Translating Research to Practice: Taking the Next Step to get Children Diagnosed with Cancer Moving
Most research-based physical activity (PA) interventions show that children diagnosed with cancer experience healthrelated benefits during the intervention period. However, translating these interventions into practice is uncommon. To better understand if/how researchers translate their PA interventions to practice, we identified 65 researchers who had published research manuscripts/conference abstracts detailing PA interventions for children with cancer. Most authors reported their PA intervention was not translated into practice due to financing constraints and low adherence rates during the study period. Of those who did translate, strategies to overcome commonly cited barriers were provided. We can conclude that PA interventions are rarely translated to practice, as doing so is resource-intensive and requires concerted efforts from multiple stakeholders. Findings underscore the complicated nature of knowledge translation and raise questions about whose responsibility it is to move evidence to practice.
Introduction
An accumulating body of evidence suggests that research-based physical activity (PA) interventions can offer children diagnosed with cancer benefits [1, 2, 3, 4]. Despite this, efforts to translate PA interventions to practice are rarely described [see 5, for a notable exception] potentially contributing to a growing knowledge-to-practice gap in pediatric oncology. Researchers may be able to lead translation efforts, yet, whether researchers are translating their PA interventions into practice remains unknown. Therefore, we sought to ascertain if/how PA interventions are translated into practice in an effort to offer practical insights and guidance for those seeking to translate their research.
Methods
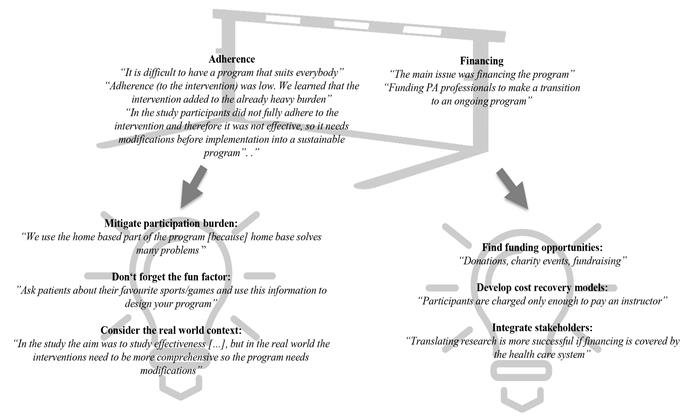
As part of a larger environmental scan [6], we conducted a systematic literature review following established guidelines [7]. Citations were identified through searching five electronic databases, and screening was conducted according to established eligibility criteria [6]. Upon confirming inclusion, the corresponding author(s) of the identified citations were contacted and asked whether their intervention was translated into practice. Based on authors’ response, one of two sets of open- and closed-ended follow-up questions were sent. These questions either asked for more information about the translation process or reasons for not translating, as appropriate. PA intervention information was extracted from the citation. A standardized data charting document was used to collate information from the identified citation and from authors’ responses. Qualitative content analysis was used to analyze authors’ responses to the open-ended questions [8]. Brief quotes to illustrate key findings were selected and are presented in Figure 1.
Results
Sixty-five authors were identified and 49 were contacted. Sixteen authors could not be contacted. Of the 49 authors contacted, 41 responded to the emails. Based on author responses, six programs were included as PA interventions that were translated and 20 were included as PA interventions that were not translated. Fifteen authors did not receive the second email because they did not respond to the first email (n=2) or were unable to provide the required information (i.e., research was ongoing n=2; author was no longer in charge of the PA program n=4; program was developed prior to research n=7).
