Best Practices for Oral Motor Stimulation to Improve Oral Feeding in Preterm Infants: A Systematic Review
Objective: Interventions within the scope of occupational therapy were examined to identify the effectiveness of prefeeding interventions toimprovefeedingoutcomesofprematureinfants.Evidence-based methods ofperi-oral and intra-oral stimulationandoral supportwereexploredandwillbediscussed inthis review. Method: Literature published from 1995 to 2015 using eight electronic databases and Cochrane Database of Systematic Reviews was searched. Fifteen studies met the inclusion criteria and were critically appraised and synthesized. Results: Analysis revealed bestpractices utilizing four areas of intervention: oral motor stimulation, non- nutritive sucking, oral support, andco-interventions. Conclusion: For infants, feeding is a vital occupation that supports growth and development. However, premature infants often have difficulties with the feeding process. Occupational therapists working with pre- term infants must have a sufficient understanding of the evidence to be able to employ best practices to improve pre-feeding readiness and oral feedings. Immature suck-swallow-breath coordination; absent, delayed, or impaired oral reflexes; abnormal muscle tone; and impaired motor control impact the infant’s safe and successful oral intake of adequate nutrition. Strong evidence supports theuse ofperi-oral and intra-oral stimulation forpre-feeding readiness andpreparation topromote successful oral feeding in preterm infants. There is also strong evidence to substantiate the use of oral support during feeding of preterm infants to increase suction and decrease liquid loss topromote efficient intake of nutrition.
Introduction
Annually in the United States, approximately 9.57% of all births are preterm with a gestation period of less than 37 weeks [1]. Pre-term infants are at high risk for oral feeding difficulties when compared with term-born infants. Frequently preterm infants, particularly those born at less than 32 weeks gestation, receive gavage feedings via orogastric (OG) or nasogastric (NG) tube as the suck- swallow reflex is typically not coordinated enough for oral feeding [2]. The ability to coordinate suck, swallow, and breathing processes leads to safe and successful oral feeding [3, 4, 5, 6]. If complicated by immature or absent oral reflexes, abnormal muscle tone and/or impaired oral motor control, oral intake of nutrition is further compromised.
Following best practices, feeding in the neonatal intensive care unit (NICU) more commonly follows an infant driven approach based on feeding readiness. Characteristics of feeding readiness include (1) physiologic stability of heart and respiratory rates, oxygen saturations, skin color, and temperature; (2) neurobehavioral state of being awake and alert, demonstrating flexion postures, and visual regard to caregiver and/or feeding source; and (3) feeding readiness/hunger cues such as fussiness prior to feeding, spontaneous rooting and sucking [7, 8]. Methods commonly used to facilitate feeding readiness include oral stimulation techniques based primarily on Beckman’s Oral Motor Intervention (BOMI), non-nutritive suck (NNS), and oral support. BOMI is a 15-minute stretch and stimulation of peri-oral (cheeks, lips, jaw) and intra-oral (inside of cheeks, gums, tongue) structures and concluding with NNS [9]. NNS is stimulated with a gloved finger, pacifier, or nipple without the introduction of food. Oral support is the provision of external assistance to cheeks, chin, and/or lips [4, 9].
The goal of oral feeding therapies in the NICU are to help infants attain full oral feedings, where all nutrition is taken by mouth. An infant’s ability to achieve full oral feedings is a key criterion for hospital discharge [10]. Hence, feeding training for pre-term infants begins in the Neonatal Intensive Care Unit (NICU) [11]. Therefore, strategies to improve infants’ oral motor skills are necessary. The purpose of this review is to synthesize the literature and offer evidence-based recommendations of methodsto facilitateoral motor skills to influence successful oral feeding.
Methods
Research Question
In healthy pre-term infants with oral feeding difficulties, do non-nutritive oral motor stimulation and oral support methods improve infants’ oral feeding skills as demonstrated by time to full oral feedings, volume intake, weight gain, and/or length of hospital stay?
Search Methods
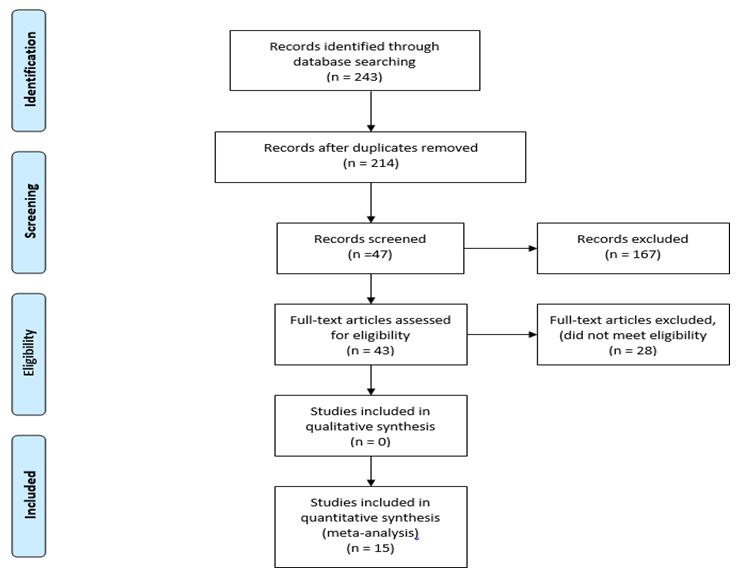
The author conducted a systematic search of the literature published from 1995 to 2015. The search included studies on pre-term infants born at least 28 weeks gestational age (GA) with no contraindications for oral stimulation or oral feeding. The databases searched included CINAHL Complete, CINAHL Plus with Full Text, E- Journals, Health Source: Nursing/Academic Edition, MEDLINE, OVID, and PubMed Clinical Queries. Search terms included oral motor OR oral stimulation, AND preterm infants OR prematurity, AND feeding. The focus was on articles reporting the effectiveness of peri-oral and intra- oral stimulation, NNS, and/or oral support on the outcomes of volume of oral intake, feeding efficiency/proficiency, weight gain, and length of hospital stay. Articles were excluded if they included infants with conditions in which oral stimulation or oral feeding are contraindicated or infants who were not medically stable to tolerate oral stimulation or oral feeding. After literature search results were collected and exact duplicates were removed, the abstracts of the remaining articles were reviewed by the author. Figure 1 depicts the flow of abstracts and articles through the process. One of the articles by Lessen [12] was retained although it included pre- term infants younger than 28 weeks GA since the information was relevant and also included infants through 29 weeks GA. Articles are summarized in Table 1.
