Tailored Functional Activities for Self-Reported Barriers to Return-to-Work in Cancer Survivors: A Proof-of-Concept Study
Purpose: Working-aged cancer survivors (18-64 years) are on average 1.4 times more likely to be unemployed after completing cancer treatments than are similar aged healthy cohorts. Given the personal and financial burdens on working-aged cancer survivors, improving return-to-work outcomes is necessary. There is sparse cancer-specific research in work-related functional interventions with self-reported measurable outcomes. Research of cancer-specific exercise programs targeting stamina and endurance show promise in improving return-to-work, though these programs do not specifically address work-related activities. A foundation of successful work outcomes is self-efficacy, which has not yet been researched as a primary endpoint in cancer-specific studies examining work-related interventions. This pilot study explored 1. the feasibility of adding tailored work-related functional activities to a cancer-specific exercise program, and 2. the value of using the Canadian Occupational Performance Measure (COPM)’s productivity section as an outcome to measure performance and satisfaction as aspects of work self-efficacy. Methods: This study utilized a single group pre-test/post-test design with working-aged cancer survivors (n=7). Outcome measures included work-related physical performance (lift tests), participation (adherence to the program - attendance and participation logs), and work self-efficacy satisfaction and performance (the COPM). Results: All participants completed their functional interventions. 6/7 participants completed pre- and post-lift tests, showing improvements at the post-lifting assessment. Participant perception of goal attainment (performance and satisfaction) showed clinically meaningful improvement (2-point change) in all participants. Conclusion: This pilot study demonstrates the feasibility of using the COPM as a tool for measuring performance and satisfaction. Embedding work-related functional activities into a physical exercise program provides a model for potential implementation and scalability.
Introduction
Background/Rationale
Working-aged cancer survivors (18-64 years) are 1.4 times more likely to be unemployed than comparatively healthy working-aged individuals [1]. As cancer treatments advance and patient outcomes improve, concern grows for cancer survivors who are reintegrating into work roles after completion of cancer-related medical treatment. Approximately 50% of all cancer- related return-to-work interventions in the United States of America result in failed work attempts, reflecting the complexity of work-related issues in cancer survivor populations, from both individual—referring to quality of life and productivity—and systemic—referring to economic—perspectives [2]. Unsuccessful work attempts and ongoing unemployment for working-aged cancer survivors are serious issues, as ongoing unemployment negatively impacts health, and imposes significant costs on the individual and society [3].
In response to the clinically identified yet unmet need for work-related support, a call has been issued for functional, work-related interventions to address the unique and individualized needs of cancer survivors [1]. Multiple research studies have suggested that cancer- specific vocational rehabilitation is warranted, with the caveat that more tailored approaches are needed [4]. A recent Cochrane Review found that no studies were led by occupational therapists and no studies focused on functional approaches to enhancing the return-to-work experience for cancer survivors [1]. To date, many work- related interventions for cancer survivors involve physical reconditioning, which may help address certain cancer-related sequelae such as fatigue, but typically do not include support for specific work-related concerns reported by cancer survivors [5]. A recent multidisciplinary trial that explored productivity and vocational outcomes following a combined intervention involving occupational counselling and physical exercise showed promise for return-to-work outcomes [6]. While functional restoration and work-specific programming in many other return-to-work contexts, such as musculoskeletal rehabilitation following physical injury or trauma, have been successful in facilitating positive return-to-work outcomes, cancer-specific return-to-work programming has not yet been extensively explored [1, 4, 7]. Canadian and American guidelines for managing side effects of cancer have been developed, including protocols for activity engagement, but work-related protocols (referring to the ability to work) remain largely absent in these publications [4, 8]. Further, limited interdisciplinary healthcare research on the association between functional outcomes and work self-efficacy has been conducted. Work self-efficacy, defined as a belief in one’s ability to work, is known to be foundational both in goal development and in outcome achievement [9]; therefore, use of work self-efficacy as an outcome may be a beneficial means of engaging an individual in work- related rehabilitation, and a useful marker of success in return-to-work related programming. As a first step, this proof-of-concept pilot study made use of the opportunity of an existing cancer-specific physical exercise program as a platform in which to embed a functional intervention, and included the Canadian Occupational Performance Measure (COPM)’s productivity section as a means of developing and measuring the tailored approach [10].
Aims/Objectives
This study explored the feasibility of implementing tailored functional activities into a physical exercise program for cancer survivors who were transitioning to their previous vocations after being off work due to cancer treatment. Feasibility-related issues of interest included the following:
• At the participant level: The extra time commitment necessary for completion of the additional work- related functional activities;
• At the level of the occupational therapist: The additional time needed to create and administer the program;
• At the level of the institution: The environmental (location and equipment) and additional time requirements necessary to accommodate both the pilot study and the exercise program;
• At the level of the assessments: The feasibility of using of performance-based lift tests for the examination of functional (i.e. physical activity) outcomes, and the use of the COPM—a tailored individualized assessment tool-for the examination of participant-reported work self-efficacy in performance and satisfaction ratings.
Context
This study was conducted within the context of a multi-site, community-based exercise study for adult cancer survivors, titled the Alberta Cancer Exercise (ACE) hybrid effectiveness implementation study [11]. The ACE study involves a 12-week community-based exercise program, with focus on full body exercise to optimize quality of life outcomes in cancer survivors. During the 12-week program, participants attend exercise sessions twice per week, for approximately 1-1.5 hours per session. The physical exercises are progressed as appropriate over the 12-week intervention by the research team—which includes kinesiologists, certified exercise physiologists and physiotherapists (referred to hereafter as ACE exercise specialists). In its current form, the ACE study neither addresses work-related concerns nor goals as part of the program.
The pilot study took place during the fall of 2018 in Edmonton, Alberta, Canada across two community sites—a cancer rehabilitation clinic and a cancer-specific community—wellness centre—with the intervention occurring during the final 7-weeks of the ACE exercise program (with pre and post-intervention testing on week 6 and after week 12, respectively).
Methods
Study Design
This study used a proof-of-concept (PoC) pre-test/post-test design. PoC designs are used to demonstrate feasibility and verify the practical potential of a concept as a means for decision making and problem solving across interdisciplinary research [12]. The pre-test/post-test design was chosen, as it allowed for exploration of the effects of embedding work-related activities into an existing exercise program. As each participant’s intervention was tailored to his/her vocation and work-related goals, the results before and after the intervention could be compared at the level of the individual prior to examination of the group’s overall performance.
