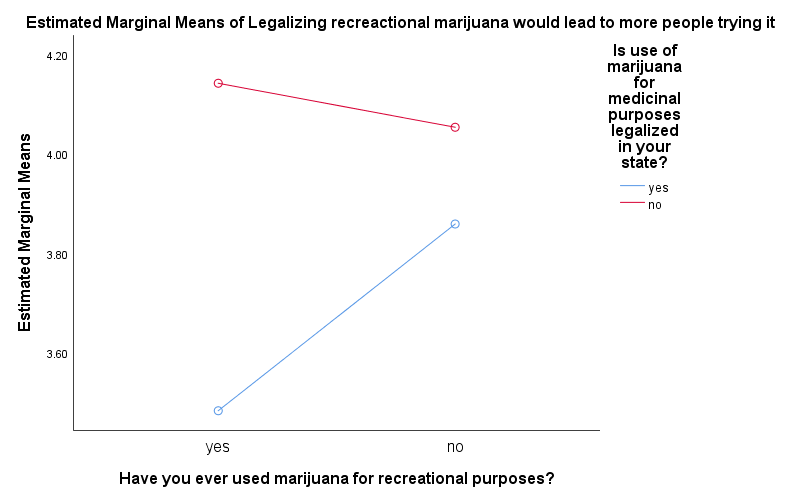
A second two-way ANOVA was calculated to examine whether or not one had ever used marijuana for recreational purposes and whether marijuana was legal in their state for medical purposes in respect to ratings for should marijuana should be legalized for recreational purposes it would lead to more people trying it. The interaction between the variables approached but did not achieve statistical significance (F (1, 183) = 1.931, p = .166). This relationship is presented in Figure 2 below. Lowest agreement ratings came from those who had tried marijuana for recreational purposes and were residing in a state where marijuana for medical purposes is legal (x = 3.483), while the highest ratings were by those who had tried marijuana for recreational purposes but not living in a state where marijuana for medical purposes is legal (x = 4.143).
Discussion
The present study attempted to ascertain the extent of marijuana use and reasons for usage along with attitudes and beliefs toward marijuana use among a national random sample of US occupational therapy healthcare practitioners. The majority of respondents were found to be living in states where marijuana was legal for medical purposes but not recreational purposes, generally due to the significant variation between the low number of states permitting recreational use versus the greater number of states permitting medical use.
Approaching half (44.3%) of these OTs admittedly used marijuana at some time in the past, with their initial use taking place when around 19 years of age. This percent of life use closely mirrors that found nationally among the general public (45.2%) [1]. For most, last use of marijuana was twenty or more years past. Usage was primarily for recreational purposes, including being able to get high, feel good, be sociable, and to relax, once again mirroring reasons expressed among the national population [12]. Least likely reasons to have used marijuana were those related to countering negative feelings of hopeless or depression, and/or to forget painful memories, also similar to national results [12].
The percentage of OTs in this study who reported they used marijuana for medical purposes (7.2%) was comparatively small, with most of those who did so tending to live in a state where medical use of marijuana was legal. Moreover, the majority of these individuals were also inclined to report they had used marijuana for recreational purposes. Reasons for their medical use, however, were not assessed.
Regardless of use or non-use, all participants rated their degree of agreement with an assortment of statements regarding marijuana and marijuana use, including statements specific to currently debated beliefs and attitudes. Significant differences were found between users and non-users in their agreement ratings toward specific item statements, notably: marijuana is less harmful than alcohol, marijuana serves as a gateway drug to stronger drug use, and marijuana is addictive. Those who had used marijuana at some point in their lives tended to agree more strongly that marijuana is not as harmful as alcohol, but agree less strongly that it is a gateway drug or that it is addictive, than did non-users. These item ratings were utilized in combination to substantiate a significant differentiation between the two groups in their overall favorability toward marijuana and marijuana use, and as key predictor variables in agreement ratings regarding legalization of marijuana for recreational purposes. Nevertheless, average item ratings from all respondents tended to reflect those of the general US public.
