Еlectroneuromyographic Indices of Respiratory Muscles in Patients with Chronic Obstructive Pulmonary Disease
Elektroneuromyographic studies were carried out according to the amplitude and muscular response of respiratory muscles to electrical stimulation in 28 patients with chronic obstructive pulmonary disease of 2, 2-3, 3 severities at the age of 49 to 65 years. The revealed changes in the functional state of the respiratory muscles and the function of external respiration aggravate the progressive nature of the pathological process in the lungs in chronic obstructive pulmonary disease that requires timely prevention of respiratory failure and the choice of tactics of electrostimulation of respiratory muscles.
Аkhmedov MA
Rehabilitation, Tashkent Pediatric Medical Institute, Uzbekistan
gulora@yandex.ru muscles.
Respiratory Function; Phrenic Nerve; Long Thoracic Nerve; Lungs
Introduction
With intense muscle loads associated with multiple increases in pulmonary ventilation and increased work of the respiratory muscles, inspiratory muscles are prone to fatigue [1, 2, 3, 4, 5, 6, 7, 8]. Among the main criteria for violations of the function of the respiratory muscles are fatigue and weakness of the respiratory muscles. Fatigue of the respiratory muscles is a condition in which there is a decrease in the strength and speed of movement due to excessive work. Fatigue is a reversible process. Under the weakness of the respiratory muscles understand the state Еlectroneuromyographic Indices of Respiratory Muscles in Patients with Chronic Obstructive Pulmonary Disease in which the strength of the respiratory muscles is reduced and in conditions of "rest". The cause of respiratory muscle weakness is metabolic, inflammatory and degenerative changes that lead to dysfunction of the mouse itself, nerves, or neuromuscular connections.
The relevance and practical significance of the study of respiratory muscle function, the need to improve their clinical interpretation is emphasized by leading domestic and foreign scientists [6, 7, 8, 9, 10, 11].
Purpose of the Study
To identify electroneuromyographic changes of respiratory muscles in patients with chronic obstructive Ann Physiother Occup Ther
pulmonary disease depending on the severity for predictive planning of tactics of treatment of respiratory failure.
Material and Methods
28 COPD patients aged 49 to 65 years were monitored male (77 %) female (23%). The first group included patients with COPD with 2 and 2-3 degrees of severity-13 people, patients of the 2nd group-COPD-3rd degree of severity -15 people.
To assess the functional state of the respiratory muscles and diaphragm, electroneuromyography (ENMG) was performed on a Myograph Synapsis Neuro ztech Russian apparatus. The following modes of operation of the apparatus were used: muscle response (M-response), latency (L-lat). The following were determined: the amplitude (mV) of the M-response of the phrenic and long pectoral nerves: laterally (ms) of the nerves of Phrenicus DS (region of the sternoclavicular - mastoid muscle); and N. Toracicus longus DS (Erb's point). We analyzed a graphic image of the pulse extension rate (SPI-distal).
In 49% of patients with COPD of 2 severity, an increase in latency along the research nerves was revealed, at normal amplitude parameters, which indicates the presence of signs of muscular-dystrophic changes in the chest Table1.
The study of the function of external respiration was carried out using a desktop computer spirograph Shiller, and a peak flow meter. The following indicators of respiratory function were calculated: lung capacity - FVC (л); forced exhalation volume - FEV1,0 л;the volume of forced exhalation to the vital capacity of the lung - FEV1,0 / FVC -%;stream indicator of the forced vital capacity of lungs - FEF25-75%; forced exhalation - PEF л\с;peak exhalation rate - MEF 75%; peak exhalation rate - MEF 50%; peak exhalation rate - MEF 25%. Measurement of peak exhalation rate was carried out according to the generally accepted method [10, 11].
Results
Patients complained of causeless shortness of breath, decreased exercise tolerance, periodic respiratory failure in sleep, drowsiness, decreased quality of life, and development of respiratory failure.