Ethics and Consent
Informed written consent was obtained. The ACE study and the present sub-study received scientific and ethical approval from the Health Research Ethics Board of Alberta: Cancer Committee.
Sample and Recruitment
Participants were selected based on their baseline assessments in the ACE study. This pilot study focused on functional work-related activities to potentially improve work self-efficacy of cancer survivors in general, and thus, eligibility included all cancer types. Based on normative data for pilot studies of a similar nature, we aimed for a minimum sample of 5-10 participants.
Inclusion criteria included:
• Current ACE participant aged 18-64 years, whose demographic data indicated previous vocation, with intent to return to their previous work.
• Score of 4 or higher on the item “Tiredness” on the Edmonton Symptom Assessment Scale (ESAS) [13]; or, indicating a level of fatigue described as “somewhat” or higher on the FACT-Fatigue subscale question “I feel fatigued” [14].
• Identifying issues related to “work” on the Canadian Problem Checklist (CPC) [15].
• Attending an ACE site offering a group personal training exercise format.
Participants were excluded if there were any changes related to disease or health status that required active treatment, or if they were currently working at their previous level of vocational engagement.
Eligible ACE participants were randomly selected to participate in this optional pilot sub-study. ACE research coordinators contacted potentially eligible participants. Participants were informed that this pilot would be a supplement to their prescribed ACE exercise program, and that work-related activities would be carried out.
concurrently with their exercise sessions. Those who expressed interest in taking part were then telephoned by a research assistant to answer any further questions about the optional study, and to set up the baseline assessment session.
Outcome Measures
Information about each participant was collected from the following sources: (1) ACE Assessments for baseline feasibility; (2) Participant attendance and participation logs;
(3) Lift tests, for determination of physical work-related outcomes over time [16];
(4) COPM, as a measure of work self-efficacy through scores of task importance, satisfaction, and performance over time [10].
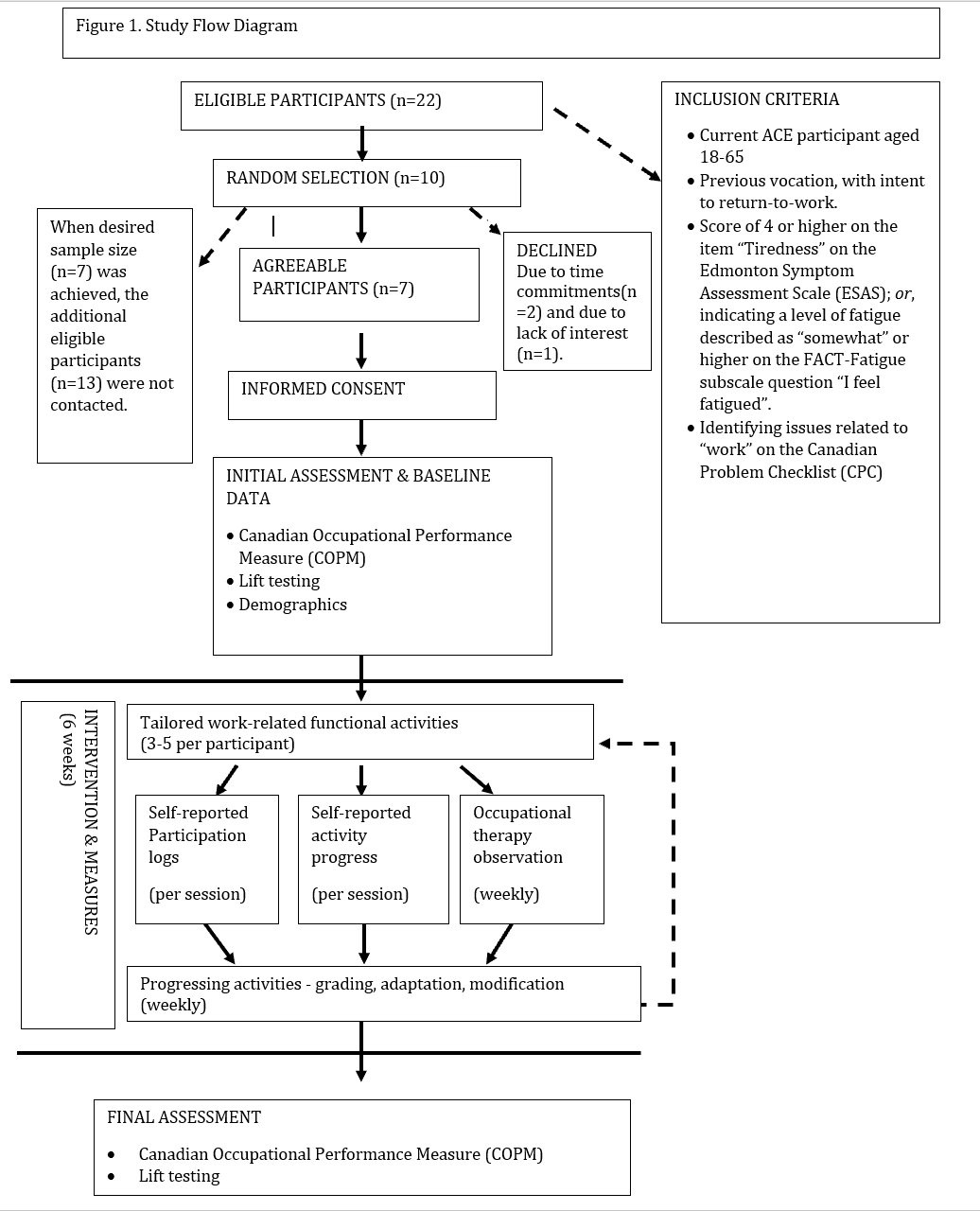
Thus, endpoints of measure included work-related physical performance (lift tests), participation (adherence to the program – attendance and participation logs), and satisfaction and performance as components of work self- efficacy (COPM). Figure 1 (Study Flow Diagram) illustrates the measures in context of recruitment and study timeline.
Information about the feasibility of the intervention was collected through feedback from ACE exercise specialists, time records of the occupational therapist, and timetabling and scheduling information from the sessions at the venue.
ACE Assessments for Baseline Data
Participant demographic and medical information provided to the parent ACE study was accessible for this pilot. Vocational history was gathered as part of the COPM. Employer and company details were not used as part of the collected data in the study. In order to protect the identities of all participants, each participant was given a code number, and all identifiable data were excluded/removed from study-related documentation.