Studies included in this review provide Level I and III evidence. Level IV and V evidence was excluded. The American Occupational Therapy Association [13] recognizes the following levels of evidence adapted from [14]. Level I - Systematic reviews, meta-analyses, randomized controlled trials Level II - Two groups, nonrandomized studies (e.g., cohort, case-control) Level III - One group, nonrandomized (e.g., before and after, pretest and posttest) Level IV - Descriptive studies that include analysis of outcomes (single-subject design, case series) Level V - Case reports and expert opinion that include narrative literature reviews and consensus statements
Quality Review
Cincinnati Children’s Hospital Medical Center’s (CCHMC) evidence evaluation tools & resources were used with permission [15]. CCHMC utilizes Let Evidence Guide Every New Decision system to guide the evaluation of evidence, develop best evidence statements and evidence-based care guidelines, and guide decision-making to “achieve the best, safest care for children” [16]. The author used the CCHMC’s LEGEND appraisal forms to appraise each of the articles. For the purpose of this review, the Intervention Systematic Review / Meta-Analysis, Intervention Randomized Controlled Trial or Controlled Clinical Trial, and Intervention Cohort Study forms were used [17]. LEGEND resources were also used to grade the body of evidence and judge the strength of each recommendation.
According to LEGEND’s Grading the Body of Evidence (BOE) system, a high BOE indicates that there is a sufficient number of high quality studies with consistent results on the topic; a moderate BOE indicates that the studies included a single well-done trial, multiple lesser quality trials, or multiple large, high-quality observational studies on the topic; a low BOE indicates that studies included were of lesser quality or with some uncertainty on the topic; a very low BOE indicates that the studies included were of insufficient quality including descriptive studies, case series, general reviews, insufficient design or execution, there were too few studies, and/or inconsistent results; and grade not assignable indicates local consensus only [18]. LEGEND’s dimensions for “judging the strength of a recommendation” include the components of safety/harm, benefits, burden to adhere to recommendations, cost-effectiveness, directness of the evidence, impact on quality of life, morbidity, and mortality, and grade of the BOE resulting in strengths of high, moderate, weak, or no recommendation [19].
Results
Fifteen articles were reviewed for the final synthesis. The articles provide Level I evidence, with the exception of one Level III article. Findings were organized into four areas of intervention: oral motor stimulation, non- nutritive sucking, oral support, and co-interventions. Supplemental provide information on risk of bias of articles.
All studies exhibited a low risk of bias, with the exception of the meta- analysis by Daley and Kennedy [20], which presented with moderate risk due to lack of information related to data extraction, number of excluded articles, and unclear study appraisal methods.
Figure format from “Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement,” by D. Moher A, Liberati J, Tetzlaff DG, Altman; PRISMA Group [21],
| Level of Evidence/Study | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Design/ | Intervention and | Outcome | ||||||||||||
| Author/Year | Results | |||||||||||||
| Participants/Inclusion | Control Groups | Measures | ||||||||||||
| Criteria | ||||||||||||||
| Arvesdson, et al. [3] doi:10.1044/10 58- 0360(2010/09- 0067) | Level I Systematic review N = 12 studies Inclusion Criteria • Published in peer- reviewed journal • Between 1960-2007 • Experimental, quasi- experimental, or multiple- baseline single-subject design • Conducted on preterm infants and examine the effects of OMI (as defined by this EBSR) used as a treatment (not just a single application) to facilitate oral feeding and swallowing skills | Intervention Oral support, oral and peri-oral stimulation, NNS via pacifier either during gavage feedings or pre-oral feeding, and/or sensory input. For studies with control groups, either no stimulation/interve ntion, sham intervention, or stroking was provided. | Feeding/swal lowing physiology Transition time to oral feeding Volume of intake Weight gain. | The majority of studies showed statistical significance in the areas of feeding time and feeding rate following oral stimulation. Three studies demonstrated statistical significance on weight gain. NNS with and without oral/perioral stimulation resulted in strong positive findings for improvement in some feeding/swallowing physiology variables and statistically significant reduction in time to oral feeding. Pre-feeding stimulation showed equivocal results across the outcomes. | ||||||||||
| Asadollahpour, et al. [22] doi:10.5812/ijp. 25(3) 2015.809 | Level I RCT N = 32 Intervention Group 1, n=11. M/F = 6/5 Intervention Group 2, n=10. M/F = 5/5 Control Group, n=11. M/F = 5/6 Inclusion Criteria • preterm infants from 26 to 32 weeks of gestational age • fed through a tube • birth weight of 1000 to 2000 grams | Intervention Group 1: NNS – palate stroking to elicit suck during first 5 mins of tube feeding, 3 times per day. Group 2: Once daily pre-feeding oral stimulation protocol by Fucile et al.: 12 mins stroking of cheeks, gums and tongue, followed by 3 mins of NNS Control Sham intervention: | Time to independent oral feeding Length of hospital stay Weight gain. | NNS and pre-feeding stimulation groups reached 7.55 and 6.07 days sooner to independent oral feeding than in the control group, though not statistically significant. Weight gain at discharge time was significant higher (p<0.05) in NNS group than control and pre- feeding oral stimulation groups. |
therapists’ hands in incubator without touching infant for
15 mins.