PA Interventions that were translated
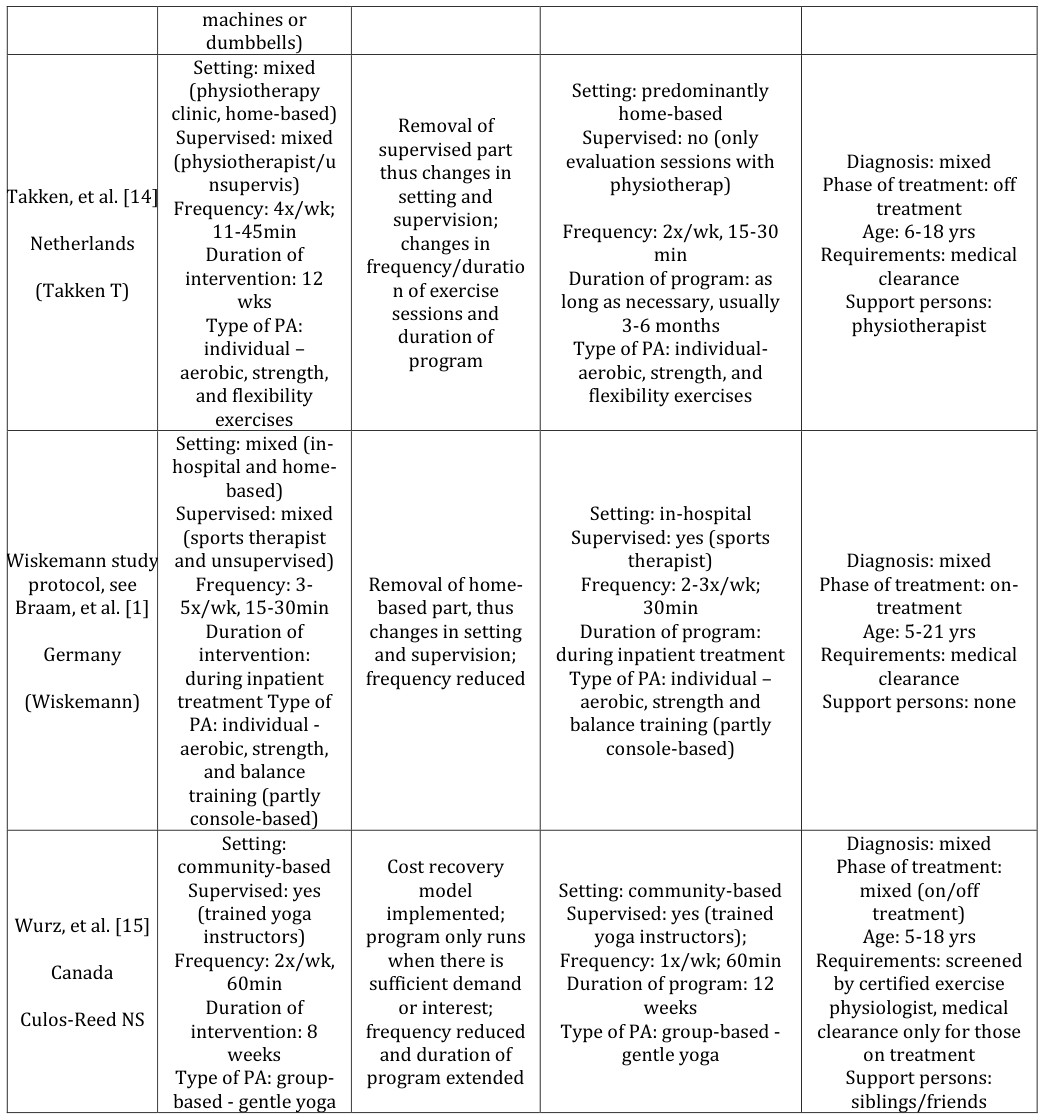
Five of the six authors who translated their PA intervention responded to the questions. Details related to the research-based PA interventions and subsequent translated PA programs can be found in Table 1. Similar to the intervention from which it was translated [1, 3, 9- Study Author, Research-based PA Country (Corresponding intervention as Changes made in translation process described in identified citation Author) Setting: in-hospital Supervised: yes (sports therapist) Frequency: 1x/wk, Beulertz, et al. [3],
60min Duration of
Germany,
intervention: 6 Duration of program not months Type of PA: group- (Daeggelmann J) limited based - aerobic, strength, coordination exercises and games Setting: in-hospital Fiuza Luces, et al.