Feasibility
Feasibility at the level of the participant was measured through adherence and engagement. Participant attendance for both the exercise programming and the tailored, functional work-related activities were recorded for each session and collected weekly to review. Since ease of implementation was an important consideration for embedding functional activities within a physical exercise program, the time commitment and attendance records were significant measures in ensuring that participants were not burdened by too many activities and that the added activities did not result in negative impact or excessive physical overload on the participants.
Feasibility at the level of the occupational therapist was measured by recording the time required for developing and implementing the additional activities, and the timing and requirements for implementing the intervention for each of the seven participants. Again, with ease of implementation being an important consideration for embedding functional activities within a physical exercise program, it was important to quantify the impact of the additional workload.
Feasibility at the level of the institution was measured through our ability to utilize existing gym space and equipment, and to schedule and carry out the intervention. The feasibility of timing and scheduling of the activities was measured through feedback from the participants and ACE exercise specialists, time-tabling for the shared used of space, and participation logs indicating successful completion of session activities. Feasibility at the level of the assessments was measured by evaluating the findings of study outcomes used for individualized interventions, which included lift tests and the COPM, described below.
Lift Tests
To compare physical work-related outcomes, lift tests were utilized, as they have been found reliable and are moderately associated with return-to-work outcomes in other health-compromised populations [17, 18, 19]. Lift tests involved three separate tests of lifting and carrying a weighted crate: (1) lifting a weighted crate from waist height to floor; (2) lifting a weighted crate from waist height to shoulder height; (3) carrying a weighted crate at waist level while walking a short distance (10m). The starting weight category was determined based on job requirements and on whether the participants were able to statically lift the expected amount for the weighted crate. Performance on the lift tests was categorized into limited, light, medium, or heavy, based on the National Occupational Classification (NOC) database job descriptions and participant-reported work tasks [20]. Weight categories were divided into limited 0-5 kg (0-11 lbs.), light 5-10 kg (11-22 lbs.), medium 10-20 kg (22-44 lbs.), and heavy >20kg (>40 lbs.). Less physical vocations (sedentary roles) were considered in a limited to light weight category. Moderate physical vocations were considered in the medium category. High physical vocations were considered in a heavy category. Details of vocation-specific physical demands can be found in the NOC database. Lift tests were progressed incrementally to either the maximum as reported or demonstrated by the participant (i.e. psychophysical endpoint) or the maximum ability required for the vocation [21, 22]. The test was stopped if the participant had observable signs of maximal physical effort which included groaning, wincing, and/or poor posture/ lift form [22]. An improvement of 5kg per week in lifting, and/or progress to a higher NOC lift category can be considered meaningful improvements in lift testing [23]; for this study, the NOC category change was used to measure a meaningful improvement.
Canadian Occupational Performance Measure (COPM)
The COPM scores were used to measure work self- efficacy through the combined respective pre- and post- intervention individual performance and satisfaction ratings [24]. The COPM is a standardized individualized assessment, which has a section devoted to productivity (work-related activities). Each participant ranked his/her most important productivity (work-related) concerns on a scale of one (least important) to ten (most important); the highest ranked three-to-five activities were used in the subsequent aspects of the COPM assessment, and in the development of the tailored, functional work-related activities.
Then, on a ten-point scale, each participant rated his/her current level of performance and satisfaction for each of the selected items. Participants could rate importance, performance, and satisfaction as low as zero an as high as ten respectively. To be used in the intervention, activities could not have initial performance ratings of 10/10, as there would have been no goal to achieve. The maximum score a participant could begin with is performance at 9/10 and satisfaction at 9/10. The performance and satisfaction ratings reported by each participant at the end of the program were compared to his/her initial scores to better understand changes in individual perceived work self-efficacy in performance and satisfaction (i.e. perceived task performance and level of satisfaction) over time. A positive change of 2 points on each COPM category of performance and satisfaction is considered a meaningful improvement [24].
Procedures
The baseline session took place during week six of the ACE program. In this initial session, participants met with an occupational therapist and study interventions and outcomes were explained. The COPM-productivity section was completed and a custom protocol lift test was performed [24, 16].
Following this initial session, the occupational therapist developed between three and five supplemental, tailored, functional, work-related activities based on the COPM and lift test results. Consideration of the equipment and resources available, such as the range in dumbbell or sandbag weights available at each site, was required in developing the activities (see Limitations for further details). These new activities were then added to the participant’s ACE exercises, to be performed during weeks seven through twelve of the ACE program. Each of the supplemental functional activities was designed to be integrated into the participant’s ACE programming and to require 5-15 minutes to complete (about 25 minutes in total for all activities).
The occupational therapist progressed the functional activities weekly based on both observations of performance and participant self-report. Grading, modification, and adaptation of the activities followed the “just right” principle of occupational therapy practice [25]. As a participant demonstrated ease in task completion and/or reported manageable task completion, the activity was progressed to provide a greater challenge with the aim of eventually reaching the determined end goal [25]. The functional activities made use of the gym equipment available in the ACE study—such as weighted wheels, sandbags, treadmills, balance equipment, stairs—to simulate the functional, physical, work-related task demands. Some examples of the gym-equipment used in real-work functional contexts include the following:
- Use of a weighted wheel in a seated position to practice driving a vehicle, wherein the weighted wheel simulates the steering wheel of a vehicle.
- Use of weighted sandbags to practice carrying babies and children in a nursing context.
- Use of incline and front bars on a treadmill to simulate pushing objects, such as a hospital bed.
The final post-intervention session involved completing the COPM and repeating the lift testing. Figure 1 is a diagram depicting the study flow.
Analysis
Feasibility
Participant intervention adherence measures were analysed descriptively through participation and attendance logs, and as well as the number of weekly progressions of activities. The occupational therapist’s time commitment was analysed descriptively, as were the environment, equipment and resources needs at each exercise location. Finally, the feasibility of assessments were analysed descriptively through the work-related outcomes.
Work Self-Efficacy Performance and Satisfaction
Performance and satisfaction as measures of work self-efficacy were recorded through the COPM performance and satisfaction scores over time. These scores were hand calculated as per the assessment guidelines, to compare improvements specific to important vocational issues reported by participants.