All interventions
provided for 10 consecutive days.
Level III Cohort prospective study
Intervention Measurement of NNS, standardized
N = 51
Bingham, et al.
[23]
M/F = 16/35
doi:10.1136/ad c.2009. 164186 feeding advance schedule, and performance of Inclusion Criteria • infants born between 25 NOMAS.
and 34 weeks’ PMA
Intervention Group 1: Oral
stimulation protocol: cheeks, lips, and tongue were stimulated to breathing comfortably with no respiratory support or with nasal cannula (room improve muscle contractility, and air) only Level I RCT strength and orientation reflexes, Boiron, et al.
[24]
Intervention Group 1, n=9.
inhibit mouth- closing reflex, and initiate sucking and https://doi.org/ M/F = 5/4
10.11 11/j.1469- 8749.2007.0043 Intervention Group 2, n=11.
swallowing (SS) reflexes.
M/F = 4/7 Intervention Group 3, n=12.
Group 2: Oral support: chin, cheek,
9.x M/F = 7/5 Control Group, n=11. M/F =
and lip support to
7/4 aid in lip closure and deglutition and movement of nipple to corner of mouth to stop SS pattern to facilitate breathing.
Level I Meta-analysis
Intervention Sucking apparatus
Daley, et al. [25]
N = 10 studies
with and without NPO, oral feeding with and without doi:10.1097/00 Inclusion Criteria • English-language papers
00523 7- 200012000- NGT in place, various nipple
00006 on nipple feeding, feeding performance, and feeding types, breast feeding vs bottle Infants with higher NNS organization scores transitioned to FOF 3 days PMA at IOF PMA at FOF PMA at SOF earlier (p<0.05) than infants with more chaotic patterns of suck bursts and Transition time IOF to a higher NNS organization FOF.
score resulted in fewer number of days from IOF
to SOF (p <0.10).
Non-nutritive
pacifier attached to a Non-nutritive sucking pressure and sucking activity were statistically significantly increased for catheter connected to a pressure transducer to the stimulation and the stimulation+ support groups compared with the control group at Day 7 and the pressure amplifier, to calculate the Day 14 (p<0.001). Significant improvement was also noted at Day 17 mean maximum non- nutritive and Day 20 for time for sucking pressure.
milk ingestion.
The following areas did
Effects of NPO, NGT,
not have statistically significant results (as indicated by no to small effect size): NGT, nipple type (only the comparison nipples, breast vs bottle, GA, oral support, oral stim, and of Enfamil to Nuk nipple showed a large effect size), NNS.
breast vs bottle, and NNS.
efficiency in premature feeding, oral support, and NNS
infants • Experimental and quasi-
experimental designs Level I RCT
Intervention
Intervention Group 1, n=19.
Group 1: OS consisting of stroking the lips, M/F = 12/7
Intervention Group 2, n=18.
cheeks, gums, tongue and sucking M/F = 11/7
on a pacifier Intervention Group 3, n=18.
Group 2: Tactile/kinesthetic
M/F = 10/8
Control Group, n=20. M/F =
Fucile [4]
(T/K) involving stroking the body
16/4 and limbs and passive range of Inclusion Criteria
- Clinically stable preterm motion to limbs Group 3: OS + T/K infants, born between 26 and 32 weeks GA
- Appropriate size for GA
- Receiving all tube feedings Control Received no
- No chronic medical stimulation complications Intervention Pre-feeding oral Level I RCT Intervention Group, n=16.
stimulation program based on M/F = 7/9
Beckman’s
Control Group, n=16. M/F =
principles consisting of 12 minutes stimulation
6/10 Fucile, et al. [26]
Inclusion Criteria
- Preterm infants, born between 26 and 29 weeks doi:10.1067/mp to cheeks, lips, gums, and tongue, d.200 2.125731 followed by 3 minutes of sucking GA
- Appropriate size for GA
- Receiving full tube feedings on a pacifier routinely used in the nursery (120 kcal/kg/day)
- No chronic medical Control Sham stimulation The following areas did have statistically significant results: length of NPO prior to feeding, gestational age, oral support, and oral stimulation.
Independent oral feeding was achieved significantly earlier in all three intervention groups than Time to attainment of the control group (p<0.001). Proficiency and independent oral feeding volume transfer were significantly greater in the three intervention groups, Volume of milk taken over first 5 rate of transfer was significantly greater in the minutes OS and multi- OS+T/K groups, and there was less Sucking skills.
volume loss in the OS group only compared to the control group (all tests p<0.042).