Supervised: yes
[9]
(experienced professional) Frequency: 3x/wk,
San Juan, et al.
Integration into
60-120min Duration of intervention: 8- 49wks Type of PA: individual -aerobic
standard care;
Soares Miranda,
duration of exercise sessions et al. [13]
reduced Spain
(cycle ergometer) (Lucia A)
and strength training (resistance
15] programs are being offered in either the hospital or the community [1, 5, 9, 10, 11, 12, 13, 14]. PA professionals lead or supervise most PA programs, with one exception, wherein participants receive PA evaluation sessions with a physiotherapist but perform their PA program unsupervised at home. Programs are offered to any child diagnosed with cancer across the cancer trajectory and medical clearance is required to participate in four of the programs. For one program this is only required for children on-treatment. Two programs are open to support persons (e.g., friends, siblings).
There were no major changes in the type of PA during the translation process. However, four programs reduced the frequency and/or length of each PA session, three authors mentioned modifications in the duration of the PA program, one developed a cost recovery model and the program only runs if there is sufficient demand for classes and one author reported that the PA program was integrated into standard care. Two programs removed either the supervised or home-based part (Table 1).
PA program participants as described in response PA program as described in response to email to email Setting: in-hospital Supervised: yes (sports Diagnosis: mixed Phase of treatment: mixed (during maintenance therapist) Frequency:
1x/wk; 60min Duration of program: Open-
treatment and off- treatment) Age: 4-18 yrs ended Type of PA: group-based- Requirements: medical clearance and written aerobic, strength, coordination, exercises and informed consent Support persons:
games siblings/friends Setting: in-hospital
Supervised: yes (experienced professional)
Diagnosis: mixed Phase of treatment: on- Frequency: 3x/wk, 60-90 min Duration of program: during inpatient treatment treatment (including first year of maintenance treatment) Age: 4-18 yrs Requirements: medical clearance and informed Type of PA: individual – aerobic (cycle ergometer, treadmill, arm cranking, games) and strength consent Support persons: none training (resistance machines or dumbbells)
- Setting: mixed
- (physiotherapy clinic, home-based) home-based
- Supervised: no (only evaluation sessions with
- Removal of supervised part
- Supervised: mixed
- (physiotherapist/u
- Diagnosis: mixed
- Phase of treatment: off thus changes in nsupervis)
- Frequency: 4x/wk; physiotherap)
- Takken, et al. [14] setting and supervision;
- Frequency: 2x/wk, 15-30 treatment
- Age: 6-18 yrs
- Requirements: medical
- Netherlands
- 11-45min
- Duration of intervention: 12 changes in frequency/duratio min
- Duration of program: as long as necessary, usually (Takken T) clearance
- Support persons: n of exercise sessions and wks
- Type of PA: individual – aerobic, strength,
- 3-6 months
- Type of PA: individualphysiotherapist duration of program aerobic, strength, and and flexibility flexibility exercises exercises
- Setting: mixed (inhospital and homebased)
- Supervised: mixed
- Setting: in-hospital
- Supervised: yes (sports
- (sports therapist and unsupervised)
- Wiskemann study therapist)
- Frequency: 2-3x/wk;
- Diagnosis: mixed
- Phase of treatment: onprotocol, see
- Braam, et al. [1]
- Frequency: 3-
- 5x/wk, 15-30min
- Removal of homebased part, thus changes in setting
- 30min
- Duration of program: during inpatient treatment treatment
- Age: 5-21 yrs
- Requirements: medical
- Germany
- Duration of intervention: during inpatient treatment Type of and supervision; frequency reduced (Wiskemann)
- Type of PA: individual – clearance
- Support persons: none aerobic, strength and balance training (partly
- PA: individual aerobic, strength, console-based) and balance training (partly console-based)
- Setting: community-based
- Diagnosis: mixed
- Phase of treatment:
- Cost recovery
- Supervised: yes model implemented; program only runs
- Setting: community-based mixed (on/off
- (trained yoga
- Supervised: yes (trained treatment)
- Age: 5-18 yrs
- Requirements: screened
- Wurz, et al. [15] instructors)
- Frequency: 2x/wk, yoga instructors);
- Frequency: 1x/wk; 60min
- Canada when there is sufficient demand
- 60min
- Duration of intervention: 8
- Duration of program: 12 by certified exercise physiologist, medical clearance only for those
- Culos-Reed NS or interest; frequency reduced weeks
- Type of PA: group-based weeks
- Type of PA: groupbased - gentle yoga and duration of program extended gentle yoga on treatment
- Support persons: siblings/friends
Table 1: Description of research-based PA interventions, changes made during translation, and resultant ongoing PA