One of the more interesting findings came from an analysis of the agreement ratings as to whether marijuana should be legalized for recreational purposes stemming from an interaction of two factors – (1) whether or not the OT personally used marijuana for recreational purposes, and (2) whether or not marijuana was legal in their state of residence for medical purposes. While differentiations were found between those who had used marijuana and those who had not, it was the added impact of living in a state where marijuana was legal for medical purposes that promoted higher agreement ratings for recreational legalization. Consequently, highest agreement ratings toward legalization of marijuana for recreational purposes came from those who had used marijuana and living in states where marijuana for medical purposes was legal, while those who had used marijuana but were living in states where it was not legal for medical purposes tended to respond similarly to those who had never tried the drug by responding with low agreement ratings.
Conclusion
Results from the current study suggest that the percentage of OTs who used marijuana at some point in their lifetime is comparable to that of the general US population. Regrettably, no questions were proposed to determine the frequency or depth of use by these participants to compare with national trends, and sadly no previous research exists to ascertain rate of change among occupational therapists, if any, over the past years. National studies of the overall population, however, indicate that likelihood and frequency of use has only modestly increased over the past decade, with this increase found in the 26 and older grouping, but not in the 25 and younger age grouping [35]. Nevertheless, marijuana use among 18 to 25 year olds remains high at roughly twenty percent use in past month [36], compared with just eight percent for those 26 and older [36, 37]. Yet, contrary to expectations, likelihood of use among the general population, or segments of the population, in those states where marijuana has been legalized for medical purposes, and especially in those states where it has been legalized for recreational purposes, has not materialized [38]. Similarly, in a systematic review and meta-analysis, Sarvet found no increase in prevalence of use among adolescents following legalization compared to use prior to legalization [39].
Nonetheless, negative consequences stemming from marijuana use have taken place in states where use has been legalized. For example, usage among adults who were already using marijuana before legalization in their state took place tended to increase as did use among adolescents in 8th and 9th grade who were using prior to legalization [40, 41]. Calls to poison care centers for 9 through 17 year olds dramatically increased while hospitalizations for 18 through 25 year olds essentially tripled [42]. Congruently, risk for initial incidence of marijuana use disorder has increased secondary to higher concentrations of phytocannabinoids in current supplies of the drug, whereby concentrations in the 0’s was estimated at under 4 percent compared to 50% or higher in current supplies [43, 44].
At this point, the American Occupational Therapy Association has not adopted any position on the use of marijuana for medical or personal/recreational purposes among its members. However, this is not unusual given the lack of any such position among other health professions, other than the standard recommendation that members follow the laws of the state in which they practice. Nevertheless, because the impact of consuming marijuana, like that of other substances such as alcohol, is multi-consequential, the results of this study present need for ongoing address of this topic by the profession. This would include a continued monitoring of substance use among its members, the promotion of available treatment options for those abusing marijuana or other mood- altering substances, and a focused emphasis on substance abuse within educational curricula. Such address will provide increased support and assistance to members abusing the substance when needed, and provide ongoing accountability and reassurance to the public at large.
Limitations
A primary limitation in the present study was the overall low return rate often typified in postal surveys. Moreover, because of the professional sensitivity of the topic of marijuana use, those individuals currently using the drug for recreational purposes, especially in states where use is not legal, may have been hesitant to respond. In addition, because the sample was obtained from and constituted only members of the American Occupational Therapy Association, in which a disproportionately low percentage of occupational therapists in the United States maintain membership, the results may not accurately reflect the beliefs and behaviors of all US occupational therapy practitioners, nor are the results likely to reflect attitudes and use of marijuana among occupational therapists in any other country.
Declaration of Conflicting Interests
The authors report no conflicts of interest. The authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest or non-financial interest in the subject matter, materials, or results discussed in this manuscript. The authors alone are responsible for the content and writing of the paper.
Funding
This research received no specific grant support from any funding agency in the public, commercial, or not-for- profit sectors.
References
-
Samhsa Results from the (2017) National Survey on Drug Use and Health: Detailed Tables. Samhsa, CBHSQ.
-
Atakan Z (2012) Cannabis, a complex plant: Different compounds and different effects on individuals. Ther Adv Psychopharmacol 2(6): 241-254.