Independent oral feeding was attained significantly Time to attain independent earlier in the Exp. group than the control group, 11 oral feeding Number of days to reach ± 4 days (mean ± SD) versus 18 ± 7 days, respectively (P = .005). Overall intake and rate of one and 4 successful oral feedings milk transfer were significantly greater over time in the Exp. group than per day Overall intake the control group (P = .0002 and .046, respectively). There was no difference in length of hospital stay between the 2 groups, although the Exp.
Rate of milk
transfer Length of hospital stay.
group was discharged an average of 5 days sooner Gaebler, et al.
[27]
Intervention Group, n=9.
stroking protocol a higher percentage of nipple/partial nipple feeds Motor
doi:10.5014/ajo M/F = 6/3
and an additional 2- minute perioral and t.50.3. 184
Control Group, n=9. M/F =
intraoral stimulation
8/1 Inclusion Criteria • Preterm infants, born between 30 and 34 weeks program.
Control 5 min pre-feeding
GA
- Medically stable and in stroking protocol only isolette or open crib
- Fed via gavage or nasogastric tube
- No history of cardiac or gastrointestinal disorders, or central nervous system dysfunction Level I RCT Intervention Group 1, n=19.
M/F = not identified
Intervention Group 2, n=18.
Intervention
Group 1: Nonnutritive oral
M/F = not identified
Intervention Group 3, n=18.
motor therapy (NNOMT) M/F = not identified Group 2: Infant massage therapy Control Group, n=20. M/F = Lau, et al. [28]
doi:10.3233/NP not identified (iMT) Inclusion Criteria
- Preterm infants, born between 26 and 32 weeks Group 3: Combined M- 1262612 interventions (NNOMT + iMT) GA
- Appropriate size for GA
- No congenital anomalies or Control No intervention chronic medical (sham) complications
- Characterized as “feeders and growers”
- Clinically stable Level I Intervention RCT Received developed Lessen (2011) Level I Intervention Received developed Premature Intervention Group, n=10. (PIOMI) - specifically designed fo 182115a2a M/F = 4/6 infants Premature infant Lessen [12] 10.1097/ANC.0 oral Moter Intervension (PIOMI) -specifically b013e3 as young as 29 weeks GA based on Beckman’s protocol designed fo 182115a2a M/F = 4/6 infants as young and Control Group, n=9. modified Assessment Scale during a than those in the control group (t[16] = 1.77, p <
1-min trial of .05; scored higher on normal characteristics of the nutritive suck scale (U nonnutritive sucking and a
5-min trial of = 25, p = .08); were discharged from the hospital earlier, (t[16] = - nutritive sucking
2.4, p = .01); and gained more weight than their counterparts (t[16] = 1.49,
p = .07.
Number of
days from Infants in the NNOMT+
start to independent iMT group attained independent OF significantly earlier than oral feeding.
Overall transfer (%
controls (p<0.001) with shorter day intervals from start of OF to 3–5 daily volume taken/volume oral feedings.
Infants in both NNOMT
prescribed) Proficiency
and NNOMT+ iMT groups transitioned faster from 3–
(% volume taken at 5 min/volume
5 daily oral feedings to independent OF (p≤0.003).
prescribed) Rate of transfer over
Infants in all intervention
groups demonstrated a faster rate of oral feeding the entire skill maturation than the feeding (ml/min).
control group.
For feeding progression,
although there was a statistically significant decrease in transition from Feeding progression gavage to oral feedings for Length of hospital stay the PIOMI group of 5 days sooner, infant birth weight covariant eliminated the statistical significance. Although infants in the for this younger GA for M/F = 3/6 mins of finger stroking to cheeks (internal as 29 weeks GA based on Beckman’s protocol and modified for this and external), lips, gum Inclusion Criteria tongue, and younger GA for M/F = 3/6 mins of palate.
- Preterm infants, born finger stroking to cheeks (internal and between 26 and 29 weeks PMA Control
- Appropriate size for GA external), lips, gum tongue, and palate.
Provider’s hands inside
Control Provider’s hands inside isolette
isolette f • Clinically stable per medical staff, but 5 mins, not touching f5 mins, not touching infant. Each intervention infant. could be receiving oxygen per was provided f nasal Each intervention was cannula 7 consecutive days.
provided f cannula Level I Randomized
crossover design Intervention/Control, n=10
Control During control observation, infa was positioned in right side-lyin for 2
(crossover) M/F = not identified Inclusion Criteria •
Pickler, et al.
[29] doi:10.1016/j.a dnc.20040.05.0 Preterm infants, born prior to 32 Control weeks GA • No known minutes prior to
5 cognitive, neurologic, feeding wi no pacifier offered.
cardiovascular, gastrointestinal, or craniofacial disorders Level I RCT Intervention Group, n=49 Intervention 15 minutes perioral with 2 losses in follow-up resulting in 47 analyzed. M/F and intraor stimulation using = not identified Control Group, n=49. Control gloved finger a pacifier during Pimenta, et al.
[30] doi:10.2223/JPE M/F = not identified gavage until preterm infants started oral diet for Inclusion Criteria • Preterm infants, born between 26 and 32 feeding.
D.183
a period of at least weeks, 6 days GA • Adequate or small for GA
10 days. Control Sham procedure with no form of oral • Birth weight <1500 g PIOMI group were discharged 2.6 days sooner than the controls, this was not a statistically significant difference.
NNS and NS measured by
NS waves were smoother
and more regular than NNS waves. Time to onset a stretch sensitive chin and duration of the first non-nutritive suck burst were positively correlated strain gauge for measuring sucking rate with time to onset for the first nutritive suck burst (r and rhythm during feeding; effects of pre- = 0.79, P = 0.01) and (r =
0.94, P = 0.01).