Results
Of a total of 68 ACE participants in the cohort, 22 ACE participants were deemed eligible for the study, 10 participants were randomly selected to participate and seven agreed to take part. Two potential participants declined due to the increased time commitments of the pilot study and one potential participant declined due to lack of interest. Of the seven participants who took part in this pilot study, two were males and five were females, with five involved in healthcare vocations (Table 1).
| Participant Characteristics (n=7) | |||
|---|---|---|---|
| Variable | Value | ||
| Age in years: Mean (Min-Max) | 44.3 (26-62) | ||
| Sex | |||
| Number of Females | 5 | ||
| Number of Males | 2 | ||
| Employment Status | |||
| Number returning to partial work within 3 months prior to pilot-study commencing | 2 | ||
| Number returning to work/partial work during pilot-study | 2 | ||
| Number intending to return to work/partial work 1 month post-pilot study | 1 | ||
| Number not intending to return to work during study or 1 month post- study | 2 | ||
| Time Since Diagnosis | |||
| Within the first year | 4 | ||
| > 1 year | 3 | ||
| Vocations (National Occupational Classification job description code) | |||
| Acute care nurse (3152) | 1 | ||
| Clinic nurse coordinator (3151) | 1 | ||
| Neonatal nurse (3152) | 1 | ||
| Operating room nurse (3152) | 1 | ||
| Paramedic (3234) | 1 | ||
| School teacher (4142) | 1 | ||
| Yoga instructor (5254) | 1 |
Table 1: Participant Characteristics.
Feasibility
At the participant level, feasibility was demonstrated by adherence and completion rates. All participants (n=7) completing the initial and final COPM sessions, and 6/7 completed the initial and final lift tests. One participant sustained an injury unrelated to the study, and was unable to complete the final lift test. There were no drop- outs during the study. At baseline, each participant was able to identify his/her most important issues regarding workability through the COPM, and rate these issues in terms of his/her performance and satisfaction. All participants attended 100% of the sessions throughout the 6-week intervention. The overall time for functional work-related activities per session was approximately 25 minutes. The time commitment for participants was deemed acceptable based on participant attendance and participation. ACE exercise specialist feedback included no reported issues with the additional time commitments for this study, and the neutral impact of the additional activities on symptoms and performance of the prescribed ACE program.
Table 2 depicts the vocational concerns and functional interventions, as well as the time commitments for activities, equipment and space used, and total number of times that activities were progressed. As seen in Table 2, the occupational therapist progressed each participant’s activities at least three times during the 6-week intervention.
At the level of the occupational therapist, feasibility was demonstrated through the ability to use the participant-driven COPM data to generate functional, work-related activities for the intervention. The time commitments were deemed feasible given that one occupational therapist was able to develop the interventions and prescribe the activities within 21 hours (approximately 3 hours per participant) prior to the interventions, observe and adapt interventions at a commitment of 5 hours per week, all within the timeframe of the study (7 weeks).
At the level of the institution, managing equipment and space-usage was deemed feasible, and made possible through time-tabling and clear communication.
| Vocation | Work- related/COPM concerns* | Intervention goals | Activities | Equipment used | Total number | ||
|---|---|---|---|---|---|---|---|
| of times | |||||||
| activities were | |||||||
| progressed | |||||||
| during 6 week | |||||||
| intervention | |||||||
| (weekly basis) | |||||||
| Acute care nurse | Difficulty completing shift at work due to fatigue and limited stamina | Tolerate 2.5 hours of sustained activities with only micro (less than 3 minute) breaks. | -On ACE session days, progressively reduce breaks and duration of breaks in session; grade activity to eventually include the hour prior to ACE and ½ hour following ACE to simulate a shift and break timeframe. Education and practice of mini and microbreaks (of less than 3 minutes) | - N/A | 5x | ||
| Difficulty managing post- operative care for patients second to deconditioning (dynamic standing, 20 minutes) | -To successfully complete ACE free weight exercises in standing without a break (20 minutes) -To successfully simulate 20 minutes of patient-care in standing at side of plinth | -Using resistance bands and light free weights for shoulder/upper extremity movements; focus on body mechanics for dynamic standing including posture and weight shift. | -Free weights (light) Resistance band -Plinth/ adjustable height rolling table |
| Difficulty moving patient beds in 20m hallway (push/pull) | To successfully push weighted cart/plinth in hallway 10m | -Progress from treadmill inclined to treadmill with incline and forward push motion for 2 minutes. -Progress from pushing plinth unweighted in hallway to plinth in hallway with added weights to plinth to incrementally simulate patient in hospital bed, to reach 20m. | -Treadmill -Plinth -Hallway -Weights | ||
|---|---|---|---|---|---|
| Clinic nurse coordinator | Limited stamina walking to and from work (20 min, 2x daily) | Successfully walk for 20 minutes 2x daily at a moderate pace | -Progressive walking performed twice in a session, either on a treadmill or outside, for 20 minutes each time. | -Treadmill -Hallway -Outdoor space | 4x |
| Difficulty with picking objects off of floor | Successfully manage lunges to lift light object from floor 3x in session | -Progressive review of lunges and transfers to safely pick up object on floor | -Paper and light objects placed on floor -Mat | ||
| Difficulties lifting and moving supplies (10lbs or less) from waist height to higher or lower and shifting files from one counter to another | Successfully move weighted crate (less than 10lbs) from floor to waist and waist to shoulder height 3x in session. Successful drag then push of crate for 1 metre each, along counter. | -Progress with weights in crate and duration of activity to reach goals, -Review of body mechanics and lift techniques in sessions. | -Crate -Light weights (1- 10lbs) Countertop space Shelf space | ||
| Neonatal nurse | Unable to manage fast movements at work, i.e. Fast paced walking (approx. 30 seconds, 3x shift) | To complete treadmill sprint walks 3x for 30 seconds each while walking on treadmill | -Progress speed and duration of fast-paced walking up to goal of 30 seconds | -Treadmill -Timer | 3x |
| Unable to hold a baby for 20 minutes | To carry a weighted sandbag of 8lbs during walking activity for 20 minutes | -Progress with use and duration of weight to simulate baby carry | -Treadmill -3-10lb sandbag weights | ||
| Difficulty transferring babies from incubator to beds (lift and carry) | Successfully complete 3 simulated transfers from incubator to bed in standing position | -Sandbag weight (8lbs) transfer using weight shift of 8lbs from chest height crate to waist height plinth; progress the weight of the sandbag and number of repetitions | -Sandbag weights (5- 10lbs) -Plinth -Table with crate | ||
| Difficulty multitasking walking while completing other work tasks, such as carrying a baby while walking, or | Complete 10 minutes of moderate paced walking while moving weighted objects across midline on inclined treadmill | -Progress activity to include light weights transferred across the midline of the body. Alternate this task with the fast-paced walking task. | -Treadmill -Light weights -Timer |
moving IV poles.