-
Pertwee RG (2006) The pharmacology of cannabinoid receptors and their ligands: An overview. Int J Obes 1: 13-18.
-
Izzo AA (2004) Cannabinoids and intestinal motility: Welcome to CB2 receptors. Br J Pharmacol. 142(8): 1201-1202.
-
Schauer GL, King BA, Bunnell RE, Promoff G, McAfee TA, et al. (2016) Toking, Vaping, and Eating for Health or Fun: Marijuana Use Patterns in Adults, U.S., 2014. Am J Prev Med 50(1): 1-8.
-
National Institute of Health (NIH) (2018) National Institute on Drug Abuse. Marijuana: What are marijuana effects?
-
Grella CE, Rodriguez L, Kim T (2014) Patterns of medical marijuana use among individuals sampled from medical marijuana dispensaries in Los Angeles. J Psychoactive 46(4): 267-275.
-
Nunberg H, Kilmer B, Pacula RL, Burgdorf JR (2011) An analysis of applicants presenting to a medical marijuana specialty practice in California. J Drug Policy Anal 4(1): 1.
-
Nussbaum AM, Thurstone C, McGarry L, Walker B, Sabel AL, et al. (2015) Use and diversion of medical marijuana among adults admitted to inpatient psychiatry. Am J Drug Alcohol Abuse 41(2): 166-172.
-
Ryan‐Ibarra S, Induni M, Ewing D (2015) Prevalence of medical marijuana use in California, 2012. Drug Alcohol Rev 34(2): 141-146.
-
Whiting PF, Wolff RF, Deshpande S (2015) Cannabinoids for medical use: A systematic review and meta-analysis. JAMA 313(24): 2456-2473.
-
Patrick ME, Bray BC, Berglund PA (2016) Reasons for marijuana use among young adults and long-term associations with marijuana use and problems. J Stud Alcohol Drugs 77(6): 881-888.
-
McGinty EE, Samples H, Bandara SN, Saloner B, Bachhuber MA, et al. (2016) The emerging public discourse on state legalization of marijuana for recreational use in the US: Analysis of news media coverage, 2010–2014. Prev Med 90: 114-120.
-
McGinty EE, Niederdeppe J, Heley K, Barry CL (2017) Public perceptions of arguments supporting and opposing recreational marijuana legalization. Prev Med 99: 80-86.
-
Drug Enforcement Administration (DEA) Drug scheduling.
-
Campbell W, Twenge J, Carter N (2017) Support for marijuana (cannabis) legalization: Untangling age, period, and cohort effects. Collabra: Psychol 3(1): 1-2.
-
Felson J, Adamczyk A, Thomas C (2019) How and why have attitudes about cannabis legalization changed so much? Soc Sci Res 78: 12-27.
-
Quinnipiac University (2016) Allow marijuana for vets with PTSD, US. voters say 10-1, Quinnipiac University national poll finds; slim majority say legalize marijuana in general.
-
Stetten N, Pomeranz J, Moorhouse M, Yurasek A, Blue AV, et al. (2018) The level of evidence of medical marijuana use for treating disabilities: A scoping review. Disabil Rehabil 20: 1-12.
-
Baldwin JN, Scott DM, Agrawal S (2006) Assessment of alcohol and other drug use behaviors in health professions students. Subst Abus 27(3): 27-37.
-
Baldwin JN, Davis-Hall ER, DeSimone II (2008) Survey of attitudes and behaviors toward alcohol and other drug use in allied health and physician assistant students. J Allied Health 37(3): 156-161.
-
Baldwin JN, Bartek JK, Scott DM, Davis-Hall RE, DeSimone II EM, et al. (2009) Survey of alcohol and other drug use attitudes and behaviors in nursing students. Subst Abus 30(3): 230-238.
-
Chan MH, Knoepke CE, Cole ML, McKinnon J, Matlock DD, et al. (2017) Colorado medical students’ attitudes and beliefs about marijuana. J Gen Intern Med 32(4): 458-463.
-
Moeller KE, Woods B ( 0 5) Pharmacy students’ knowledge and attitudes regarding medical marijuana. Am J Pharm Educ 79(6): 85.