Prefeeding NNS had no
feeding NNS on breathing
statistically significant effect on characteristics of measured with a nasal Thermistor, breathing or on any other characteristics of NS. Behavioral state during and on behavior state feedings and feeding before, during, and efficiency were not affected by prefeeding NNS after Length of hospital stay for infants in the experimental Length of hospital stay group was significantly lower than for the control and breastfeeding group, which was discharged 10.8 days later.
rate at discharge, 3- month and 6- month follow- The length of stay in the hospital for the control group was 52.37±19.51. The length of stay for the up.
experimental group was
41.81±17.7 (p=0.007). Fifty-nine infants (61.5%)
No malformations. Severe asphyxia, or presence of 3rd
stimulation during gavage feeding.
or 4th degree intracranial hemorrhage Intervention Oral support (The
first author) held the infant’s cheeks inward and forward Level I Randomized crossover design by placing her right Intervention/Control, n=20 ring finger on the infant’s left cheek (crossover) M/F = 7/13 and the thumb of the other hand on the infant’s opposite Yea Shwu, et al.
Inclusion Criteria • Preterm infants, born 25 to [31]
cheek to assist the infant in sealing the doi:10.5014/ajo
36 weeks GA • Allowed to take 15 ml by lips around the t.2010. 09031
nipple. Simultaneously, the
mouth per feeding, • Were inefficient feeders author placed her (i.e., unable to consume an average of 4 ml of feeding right little finger under the infant’s chin to stabilize the intake per min in a 5-min lower jaw.
feeding assessment) Control No oral support Level I RCT
Intervention 15 mins oral
Intervention Group, n=10
Younesian, et al.
stimulation according to [32]
M/F = 5/5
doi:10.5812/irc Control Group, n=10. M/F =
Beckman’s principles once per
mj.17( 5)2015.13515
5/5 day for 10 successive days 20-
Inclusion Criteria
40 mins prior to were breastfeeding at the time of hospital discharge,
31 (36.9%) at 3 months, and only 18 (20.5%) at 6 months of corrected age. At discharge, 46.9% of the control group and 76.5% of the experimental group were breastfeeding (p =
0.003). There were statistically significant differences between rates of breastfeeding at discharge (47 vs. 76%), 3 months (18 vs. 47%) (p = 0.003) and 6 months after discharge (10 vs. 27%) (p = 0.029).
For the intervention condition, statistical significance was noted in higher intake rate during Feeding performance the initial 5-min feeding period (p=0.046), lower % including duration, percentage leakage for initial 5-min (p=0.040), shorter feeding ingested, percentage duration (p=0.044), and higher intake rate for entire feeding (p=0.023) leakage, intake rake, than during control suck frequency, condition.
No statistical differences were noted in prescribed and mean volume ingested per volume consumed (p=0.11) or overall % of suck.
Physiological
leakage (p=0.84).
No significant differences
status was also assessed.
were noted in physiological status between conditions.
Number of
Statistical significance was
days to transition to SOF and FOF
achieved for SOF in Exp group over controls for 1 (P < 0. 001), 4 (P < 0.001), and 8 (P < 0.001) feedings (8 oral feedings per per day. Infants in Exp group were discharged day for 2 consecutive days), length ~1 week earlier than controls (p<0.05). Both
- of hospitalizatio n, and weight
- Control
- No stimulation other than routine
- GA
- • Appropriate size for GA
- (p=0.001) with no statistical difference between the groups. gain.
- • Fed by tube
- • Without chronic medical nursery care. complications such as bronchopulmonary dysplasia, intraventricular hemorrhage grades 3 and 4, periventricular leukomalacia, necrotizing enterocolitis, and congenital anomalies
- Transition to FOF was significantly shorter for
- NNS, OS, and NNS+OS than controls (all p<0.001). The
- Level I RCT
- Intervention Group 1, n=25.
- NNS+OS group attained independent oral feeding
- Intervention
- Group 1: (NNS) received 5 mins sucking on pacifier
- M/F = 11/14
- Intervention Group 2, n=27. at a significant lower weight (p=0.01) and days
- Transition from initial oral feeding
- M/F = 17/10
- Intervention Group 3, n=29. of life (p=0.004) than controls. These differences
- 7-8 times per day.
- M/F = 15/14 were not significant between the NNS group or
- OS group and the controls.
- Group 2: (OS) received 12 mins peri and intra-oral to FOF
- Control Group, n=27.
- Rate of milk
- Zhang, et al. [33]
- M/F = 14/13
- Inclusion Criteria
- • Preterm infants, born between 29 and 34 weeks
- All 3 intervention groups stroking protocol
- (Fucile’s program) transfer, proficiency doi:10.1097/PC had significantly greater once per day.
- Group 3: (NNS+OS)
- (volume taken during
- C.0000
- 000000000182 rate of transfer than controls (p<0.001). No
- GA
- • Weight appropriate for GA received combined first 5 mins)
- Total volume significant difference
- 12 min oral program and 3 mins
- • Apgar scores greater than among any of the 3 intervention groups for rate of transfer. Only the consumed
- Weight gain or equal to 3 at 1 min. and greater than or equal to 5 at
- NNS.
- Control
- Received standard
- Length of hospital stay
- 5 mins.
- • Received all feedings by
- NNS+OS group demonstrated a significantly improvement care only with no tube
- • No congenital anomalies or intervention. in proficiency over the developed chronic medical control group. No significant differences were noted in weight gain complications or length of stay among groups.