As shown in Figure 1, the main barriers mentioned by authors who successfully translated their interventions were related to financing and low recruitment/adherence rates during the PA intervention. To overcome these barriers, authors reported using a variety of funding models, often securing funding from private donors, fundraising/charity events, and institutions/government. As well, authors reported engaging in extensive promotion efforts in order to enhance recruitment rates and modified the PA intervention to ensure adequate adherence (i.e., lessening the number of sessions/week or duration to reduce participation burden).
PA Interventions that were not translated
Sixteen of the 20 authors who indicated they did not translate their research responded to the questions. Eleven stated that they had not planned to translate their research intervention and five reported they were unable to successfully translate their research. The main reason authors did not translate their intervention was because there were no resources to continue the program beyond the intervention period. Moreover, low adherence rates during the PA intervention, non-significant findings, and a range of miscellaneous reasons were also provided (e.g., authors moving institutions and being unable to sustain the PA intervention; see Figure 1).
Discussion
In an effort to understand if/how research interventions are translated into practice, we reviewed the current literature. Findings suggest that only a small proportion of interventions were translated. The authors who intended to translate and were successful in their efforts offered brief insights into practical ways to overcome some barriers to translating research, while those who were unsuccessful underscored challenges that need to be considered. Financing constraints and low adherence rates were common barriers identified. Bolstering funding via concerted efforts and modifying the design of the intervention were necessary to overcome these barriers.
A main finding from this study was that most authors did not translate their research because it was never their intention to do so. They conducted an intervention to examine a specific outcome, and thus the research was not designed with factors to address external validity and generalizability (including implementation into practice). This raises important questions about (a) the design of research without consideration of knowledge translation, (b) current research funding paradigms, and (c) whose responsibility it is to translate PA interventions. On the one hand, researchers may be ideally suited to translate their interventions as they are up-to-date on the best available evidence and designed/conducted the intervention. As such, they have insight into what aspects, if any, should be modified to ensure participant engagement. On the other hand, translating research to practice is often time- and resource-intensive. One possible strategy to mitigate this burden is to provide the minimal PA prescriptions needed for change [16]. Indeed, less frequent PA interventions (e.g., 1-3 days/week) have not only been shown to be effective [3], but have even been reported as a key to the ongoing sustainability of PA programs for children diagnosed with cancer [3].
Moreover, the importance of collaborative and coordinated approaches was highlighted [17]. Those researchers who were successful in translating their intervention described concerted and ongoing engagement with key stakeholders. It may be prudent for researchers to establish and foster relationships with individuals in the local healthcare system (e.g., healthcare providers, administrators) and in the community (e.g., organizations) from study inception onward. As healthcare systems, particularly healthcare providers, have been shown to play a key role in PA promotion [18]. fostering productive healthcare and allied healthcare providers’ relationships might be ongoing education and systems that enable them to easily and efficiently refer to PA interventions/programs [19]. Among older adult cancer survivors, similar ideas have been suggested. Notwithstanding the importance of fostering relationships, it is likely that many researchers may have limited experience engaging stakeholders and translating knowledge. Thus, to move research to practice, it may be important to encourage interdisciplinary collaborations between pediatric oncology/exercise researchers and specialists in knowledge translation and implementation science. This may enhance the likelihood of knowledge translation upon study cessation and could serve to spread out or share the load/effort required to translate research [16]. Moving forward, more efforts to identify how researchers and stakeholders can effectively share responsibility for moving evidence to practice is necessary.