To successfully simulate scrubbing in, which includes wearing operating room garments and cleaning equipment for 15 minutes Difficulty tolerating scrubbing in prior to surgeries second to fatigue Throughout 1 hour of ACE session, will successfully manage exercise and activities without a seated break (1 hour standing/dynamic mobility) Difficulty standing/walking during surgery of more than 1 hour Operating room nurse Unable to manage cart sort (high/low movements, including squatting) to set up station.
Successfully complete 10 minute cart sort and set up simulation Successfully complete 20 minutes of walking with completion of simulated plinth/cart push using treadmill at incline 3x for 2 minutes.
Unable to push/pull cart or plinth due to deconditioning To self-manage approx. 2 foot jump at rear of ambulance 3x in 1 hour without fatiguing Difficulty entering and exiting back of ambulance Paramedic -Progress activity with static and dynamic standing at the sink to reach 10 minutes of simulated scrubbing in. Task includes washing objects in the sink and turning to place on table behind. -Simulated operating bed set up for 5 minutes with crossbody movements to place equipment properly for simulated surgery.
-Sink -Hospital gown, mask, and gloves -Objects in sink, including cups and sponges -Table at waist height -Plinth -Simulated operating equipment, including small pens and rulers -Use of treadmill and ACE exercise activities to progress to 1 hour of continuous activity. Grade by reducing break times and frequency of breaks.
-N/A
4x -Progress with lunges, squats, high-low movements in ACE exercise program for use in cart sort and set up. -Simulated cart to include items stacked in progressively challenging ways (i.e. All objects on lowest shelf to start) -Rolling cart -Plinth -Simulated operating equipment, including small pens, rulers, water bottles, light sandbag weights for fluid bags etc.
-Progress walking slowly on treadmill, to moderate- paced walking. Increase repetitions and duration of incline, and progressively increase level of incline.
-Treadmill -Timer -Lunging on stairs over 3 stair spread Jumping on mat, progressing to jumping from higher step to base of stairs (3 stair spread). -Leaping over target object -Access to Stairs -Access to hallway Exercise mat -Object for target (i.e. Tape marking “x”)
3x
To self-manage lifting a 40lb sandbag weight from floor to waist level with 30 second hold (simulating a child, based on weights available) Difficulty lifting patients (with a partner) from floor to waist level To self-manage 2x simulated sliding transfers of 40lb weighted sandbag in a session with proper body mechanics.
Difficulty transferring patients from bed to stretcher To complete accelerated paced climb and descend of 26 stairs; to consistently run stairs for 2 minutes in a session without fatiguing.
Unable to manage 2 flights of stairs in an emergency call Unable to lift/carry boxes with supplies (approx. 20lbs) for any length of time To complete 5 minutes moderate- paced walking on a treadmill with carry of weighted objects (up to 20lbs).
Difficulty with balance/cross body movements to reach and place objects in the room To self-manage balance tasks with object placement for 2 minutes School teacher Difficulty mobilizing while multitasking, such as walking and delivering student papers, second to proprioceptive changes post- cancer diagnosis and treatment To complete 10 minutes of moderate-paced walking on a treadmill with cross body object transfer Unable to stand up from floor level, either after picking up small objects from the floor or from To complete 5 repeated floor-to- stand transfers, and 1 sustained (more than 10 minutes) floor-to-stand - Progressive lifting of sandbag weight in carrier bag (starting with 10lbs and progressing to maximum weight available) -Progressive timing of lift and lower to include up to 30 second hold at maximum -Cylindrical sandbag weights with carrier bag -Clock or timer -Light to medium -Stretch resistance bands, tied to hold body in position -Plinth/table at waist height -Sandbag weights in carrier bag -Simulation of sliding transfer using sandbag weight, with use resistance bands at legs and arms to cue for body mechanics, with progressive reduction in physical cues.
-Progressive increase in stair climb and speed over sessions - Stairs -Timer
-While walking on treadmill, using either weighted sandbag, 1 free weight, or small crate to simulate sustained carrying task in ambulation -Treadmill -Free weight (5-10lbs) -Sandbag weight (20lbs) -Small crate -While standing in balance postures for ACE program, adjust activity to include grasp and place of school objects for simulated balance and crossbody movements; objects provided and placed at varied heights -School objects, including: water bottles, pens, binders, books, pages in a folder
3x -Objects, including: light free weight (5lbs max), school-type objects (folders, binders, books), weight sandbag (max 10lbs) -While walking on treadmill, objects placed on left and right sides of treadmill, for grasp and place tasks.
-Low squats with object pick up; lunges and floor-to- stand lunge transfers with object pick up -After floor/mat work for ACE, practice lunge to stand - Mat -Objects for pick up (i.e. Books, small ball, water bottle) seated on the floor transfer To complete 5 minutes of sustained filing simulation tasks, including object placement waist to shoulder to level.
Unable to complete filing for paper items at or above shoulder level.
Difficulty with seated tolerance in driving and floor sitting, more than 5 minutes To tolerate 15 minutes of dynamic sitting either in chair or floor Difficulty and instability with transfers from the floor to standing To successfully complete 3 floor- to- stand lunge transfers in 1 hour -Low lunge transfer progression -Stair lunges Yoga instructor To successfully tolerate static squatted hold for > 2 minutes Prolonged squatting more than 2 minutes Weighted carry and drag to position cushions for classes (approx. 10lbs each, approx. 20x per session) To successfully drag/carry weighted objects of 10lbs 20x in session -At filing cabinet, using papers, 1lb weights and files, placing objects into cabinets of varying levels of height (floor to shoulder) -Filing cabinet or tall shelf 1lb weight -Papers/files -ACE upper extremity free weight and shoulder exercises completed in seated, with directions to calf pump and shoulder check to simulate a car (approx. 15 minutes) -Seated cool down at end of session on the floor in modified cross legged positions (approx. 5 minutes) -Free weights -Chair -Timer -Mat -Towel rolls for modified floor sit positions as need be
4x -Hallway staircase (3 steps) -Mat
-Squat-to-stand transfers, review of weight shift -Progressive squat hold x2 minutes, beginning with 20 second, 6x.