Table 2: Evidence Table for the Systematic Review of Best Practices for Oral Motor Stimulation to Improve Oral Feeding
There were 13 articles of Level I evidence and one of Level III evidence reviewed that provide supportive data of preterm infants [15]. There is also a high BOE/high strength of evidence for recommending intra-oral stimulation immediately following peri-oral stimulation prior to oral feeding of preterm infants.
Findings support that oral motor stimulation techniques, particularly those based on Beckman Oral Motor Intervention principles, can be used to promote a more organized suck-swallow-breathe coordination, improve latching, and increase suction strength and endurance, which may therefore lead to safe and successful oral feeding. The use of peri- and intra-oral pre-feeding stimulation was associated with p values showing statistically significant positive outcomes of shorter time to full oral feedings, increased volume intake, improved feeding efficiency, shorter length of hospital stays, and/or increased weight gain [25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36].
Before initiating oral stimulation with preterm infants in preparation for oral feeding, the infant should be physiologically stable, demonstrate hunger cues, and exhibit neurobehavioral states of being quiet and alert [10, 27, 29, 37]. Once aforementioned stability, cues, and states are achieved, it is recommended that the infant receives peri-oral stimulation to cheeks, upper and lower lips, and the jaw followed by intra-oral stimulation to internal cheeks, gums and [4, 9, 10].
Non-Nutritive Sucking
Twelve articles of Level I evidence provided support of the use of NNS as a pre-feeding intervention. According to LEGEND criteria, there are both a high BOE and high strength of evidence for recommending NNS as a preparatory method to promote successful feeding in preterm infants [15]. Non-nutritive sucking may increase strength, endurance, and suction and may help with organization of infants’ physiological and behavioral states as well as suck-swallow-breathe coordination [4, 5]. Multiple studies report that NNS using a pacifier or finger resulted in statistically significant improvement and moderate to large effect sizes in suck organization, coordination, and/or strength and endurance [3, 12, 10, 25, 28, 30, 33, 37]. NNS combined with oral stimulation also produced large positive effect sizes on oral feeding [22, 34]. One study by Pickler and Reyna [29] found no statistically significant effect of NNS on breathing characteristics or feeding efficiency. However, they did find that first NNS suck burst positively correlated with onset of first nutritional suck burst. The authors identified several limitations including small sample size and only two observations per infant. Fucile, Gisel & Lau [26] and Pimenta, et al. [30] found that preterm infants who received NNS in conjunction with oral stimulation were discharged earlier than those who did not receive NNS by a mean average of 5 days and 10.8 days respectively.
It is recommended that NNS be performed by placing a pacifier or gloved fifth finger in infant’s mouth during gavage feedings and 2-3 minutes prior to feeding following intra-oral stimulation [4, 10, 20, 26, 30, 37]. The finger should be placed at the midline, center of the palate, gently stroking the palate to elicit a suck [10]. If using a pacifier, a standard pacifier should be used rather than an orthodontic, flat, or bulb shaped pacifier [9].
Oral Support
Consistent with LEGEND criteria, there is a high BOE and high strength of evidence for providing oral support during oral feeding. Five articles of Level I evidence supported the provision of oral support during feeding of preterm infants to safely maximize oral intake [15]. According to this review of evidence, oral support is beneficial to infants who have poor suck performance, strength, and/or endurance, but once suck performance improves with the provision of NNS, oral support is no longer necessary. Oral support decreases fluid loss, provides cheek and jaw stability, and aids in coordination of deglutition [4, 24, 31, 33, 34]. It is recommended that oral support be provided during oral feeding to provide stability and ameliorate the sucking pattern by placing the middle finger under the chin providing pressure at the mandible, the thumb and index fingers compressing the cheeks toward lips, and the fifth digit compressing the floor of the oral cavity under the chin to reinforce the swallowing [4, 31, 34, 36].
Co-Interventions
Both the BOE and strength of evidence are high according to LEGEND criteria to recommend combining interventions in preparation for and during oral feeds of preterm infants [15]. The systematic review by Arvedson, et al. [34] and studies by Asadollahpour, et al. [22], Fucile, Gisel & Lau [26] and Zhang, et al. [33] provided level I evidence that when combined with oral support and/or NNS, oral stimulation resulted in statistically significant p values over oral stimulation alone for weight gain and transition to full oral feedings. Results from Fucile [4], Gaebler & Hanzlik [27], and Lau, Fucile & Gisel [28] reported that subjects who received touch therapies, such as stroking or massage along with oral stimulation gained significantly more weight and were discharged significantly earlier than those who received only one intervention or no intervention.
The infant must be monitored for apnea, oxygen desaturation, and bradycardia during oral stimulation. Lack of suck-swallow-breathe coordination, the effort required to actively respond to stimulation, and the infant’s immature body systems contribute to this risk [4, 10, 34]. These adverse events are uncommon during oral stimulation and did not result from oral stimulation during any of the studies examined.
Applicability Issues
There are initial costs to consider when implementing the recommended pre-feeding oral motor interventions, primarily related to personnel salaries. These include time to train the therapists and NICU nursing staff, time to provide intervention to the infants, and time for parent/caregiver training. No specialized equipment is needed to carry out these interventions. The pre-feeding oral motor methods and oral support recommendations can be incorporated into established or on-demand feeding schedules.