-
Doblin RE, Kleiman MA (1991) Marijuana as antiemetic medicine: a survey of oncologists’ experiences and attitudes. J Clin Oncol 9(7): 1314- 1319.
-
Flaherty JA, Richman JA (1993) Substance use and addiction among medical students, residents, and physicians. Psychiatr Clin 16(1): 189-197.
-
Hughes PH, Brandenburg N, Baldwin DC (1992) Prevalence of substance use among US physicians. JAMA 267(17): 2333-2339.
-
Linn LS, Yager J, Leake B ( ) Physician’s attitudes toward the legalization of marijuana use. West J Med 150(6): 714-717.
-
Lipp MR, Benson SG (1972) Physician use of marijuana, alcohol, and tobacco. A J Psychiatry 129(5): 612-616.
-
McAuliffe WE, Rohman M, Fishman P (1984) Psychoactive drug use by young and future physicians. J Health Soc Behav 25(1): 34-54.
-
McAuliffe WE, Santangelo SL, Gingras J, Rohman M, Sobol A, et al. (1987) Use and abuse of controlled substances by pharmacists and pharmacy students. Am J Hosp Pharm 44(2): 311-317.
-
Trinkoff AM, Storr CL (1998) Substance use among nurses: Differences between specialties. Am J Public Health 88(4): 581-585.
-
AOTA What is Occupational Therapy?
-
Centers for Disease Control and Prevention (CDC). Marijuana and Public health. Therapeutic benefits- What you need to know about marijuana and chronic pain.
-
Azofeifa A, Mattson ME, Schauer G, McAfee T, Grant A, et al. (2016) National Estimates of Marijuana Use and Related Indicators-National Survey on Drug Use and Health, United States, 2002-2014. MMWR Surveill Summ 65(11): 1-28.
-
CBHSQ. Key substance use and mental health indicators in the United States: Results from the 2015 National Survey on Drug Use and Health.
-
National Institute on Drug Abuse (NIDA) Marijuana.
-
Mauro CM, Newswanger P, Santaella-Tenorio J, Mauro PM, Carliner H, et al. (2019) Impact of medical marijuana laws on state-level marijuana use by age and gender, 2004-2013. Prevention Sci 20(2): 205- 214. United States: A systematic review and meta‐analysis. Addiction 113(6): 1003-1016.
-
Leung J, Chiu CY, Stjepanovic D, Hall W (2018) Has the legalisation of medical and recreational cannabis use in the USA affected the prevalence of cannabis use and cannabis use disorders? Curr Addict Rep 5(4): 403-417.
-
Rusby JC, Westling E, Crowley R, Light JM (2018) Legalization of recreational marijuana and community sales policy in Oregon: Impact on adolescent willingness and intent to use, parent use, and adolescent use. Psychol Addict Behav 32(1): 84- 92.
-
Vigil DI, Van Dyke M, Hall KE, Contreras AE, Ghosh TS, et al. (2018). Marijuana use and related health care encounters in Colorado before and after retail legalization. Int J Ment Health Addict 16(4): 806-12.
-
Arterberry BJ, Padovano HT, Foster KT, Zucker RA, Hicks BM, et al. (2019) Higher average potency across the United States is associated with progression to first cannabis use disorder symptom. Drug Alcohol Depend 195: 186-192.
-
Mehmedic Z, Chandra S, Slade D (2010) Potency trends of Δ ‐THC and other cannabinoids in confiscated cannabis preparations from 1993-2008. J Forensic Sci 55(5): 1209-1217.
- Electrolyte Considerations for Athletes
- Comprehensive Rehabilitation in Adults with Diabetic Peripheral Neuropathy: A Literature Review on Frequency, Intensity, and Duration Parameters
- Exercise Duration and Its Association with ADHD Symptom Severity in Children and Adolescents: A Parent-Reported Survey Study
- Adaptation of the Adult Neurophysiology of Pain Questionnaire for Use in Pediatrics
- A Non-Pharmacological Multidisciplinary Pain Program within a Hospital Wellness Program: A Mixed Methods Study
- The Effect of Frenkel's Exercise with PNF on Functional Reach in Stroke Survivors: A Randomized Control Trial