-Mat -Simulation of yoga cushions using 10lb weight sandbag in pillow and pillowcase; drag 5m, carry 5m in session, 2 sets (beginning and end of ACE program), 10 repetitions -Pillow -Pillowcase 10 sandbag weight
- *As derived from the Canadian Occupational Performance Measure (COPM) results; see Table 3 for details.
- Work-Related Outcomes initial measure: see Measures section for NOC
Table 4: Vocational Concerns and Functional Interventions.
Table 3 describes the outcomes of the lift tests. Three of 7 participants initially lifted the required amount of weight for their personal job description, whereas 4/7 participants initially could lift 1-2 weight categories below their appropriate work-related weight category (i.e. a participant requiring middle weight category of lifting for their work, but could only lift light weight on their
| Particip ant vocation (n=7) | Required physical lifting ability (NOC) | Lift test initial | Lift test comple tion | COPM areas of productive importance* | COPM initial performan ce rating | COPM | COPM initial satisfacti on rating | COPM final satisfactio n rating | ||
|---|---|---|---|---|---|---|---|---|---|---|
| final | ||||||||||
| perform | ||||||||||
| ance | ||||||||||
| rating | ||||||||||
| Acute care nurse | Heavy | Middle | Heavy | Difficulty completing shift at work due to fatigue and limited stamina | 5/10 | 7/10 | 4/10 | 2/10 | ||
| Difficulty managing post- operative care for patients second to deconditioning (dynamic standing, 20 minutes) | 4/10 | 6/10 | 3/10 | 5/10 | ||||||
| Difficulty moving patient beds in 20m hallway (push/pull) | 5/10 | 7/10 | 2/10 | 4/10 | ||||||
| Pre- and Post- intervention scores (sum of ratings / number of issues) | 14/3 = 4.7 | 20/3= 6.7 | 7/3 = 2.3 | 13/3 = 4.3 | ||||||
| OVERALL COPM CHANGE SCORES (final-initial) | Performance: 2 | Performance: 2 | ||||||||
| Clinic nurse coordina tor | Light | Light (with difficul ty) | Light | Limited stamina walking to and from work (20 min, 2x daily) | 5/10 | 9/10 | 1/10 | 9/10 | ||
| Difficulty with picking objects off of floor | 4/10 | 6/10 | 2/10 | 4/10 | ||||||
| Difficulties lifting and moving supplies (10lbs or less) from waist height to higher or lower and shifting files from one counter to another | 3/10 | 5/10 | 2/10 | 4/10 | ||||||
| Pre- and Post- intervention scores (sum of ratings / number of issues) | 12/3 = 4 | 20/3= 6.7 | 5/3 = 1.7 | 17/3 = 5.7 | ||||||
| OVERALL COPM CHANGE SCORES (final-initial) | Performance: 2.7 | Satisfaction: 4 | ||||||||
| Neonatal nurse | Middle | Middle | Middle | Unable to manage fast movements at work; i.e. Fast paced walking (approx. 30 seconds, 3x shift) | 5/10 | 7/10 | 2/10 | 9/10 | ||
| Unable to hold a baby for 20 minutes | 3/10 | 7/10 | 1/10 | 9/10 | ||||||
| Difficulty transferring babies from incubator to beds (lift and carry) | 3/10 | 6/10 | 3/10 | 8/10 |
Table 5: Table 3: Outcome Measures per Participant Lift Test and Canadian Occupational Performance Measure ratings.
| Difficulty multitasking walking while completing other work tasks, such as carrying a baby while walking, or moving IV poles. | 2/10 | 8/10 | 2/10 | 10/10 | ||||
|---|---|---|---|---|---|---|---|---|
| Pre- and Post- intervention scores (sum of ratings / number of issues) | 13/4= 3.3 | 28/4= 7 | 8/4/=2 | 36/4= 9 | ||||
| OVERALL COPM CHANGE SCORES (final-initial) | Performance: 3.7 | Satisfaction: 7 | ||||||
| Operatin g room nurse | Middle | light | Middle | Difficulty tolerating scrubbing-in prior to surgeries second to fatigue | 4/10 | 6/10 | 1/10 | 3/10 |
| Difficulty standing/walking during surgery of more than 1 hour | 3/10 | 7/10 | 2/10 | 4/10 | ||||
| Unable to manage cart sort (high/low movements, including squatting) to set up station. | 4/10 | 8/10 | 5/10 | 5/10 | ||||
| Unable to push/pull cart or plinth due to deconditioning. | 2/10 | 7/10 | 1/10 | 5/10 | ||||
| Pre- and Post- intervention scores (sum of ratings / number of issues) | 13/4= 3 | 28/4= 7 | 9/4/= 2.3 | 17/4= 4.3 | ||||
| OVERALL COPM CHANGE SCORES (final-initial) | Performance: 4 | Satisfaction: 2 | ||||||
| Paramed ic | Heavy | Light | Middle | Difficulty entering and exiting back of ambulance | 5/10 | 8/10 | 3/10 | 8/10 |
| Difficulty lifting patients (with a partner) from floor to waist level | 6/10 | 8/10 | 4/10 | 8/10 | ||||
| Difficulty transferring patients from bed to stretcher | 4/10 | 6/10 | 2/10 | 6/10 | ||||
| Unable to manage 2 flights of stairs in an emergency call | 3/10 | 7/10 | 4/10 | 7/10 | ||||
| Pre- and Post- intervention scores (sum of ratings / number of issues) | 18/4=4.5 | 29/4=7.3 | 13/4=3.3 | 29/4=7.3 | ||||
| OVERALL COPM CHANGE SCORES (final-initial) | Performance: 2.8 | Satisfaction: 4 | ||||||
| School teacher | Middle | Light | Middle | Unable to lift/carry boxes with supplies (approx. 20lbs) for any length of time | 7/10 | 10/10 | 7/10 | 10/10 |
| Difficulty with balance/cross body movements to reach and place objects in the room | 6/10 | 8/10 | 3/10 | 6/10 | ||||
| Difficulty mobilizing while multitasking, such as walking and delivering student papers, second to proprioceptive changes post- cancer diagnosis and treatment | 5/10 | 8/10 | 2/10 | 7/10 | ||||
| Unable to stand up from floor level, either after picking up small objects from the floor or from seated on the floor | 5/10 | 9/10 | 7/10 | 9/10 | ||||
| Unable to complete filing for paper items at or above shoulder level. | 5/10 | 9/10 | 2/10 | 9/10 | ||||
| Pre- and Post- intervention scores (sum of ratings / number of issues) | 28.5=5.6 | 43/5=8.6 | 21/5=4.2 | 41/5=8.2 | ||||
| OVERALL COPM CHANGE SCORES (final-initial) | Performance: 3.7 | Satisfaction: 4 | ||||||
| Yoga instructo r | Middle | Middle | N/A | Difficulty with seated tolerance in driving and floor sitting, more than 5 minutes | 5/10 | 8/10 | 3/10 | 10/10 |
| Difficulty and instability with transfers from the floor to standing | 5/10 | 7/10 | 3/10 | 8/10 | ||||
| Prolonged squatting more than 2 minutes | 3/10 | 8/10 | 2/10 | 8/10 | ||||
| Weighted carry and drag to position cushions for | 7/10 | 9/10 | 4/10 | 8/10 | ||||
| Pre- and Post- intervention scores (sum of ratings / number of issues) | 20/4= 5 | 32/4= 8 | 12/4= 3 | 34/4= 8.5 | ||||
| OVERALL COPM CHANGE SCORES (final-initial) | Performance: 3 | Satisfaction: 5.5 |
Table 6: Table 3: Outcome Measures per Participant Lift Test and Canadian Occupational Performance Measure ratings.