Implications for Practice
It should be noted that OT literature on preterm feeding is lacking in the area of preterm oral motor stimulation and feeding of preterm infants. There are minimal systematic reviews and meta-analyses on the topic. This systematic review adds to the available evidence in an effort to promote best practices. Benefits and risks related to the finding are identified below.
Benefits
Benefits of following these best practices of oral motor stimulation, NNS, and oral support include:
- improvement of suck-wallow-respiration coordination
- increased volume intake
- improvement in efficiency of feeding and decreased time required for oral feeding
- decreased time to transition to full oral feeding
- weight gain
- shorter length of hospital stay
Risks
Risks associate with these methods of oral motor stimulation, NNS, and oral support include:
Although the procedures for oral feeding, other than recommendations for oral support, are not included in this systematic review, any time oral feeding is introduced to a person with swallowing difficulties, there is the risk of aspiration.
The infant must be monitored for apnea, oxygen desaturation, and bradycardia during oral stimulation. Lack of suck-swallow-breathe coordination, the effort required to actively respond stimulation, and the infant’s immature body systems contribute to this risk. These adverse events are unlikely and did not result from oral stimulation during any of the studies examined.
The infant may experience physical discomfort during oral stimulation, although this risk is minimal and unlikely.
Limitations
There are a number of limitations to be considering when interpreting the findings of this systematic review. The author acknowledges that having only one person conduct this review was a limitation and could be considered a potential source of bias. Although multiple databases were thoroughly searched and results reviewed by the author, there is the chance that some studies may have been missed.
Only articles published in English were included in this review. Methodologies and outcome measures varied among the studies. Study duration, duration of interventions, and range of interventions also varied among studies. Because new studies on the topic are always being conducted, this review can only be considered current as of July 2015. Relevant articles published after this date was not examined.
Conclusion
The quality of the body of evidence regarding oral motor stimulation to improve oral feeding skills is high. Evidence suggests that pre-feeding readiness is essential to promote oral feeding. The infants’ physiological, oral-motor, and behavioral states must be organized for successful feeding to occur.
Strong evidence indicates that oral motor stimulation techniques can be used to promote a more organized suck-swallow-breathe coordination, improve latching, and increase suction strength and endurance, which may therefore lead to safe and successful oral feeding. The provision of appropriate oral stimulation and oral support leads to improvement of suck-swallow-breathe coordination, increased volume intake, improvement in efficiency of feeding and decreased time required to complete oral feeding, decreased time to transition to full oral feeding, weight gain, and shorter length of hospital stays. The culmination of these achievements and benefits leading to more successful feeders and earlier hospital discharge results in decreased medical costs to insurance companies and families.
Use of client-centered, evidence-based practice is important in the decision making process for interventions with high-risk infants. The results of this systematic review can assist occupational therapists and other professionals in the NICU in providing the most effective interventions for preterm infants to improve oral feeding outcomes. Conflicts of Interest Statement: The author declare that she has no significant competing financial, professional, or personal interests that might have influenced the performance or presentation of the work described in this manuscript. Acknowledgement: The author would like to acknowledge the James M. Anderson Center for Health Systems Excellence for allowing the use of their Let Evidence Guide Every New Decision Evidence (LEGEND) evaluation tools and resources to help guide evidence-based decision making.
References
-
Murphy SL, Mathews TJ, Martin JA, Minkovitz CS, Strobino DM, et al. (2017) Annual summary of vital statistics: 2013-2014. Pediatrics 139(6): 1-12.
-
Blackburn ST (2007) Maternal, fetal, & neonatal physiology: A clinical perspective. 3rd (Edn.), St. Louis, MO, Elsevier Science Saunders.
-
Arvedson J, Clark H, Lazarus C, Schooling T, Frymark T, et al. (2010) Evidence-based systematic review: Effects of oral motor interventions on feeding and swallowing in preterm infants. American Journal of Speech-Language Pathology 19(4): 321-340.
-
Fucile S (2008) Pre-feeding sensorimotor stimulation as an early intervention strategy to enhance oral feeding skills in preterm infants. McGill University, Canada, pp: 1-281.
-
Pickler R (2005) A model of feeding readiness for preterm infants. Neonatal Intensive Care 17(4): 31- 36.
-
Liu YL, Chen YL, Cheng I, Lin MI, Jow GM, et al. (2013) Early oral-motor management on feeding performance in premature neonates. J Formos Med Assoc 112 (3): 161-164.
-
Korth K, Rendell L (2015) Feeding intervention. In: Case- Smith J, OBrien JC, (Eds.), Occupational therapy for children, St Louis, MO, Mosby Elsevier, pp: 389-415.
-
Shaker CS (2012) Feed me only when I’m cueing: Moving away from a volume-driven culture in the NICU 25(3): 27-32.
-
Beckman DA (2008) Oral Motor Assessment and Intervention. Winter Park, Beckman FL, Associates, Inc.
-
Lessen BS (2008) Effect of oral stimulation on feeding progression in preterm infants. Doctoral dissertation, University of Illinois at Chicago. Chicago.
-
Neonatal Intensive Care Unit. Stanford Health Care.
-
Lessen BS (2011) Effect of the premature infant oral motor intervention on feeding progression and length of stay in preterm infants. Advances in Neonatal Care 11(2): 129-139.
-
American Occupational Therapy Association (2017) Guidelines for systematic reviews.
-
Sackett DL, Rosenberg WM, Muir Gray JA, Haynes RB, Richardson WS, et al. (1996) Evidence-based medicine: What it is and what it isn’t. BMJ 312(7023): 71-72.