In the electroneuromyographic study in healthy and in the control group, muscle responses from the diaphragmatic and thoracic nerves were within normal limits. This indicates the absence of violations on the part of the peripheral neuromuscular apparatus and the muscles of the chest.
| N.Phrenicus D | N.Phrenicus S | N.Thoracicus longus D | N.Thoracicus longus S | |||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Lat.ms | . | A | mp.mv | . | Lat.ms | . | A | mp.mv | . | Amp.mv. | Lat.ms. | Lat.ms. | Amp.mv. | |||||||||||
| Norm | 7,4±2,4 | 0,8±0,9 | 7,4±2,3 | 0,8±1,2 | 3,9±3,3 | 0,8±0,7 | 3,9 ±2,6 | 0,8±1,0 | ||||||||||||||||
| COPD-2 deg. | 0,85±0,9 | 0,86 ±1,3 | 0,23±1,2 | 1,16±2,0 | 4,6±4,1 | 3,75±1,6 | 4,8±2,4 | 7,8±1,8 | ||||||||||||||||
| COPD-2-3 deg. | 0,16±1,0 | 0,06±1,2 | 1,37±1,9 | 0,07±2,0 | 7,05±2,8 | 9,35±3,5 | 9,55±3,3 | 13,55±4,1 | ||||||||||||||||
| COPD-3.deg | 0,63±1,8 | 0,18±1,7 | 0,11±1,6 | 0,09±2,6 | 4,35±3,1 | 5,8±4,0 | 3,65±2,4 | 8,2±5,3 | ||||||||||||||||
| Control | 1,33±1,7 | 1,5±2,4 | 0,45±1,9 | 0,59±1,8 | 3,9±2,9 | 8,358±4,3 | 8,05±3,9 | 6,95±3,7 |
Table 1: presents the results of electroneuromyographic studies in patients with COPD.
In 2% of patients with COPD of 2-3 severity, a moderate increase in latency along the diaphragmatic and long thoracic nerves was revealed. (р>0,05) Patients with In 57% of patients of the second group (COPD-3 severity), a moderate decrease in the amplitude of the muscular response and a moderate increase in latency along the diaphragmatic, long thoracic nerves were found. The revealed signs indicate the presence of moderately pronounced muscular-diaphragmatic changes in the muscles of the chest. Table 2 presents the results of latent electroneuromyography in COPD patients.
| N.Phrenicus D | N.Phrenicus S | N.Thoracicus longus D | N.Thoracicus longus S | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Lat.ms. | Lat.ms. Lat.ms. | Lat.ms. | Lat.ms. | |||||||||
| Norm | 7,4±2,4 | 7,4±2,3 | 0,8±0,7 | 3,9 ±2,6 | ||||||||
| COPD-2 deg. | 0,85±0,9 | 0,23±1,2 | 3,75±1,6 | 4,8±2,4 | ||||||||
| COPD-2-3 deg. | 0,16±1,0 | 1,37±1,9 | 9,35±3,5 | 9,55±3,3 | ||||||||
| COPD-3.deg | 0,63±1,8 | 0,11±1,6 | 5,8±4,0 | 3,65±2,4 | ||||||||
| Control | 1,33±1,7 | 0,45±1,9 | 8,358±4,3 | 8,05±3,9 |
Table 2: Presents the results of electroneuromyographic studies in patients with COPD.
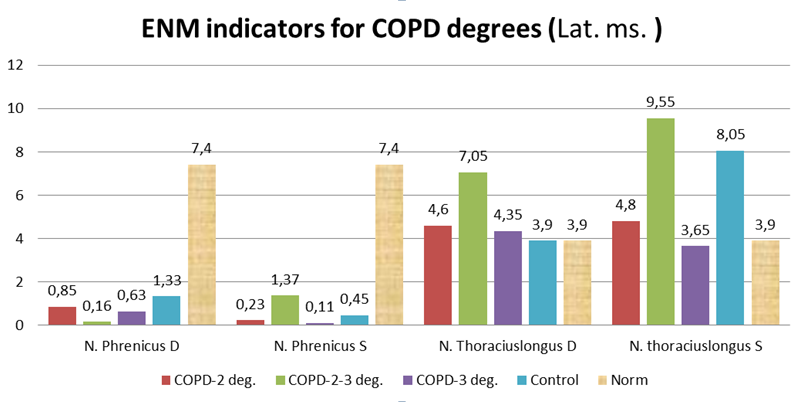
A moderate increase in latency in the left diaphragmatic and right long chest nerve was revealed in the examined patients.
| N.Phrenicus D | N.PhrenicusS | N.Thoracicus longus D | N.Thoracicus longus S | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Amp.mv | Amp.mv | Amp.mv. | Amp.mv | |||||||||
| Norm | 0,8±0,9 | 0,8±1,2 | 3,9±3,3 | 0,8±1,0 | ||||||||
| COPD-2 deg. | 0,86 ±1,3 | 1,16±2,0 | 4,6±4,1 | 7,8±1,8 | ||||||||
| COPD-2-3 deg. | 0,06±1,2 | 0,07±2,0 | 7,05±2,8 | 13,55±4,1 | ||||||||
| COPD-3.deg | 0,18±1,7 | 0,09±2,6 | 4,35±3,1 | 8,2±5,3 | ||||||||
| Control | 1,5±2,4 | 0,59±1,8 | 3,9±2,9 | 6,95±3,7 |
Table 3: presents the results of the amplitude of the muscle response to electroneuromyography in patients with COPD.