Notably, all authors who successfully translated their research noted that modifications to their PA intervention were necessary, underscoring that highly-controlled trial, which are necessary to establish efficacy, may not be conducive to translational efforts. Thus, more practical/pragmatic trials that consider the complexity of the real world are necessary [16, 17]. Within the context of pediatric oncology, including more heterogeneous samples at different stages of the cancer trajectory would increase generalizability and the pool of potential participants. Further, highly-controlled PA interventions are often costly, which could further hinder effective translation and sustainability efforts [17]. In this regard, researchers may wish to keep the resources in mind that will be required to maintain their intervention and include translation budgets when applying for funding [20, 15].
Finally, it should be noted that translating PA interventions is only one strategy to bridge the knowledge-to-practice gap, as practice does not need to always be translated directly from research. Indeed, the results from the larger environmental scan suggest that some sustainable PA programs offered to children diagnosed with cancer were not translated from research [6]. It would be insightful to determine the way in which these programs were developed and if/how the coordinators ensure evidence-informed practice.
Taken together, findings confirm that only few research-based PA interventions are translated into practice underscoring that once research-based PA interventions end, children diagnosed with cancer are tasked with finding alternatives. Results underscore the barriers faced when engaging in knowledge translation of these and offer insights into strategies to overcome some barriers. As well, results raise important questions that need to be discussed about whose responsibility it is to translate evidence to practice. Moving forward, researchers are urged to consider translating their interventions to sustainable programs to enhance PA participation opportunities for this population. Collaborating and developing practical interventions are likely crucial steps needed in order to get more children diagnosed with cancer moving.
Acknowledgment
The authors would like to thank all of the corresponding authors of the research-based PA interventions for their interest and participation in this project. As well, the authors would like to thank Liam Kronlund and Jena Shank who assisted with the larger environmental scan.
Funding
Amanda Wurz was supported by a Vanier Canada Graduate Scholarship.
Declaration of Interest Statement
The authors declare no conflict of interests.
References
-
Braam KI, van der Torre P, Takken T, Veening MA, van Dulmen-den Broeder E, et al. (2016) Physical exercise training interventions for children and young adults during and after treatment for childhood cancer. Cochrane Database Syst Rev 30: 4.
-
Baumann FT, Bloch W, Beulertz J (2013) Clinical exercise interventions in pediatric oncology: a systematic review. Pediatr Res 74(4): 366-374.
-
Beulertz J, Prokop A, Rustler V, Bloch W, Felsch M, et al. (2016) Effects of a 6-Month, Group-Based, Therapeutic Exercise Program for Childhood Cancer Outpatients on Motor Performance, Level of Activity, and Quality of Life. Pediatr Blood Cancer 63(1): 127- 132.
-
Wurz A, Brunet J (2016) The Effects of Physical Activity on Health and Quality of Life in Adolescent Cancer Survivors: A Systematic Review. JMIR Cancer 2(1): e6.
-
Chamorro Vina C, Guilcher GM, Schulte F, de Vries A, Schwanke J, et al. (2017) Description of a Community- Based Exercise Program for Children With Cancer: A Sustainable, Safe, and Feasible Model. Rehabilitation Oncology 35(1): 24-37.
-
Wurz A, Daeggelmann J, Albinati N, Kronlund L, Chamorro Vina C, et al. (2019) Physical activity programs for children diagnosed with cancer: an international environmental scan. Supportive Care in Cancer 27(4): 1153-1162.