-
Cincinnati Children's Hospital Medical Center (2017d) LEGEND (Let Evidence Guide Every New Decision) Evidence Evaluation System. Evidence-Based Decision Making Team, Cincinnati Children’s Hospital Medical Center. CCHMC.
-
Cincinnati Children's Hospital Medical Center (2017a) Evidence-based decision making. James M Anderson Center for Health Systems Excellence. CCHMC.
-
Cincinnati Children's Hospital Medical Center (2010) Evidence appraisal forms. James M Anderson Center for Health Systems Excellence. CCHMC.
-
Cincinnati Children's Hospital Medical Center (2017b) Grading a body of evidence. James M Anderson Center for Health Systems Excellence. CCHMC.
-
Cincinnati Children's Hospital Medical Center (2017c) Judging the strength of a recommendation. James M Anderson Center for Health Systems Excellence. CCHMC.
-
MG Dyck, Daley KJ (2002) Cannibalism of a Yearling Polar Bear (Ursus maritimus) at Churchill, Canada. Arctic Institute of North America 55(2): 190-192.
-
Moher DA, Liberati J, Tetzlaff, Altman DG (2009) The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. PLOS Medicine.
-
Asadollahpour F, Yadegari F, Soleimani F, Khalesi N (2015) The effects of non-nutritive sucking and pre- feeding oral stimulation on time to achieve independent oral feeding for preterm infants. Iranian Journal of Pediatrics 25(3): 1-5.
-
Bingham P, Ashikaga T, Abbasi S (2010) Prospective study of non-nutritive sucking and feeding skills in premature infants. Arch Dis Child Fetal Neonatal Ed 95(3): F194-F200.
-
Boiron M, Da Nobrega L, Roux S, Henrot A, Saliba E, et al. (2007) Effects of oral stimulation and oral support on non-nutritive sucking and feeding performance in preterm infants. Developmental Medicine & Child Neurology 49(6): 439-444.
-
Daley H, Kennedy C (2000) Meta analysis: Effects of interventions on premature infants feeding. J Perinat Neonatal Nurs 14(3): 62-77.
-
Fucile S, Gisel E, Lau C (2002) Oral stimulation accelerates the transition from tube to oral feeding in preterm infants. J Pediatr 141(2): 230-236.
-
Gaebler C, Hanzlik J (1996) The effects of a pre-feeding stimulation program on preterm infants. Am J Occup Ther 50(3): 184-192.
-
Lau C, Fucile S, Gisel E (2012) Impact of nonnutritive oral motor stimulation and infant massage therapy on oral feeding skills of preterm infants.Journal of Neonatal Perinatal Medicine 5(4): 311-317.
-
Pickler R, Reyna B (2004) Effects of non-nutritive sucking on nutritive sucking, breathing, and behavior during bottle feedings of preterm infants. Advances in Neonatal Care 4(4): 226-234.
-
Pimenta HP, Moreira MEL, Rocha AD, Gomes SC, Pinto LW, et al. (2008) Effects of non- nutritive sucking and oral stimulation on breastfeeding rates for preterm, low birth weight infants: A randomized clinical trial. Jornal de Pediatria 84(5): 423-427.
-
Yea Shwu H, Chyi Her L, Coster WJ, Bigsby R, Vergara E, et al. (2010) Effectiveness of cheek and jaw support to improve feeding performance of preterm infants. American Journal of Occupational Therapy 64(6): 886- 894.
-
Younesian S, Yadegari F, Soleimani F (2015) Impact of oral sensory motor stimulation on feeding performance, length of hospital stay, and weight gain of preterm infants in NICU. Iran Red Crescent Med J 17(7): 1-6.
-
Zhang Y, Lyu T, Hu X, Shi P, Cao Y, et al. (2014) Effect of nonnutritive sucking and oral stimulation on feeding performance in preterm infants: A randomized controlled trial. Pediatr Crit Care Med 15(7): 608-614.
-
Asadollahpour F, Yadegari F, Soleimani F, Khalesi N (2015) The Effects of Non-Nutritive Sucking and Pre- Feeding Oral Stimulation on Time to Achieve Independent Oral Feeding for Preterm Infants. Iran J Pediatr 25(3): 809
-
Bingham PM, Ashikaga T, Abbasi S (2008) Prospective study of non-nutritive sucking and feeding skills in premature infants. Arch Dis Child Fetal Neonatal Ed 95(3): 194-200.
-
Boiron M, Da Nobrega L, Roux S, Henrot A, Saliba E, et al. (2007) Effects of oral stimulation and oral support on non-nutritive sucking and feeding performance in preterm infants. Dev Med Child Neurol 49(6): 439- 444.
-
McCain G, Gartside P, Greenberg J, Lott J (2001) A feeding protocol for healthy preterm infants that shortens time to oral feeding. J Pediatr 139(3): 374-379.
- Electrolyte Considerations for Athletes
- Comprehensive Rehabilitation in Adults with Diabetic Peripheral Neuropathy: A Literature Review on Frequency, Intensity, and Duration Parameters
- Exercise Duration and Its Association with ADHD Symptom Severity in Children and Adolescents: A Parent-Reported Survey Study
- Adaptation of the Adult Neurophysiology of Pain Questionnaire for Use in Pediatrics
- A Non-Pharmacological Multidisciplinary Pain Program within a Hospital Wellness Program: A Mixed Methods Study
- The Effect of Frenkel's Exercise with PNF on Functional Reach in Stroke Survivors: A Randomized Control Trial