*Used to develop the interventions/activities described in Table 2. Table 3: Outcome Measures per Participant Lift Test and Canadian Occupational Performance Measure ratings.
Table 3 describes the outcomes of the COPM pre- and post-intervention scores including work self-efficacy performance and satisfaction outcomes. The combined performance and satisfaction scores indicate the changes in work self-efficacy ratings across each of the two domains.
Discussion
Evaluating Feasibility
This pilot study demonstrates the feasibility of implementing tailored, functional work-related activities into an existing physical exercise program. At the participant level, results suggest participants were interested and able to complete both their routine ACE program and additional work-related functional activities. Adherence, as reflected in 100% participation and completion, has been difficult to obtain in other previously published cancer-specific return-to-work interventions [1, 27]. In our study, by facilitating an embedded and functional work-focused program into the already existing and scheduled ACE program, participants could maximize their time in each session, with minimal additional time burden.
At the level of the occupational therapist, there were no issues with managing the development of the tailored interventions from the issues reported by each of the participants. Previously published literature has reported challenges in implementing and completing cancer- specific return-to-work interventions given the lack of rehabilitative personnel with expertise in cancer management and function [27, 28]. In our study, the involvement of occupational therapy ensured that functional goals were being addressed and progressed.
At the level of the institution, there were challenges and successes that arose from using a fitness centre and clinic space to conduct a functional, work-related intervention. While the challenges of limited equipment have been explained, the success of having a cohesive functional and physical program carried out in one location has benefits of efficiency and familiarity [29]. At the level of the assessments, use of lift tests and the COPM offer potential for outcome measures used in cancer survivor return-to-work research.
Testing Effectiveness: Lift Tests
While this study was proposed to test feasibility, results of the lift tests showed promising improvements across all participants who completed the pre- and post- intervention lift tests. The results reflect the conditioning and strengthening gains from the general physical exercise program, pointing to the potential benefits for combined interventions for work-related rehabilitation. While the results of the lift tests are promising, there is not a direct comparison that can be made to other studies of this nature. What is known is that cancer survivors with physically demanding vocations involving heavy lifting are at greater risk of failing attempts to return to work after their cancer treatment [30]. Moreover, those with heavy-lifting vocations are less likely to reintegrate into the workforce, despite the attention given on strength and conditioning in work-hardening programs [30, 3]. Our findings warrant further investigation of such interventions and outcomes in well-designed clinical trials.
Work Self-Efficacy Performance and Satisfaction: The COPM
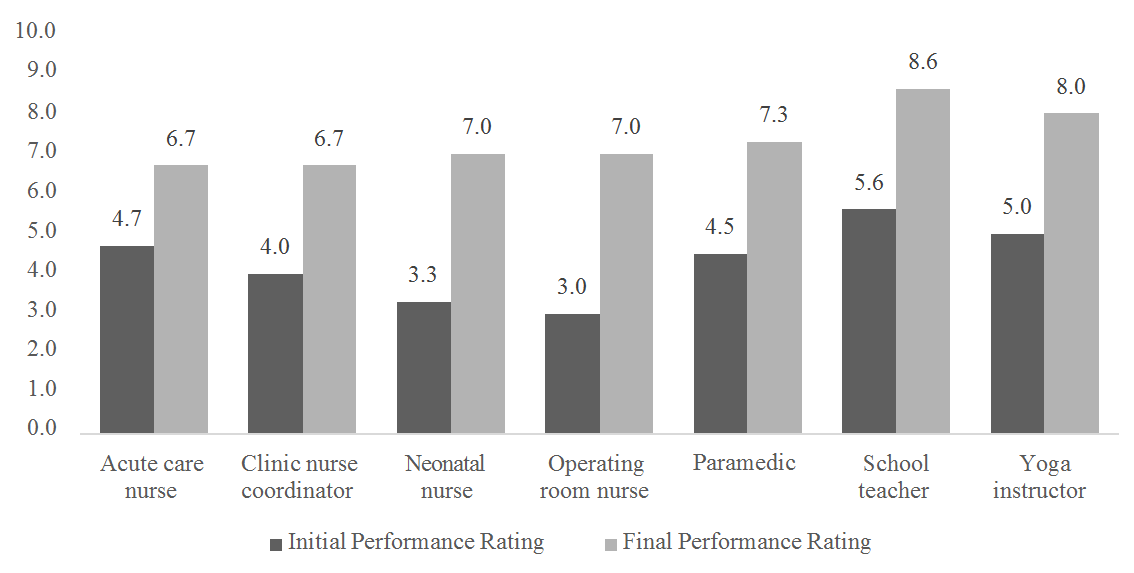
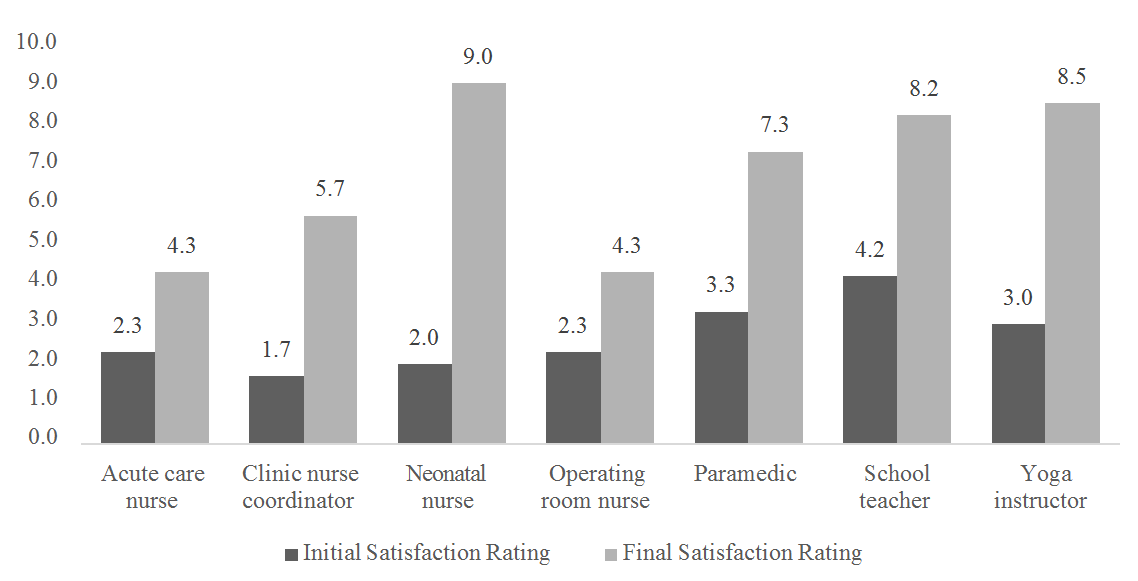
The COPM is not typically used in return-to-work research in cancer care [31]. However, at present, no cancer-specific functional outcome measure related to self-efficacy in return-to-work exists [32]; this current lack of measure could be the result of limited occupational therapy-driven research in this area. While the graphed depiction of COPM outcomes (see Figures 2 and 3) is not commonplace, it serves well for visually reflecting the results of this PoC study. Meaningful improvements were seen across the measured domains of performance and satisfaction in the category of productivity, from each individual participant and across the overall group. Interestingly, in most studies exploring the COPM, all categories of self-care, leisure, and productivity are examined, wherein self-care then often becomes the category of focus [33]. Emphasis on self-care leads to the possibility of a reduced focus on productive, or work- related, outcomes [33]. Further, in studies looking at the COPM as a work-related measure in breast cancer survivors, it was found that the COPM, completed in its entirety, did not effectively capture work-related goals [34]. In this pilot study, only the productivity category was used, allowing for work-related issues to be the sole focus of the importance, performance, and satisfactions ratings of the COPM.