-
Moher D, Liberati A, Tetzlaff J, Altman DG (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ 339: b2535.
-
Hsieh HF, Shannon SE (2005) Three approaches to qualitative content analysis. Qualitative Health Research 15(9): 1277-1288.
-
Fiuza Luces C, Padilla JR, Soares Miranda L, Santana Sosa E, Quiroga JV, et al. (2017) Exercise Intervention in Pediatric Patients with Solid Tumors: The Physical Activity in Pediatric Cancer Trial. Med Sci Sports Exerc 49(2): 223-230.
-
San Juan AF, Fleck SJ, Chamorro Vina C, Mate Munoz JL, Moral S, et al. (2007a) Early-phase adaptations to intrahospital training in strength and functional mobility of children with leukemia. J Strength Cond Res 21(1): 173-177.
-
San Juan AF, Fleck SJ, Chamorro Vina C, Mate Munoz JL, Moral S, et al. (2007b) Effects of an intrahospital exercise program intervention for children with leukemia. Med Sci Sports Exerc 39(1): 13-21.
-
San Juan AF, Chamorro Vina C, Moral S, Fernandez del Valle M, Madero L, et al. (2008) Benefits of intrahospital exercise training after pediatric bone marrow transplantation. Int J Sports Med 29(5): 439- 446.
-
Soares Miranda L, Fiuza Luces C, Lassaletta A, Santana Sosa E, Padilla JR, et al. (2013) Physical Activity in Pediatric Cancer patients with solid tumors (PAPEC): trial rationale and design. Contemporary Clinical Trials 36(1): 106-115.
-
Takken T, van der Torre P, Zwerink M, Hulzebos EH, Bierings M, et al. (2009) Development, feasibility and efficacy of a community-based exercise training program in pediatric cancer survivors. Psychooncology 18(4): 440-448.
-
Wurz A, Chamorro Vina C, Guilcher GM, Schulte F, Culos Reed SN, et al. (2014) The feasibility and benefits of a 12-week yoga intervention for pediatric cancer out-patients. Pediatr Blood Cancer 61(10): 1828-1834.
-
Glasgow RE, Emmons KM (2007) How can we increase translation of research into practice? Types of evidence needed. Annu Rev Public Health 28: 413- 433.
-
Phillips SM, Alfano CM, Perna FM, Glasgow RE (2014) Accelerating translation of physical activity and cancer survivorship research into practice: recommendations for a more integrated and collaborative approach. Cancer Epidemiol Biomarkers Prev 23(5): 687-699.
-
Keats MR, Culos Reed SN, Courneya KS (2007) An examination of the beliefs, attitudes and counselling practices of paediatric oncologists toward physical activity: A provincial survey. Paediatrics & Child Health 12(4): 289-293.
-
Mina DS, Sabiston CM, Au D, Fong AJ, Capozzi LC, et al. (2018) Connecting people with cancer to physical activity and exercise programs: a pathway to create accessibility and engagement. Curr Oncol 25(2): 149- 162.
-
Curtis K, Fry M, Shaban R, Considine J (2017) Translating research findings to clinical nursing practice. J Clin Nurs 26(5-6): 862-872.
- Electrolyte Considerations for Athletes
- Comprehensive Rehabilitation in Adults with Diabetic Peripheral Neuropathy: A Literature Review on Frequency, Intensity, and Duration Parameters
- Exercise Duration and Its Association with ADHD Symptom Severity in Children and Adolescents: A Parent-Reported Survey Study
- Adaptation of the Adult Neurophysiology of Pain Questionnaire for Use in Pediatrics
- A Non-Pharmacological Multidisciplinary Pain Program within a Hospital Wellness Program: A Mixed Methods Study
- The Effect of Frenkel's Exercise with PNF on Functional Reach in Stroke Survivors: A Randomized Control Trial