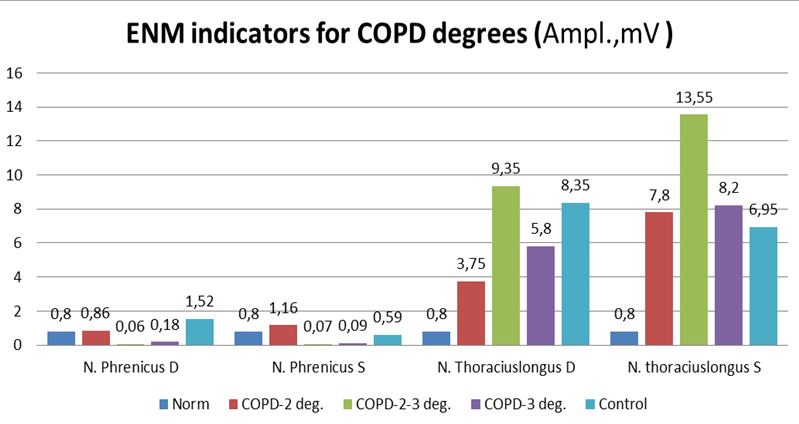
Patients with COPD revealed the same type of changes: the amplitudes of the m-response along the long thoracic nerves from 2 sides were reduced; moderate signs of muscular-dystrophic changes in the anterior dentate muscles of the chest from 2 sides were reduced.
Thus, in patients with COPD with varying degrees of activity revealed: a moderate decrease in the amplitude of the muscular response to the diaphragmatic, long thoracic nerve, signs of muscular dystrophic changes and moderate dysfunction of the chest muscles. The obtained data confirm the opinion of a number of authors that the thickening of the diaphragmatic muscle is associated with its hyperactivity due to increased respiratory load on the background of bronchial obstruction.
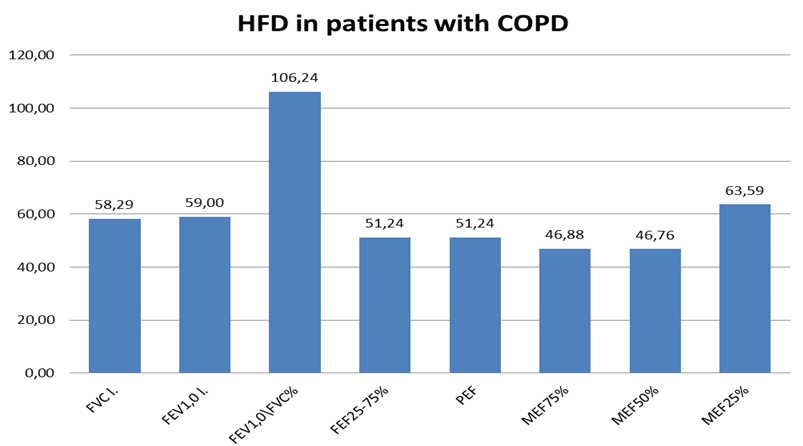
In the study of respiratory function, the majority of the examined patients showed moderate restrictive disorders with a decrease in bronchial patency of the bronchi, as evidenced by PFT 1.0, which were moderately reduced in all patients. Moreover, in 7 patients the decrease was 8-10% of the proper values, and in 4 patients - more than 13%. FVC (l) was significantly reduced in all observation groups (p <0.05). A moderate decrease was noted - MEF 50% to 43.7 ± 4.3% (Figure 3).
In most patients with COPD 3rd stage pronounced bronchial obstruction was detected, as evidenced by PSV, which was reduced by 20-25% (p <0.05) in 21 patients (60%), and in 14 patients (40%) the peak expiratory flow was reduced by 27-35 % (p <0.05). FEV1 was reduced (by 25% at p <0.05), which indicated the progression of the pathological process in these patients. In patients with COPD, overexposure of the lungs is detected, arising from airway obstruction and also able to adversely affect the function of the respiratory muscles.
In patients with COPD, overexposure of the lungs is detected, arising from airway obstruction and also able to adversely affect the function of the respiratory muscles. In patients with COPD, overexposure of the lungs is detected, arising from airway obstruction and also able to adversely affect the function of the respiratory muscles.
The revealed changes indicated an increase in the degree of bronchial obstruction in patients with COPD, this exacerbated the adverse conditions for the functioning of the diaphragm in this category of patients and created the prerequisites for the development and progression of respiratory failure.
Other groups of respiratory muscles are forced to take on a significant share of ventilation work with ineffective contractions of the diaphragm, at the first stages compensating for the” fatigue “of the diaphragm, but then come the irreversible state of the diaphragm - its "weakness". Consequently, the role of other groups of respiratory muscles in the formation of the respiratory act as a whole is much smaller, and they cannot compensate for the work of the "tired" diaphragm for a long time [1, 2, 3, 8]. The results confirm that at the beginning of the pathological process in COPD patients, there is hyper function of the diaphragmatic muscle, a change in the rate of relaxation of the diaphragm muscle, a decrease in the size of the diaphragm with forced breathing. Further progression of the pathological process in the lungs leads to the development and aggravation of respiratory failure [2, 3, 4].
Findings
In patients with COPD with manifestations of airway obstruction on electroneuromiography revealed the same type of changes: reduced amplitude of the muscular response to the long thoracic nerves, moderate signs of muscular-dystrophic changes in the muscles of the chest.
The results of the studies will allow to assess the prognostic significance as predictors of the adverse course of COPD, will be able to serve as a basis for the development of indications for differentiated complex application of treatment methods including electromyostimulation in respiratory muscular dysfunction of patients with COPD [10, 12, 7].
References
-
Avdeev SN (2002) Dyspnea: mechanisms of development, assessment and treatment: a manual for doctors, pp: 1-25.
-
Avdeev SN (20O4) Functional tests to assess the strength of respiratory muscles in clinical practice. Pulmonolop, pp: 104.
-
Avdeev SN (2004) The role of pulmonary hyperinflation in the pathogenesis of chronic obstructive pulmonary disease. The role of maintenance therapy in reducing pulmonary hyperinflation. Pulmonology, pp: 101-108.
-
Belevsky AS (2014) Global strategy for diagnosis, treatment and prevention of chronic obstructive pulmonary disease. Russian respiratory society.
-
Milani RV, Mi-Lani CJ, Mehra L (2004) How do you determine the cause of shortness of breath? Blood Circulation, pp: e27-e31. 26220 26700
-
Chauhan A, Sridhar G, Clemens R, Krishnan B, Marciniuk DD, et al. (2000) Role of Respiratory Function in Exercise Limitation in Chronic Heart Failure. Chest 118(1): 53-60.
-
Sadykova GA, Bazarova SA, Aripov BS, Akhmedov MA (2018) Electromyostimulation of respiratory muscles in the practice of pulmonologist. Journal Therapeutic Bulletin of Uzbekistan, pp: 29-32.
-
Segizbaeva MO, Alexandrova NP, Timofeev NN, Kuryanovich EN (2016) EMG analysis of human inspiratory muscle resistance to fatigue during exercise. Adv Exp Med Biol 788: 197-205.
-
Aleksandrov AL, Perley VE, Gichkin A Yu, Surkova EG, Yakovleva NG, et al. (2009) Journal Scientific notes of St. Petersburg StateMedical University named after I.P.Pavlova 2012. 14(3): 66-69.
-
Maryanova OV (2005) Clinical and asthma. Abstract. Say for a job step scientist. Cand Honey Science Ivanovo 6(5): 898-902.
-
Novik GA, Borichev AV (2005) Spirometry and peak flowmetry in children with bronchial asthma (practice of evaluation and monitoring): textbook. Allowance / under the editorship of prof. Vorontsova IM. SPb, pp: 67.
-
Chuchalin AG, Avdeev SN, Isanov ZR (2016) Russian Respiratory Society. Federal Guidelines on Diagnosis and Treatment of Chronic Obstructive Pulmonary Disease. Russian respiratory society pp: 37-54.
- Electrolyte Considerations for Athletes
- Comprehensive Rehabilitation in Adults with Diabetic Peripheral Neuropathy: A Literature Review on Frequency, Intensity, and Duration Parameters
- Exercise Duration and Its Association with ADHD Symptom Severity in Children and Adolescents: A Parent-Reported Survey Study
- Adaptation of the Adult Neurophysiology of Pain Questionnaire for Use in Pediatrics
- A Non-Pharmacological Multidisciplinary Pain Program within a Hospital Wellness Program: A Mixed Methods Study
- The Effect of Frenkel's Exercise with PNF on Functional Reach in Stroke Survivors: A Randomized Control Trial