Since the COPM is an individualized evaluation, we could explore the COPM results of each participant, from baseline to post intervention on work self-efficacy performance and satisfaction ratings. Additionally, since the COPM is a standardized assessment, we could then compare the change scores amongst the group. Each of the participants showed meaningful improvements in their own perceived performance and satisfaction ratings. In addition, the overall group findings reflected meaningful gains on both performance and satisfaction scales. The results of the self-reported participant measures reflect a positive association between the participation in the functional work-related activities and improved participant work self-efficacy outcomes in terms of performance and satisfaction. These findings are consistent with work-related self-efficacy literature, which suggests that self-perception and self-belief are key components of positive task outcomes [35]. Our findings suggest that the COPM shows promise as a measure of work self-efficacy performance and satisfaction for participants in a functional work-related intervention; further investigation of this outcome measure in a well- designed clinical trial would be beneficial.
Limitations and Strengths
PoC and pilot studies typically use a small number of respondents (n<20) to determine whether the study’s findings warrant further research. Given that each participant was compared to him/herself over time, a small sample size is not considered a limitation [36]. While this study included randomly selected participants from several professions, it happened that 3/7 participants were frontline nursing professionals (NOC code 3152). Moreover, given the inclusion criteria related to reporting RTW issues and having cancer- related fatigue or tiredness reported at moderate or higher level, the overall sample to draw from was quite small (n=22 who met eligibility criteria for inclusion from the n=65 ACE participants). Further, this study explored workability from a particular perspective, namely changes in work self-efficacy participation and satisfaction. As such, the details of specific vocations and roles were obtained primarily from participants’ self- report, and therefore may not be generalizable to those reporting similar concerns even within the same vocation.
Because the study coexisted in the same space as the parent study, equipment and baseline assessments were predetermined. Specifically, the gym equipment, including weights and machines, available in the exercise areas used were limited to fitness equipment and lighter weights. The lack of functional, work-specific equipment required creativity and problem solving to create certain functional activities. For example, in the case of the paramedic, heavier weights (sandbag weights were at a maximum of 40lbs), stair-climber equipment, and practice with an actual ambulance, would have allowed for a more tailored simulation. While a vocational rehabilitation space would have provided more opportunity to carry out work-related functional activities, the focus of this study was on the feasibility of embedding work-related functional activities into an exercise program, not work simulation. Given the fatigue issues of the participants, embedding work-related functional activities into an exercise program was used as a means to progress activities and improve overall physical endurance in preparation for future work rehabilitation.
Future Directions
The ongoing integration of tailored work-related functional activities into a cancer-specific exercise program will require further collaboration amongst occupational therapists, physiotherapists, exercise physiologists, and kinesiologists. The findings of this pilot study present a first step in delivering functional work- related activities and appropriate outcomes, which are currently lacking in the cancer rehabilitation setting. This pilot study can be used to inform future research in the field of CRF and work-specific outcomes. Clinically, integrating tailored work-related activities into existing exercise programming may provide a means of offering rehabilitation that has the potential for implementation and scalability.
Conclusion
This study offers two novel considerations for future research and practice: (1) feasibility of implementing tailored, functional work-related activities into existing cancer-specific exercise programming; and (2) the potential benefits of considering individualized assessments, such as the COPM in measuring work self- efficacy performance and satisfaction in functional, work- related interventions. Exploration of the individualized work-related needs and outcomes at the level of the cancer survivor allowed us to focus intensively on each survivor, and tailor the intervention to his/her specific work-related issues. This approach has potential to improve awareness and understanding of the subjective experience of cancer survivors in rehabilitative return-to- work contexts. Future research in functional work-related activities and measures of work self-efficacy is necessary, including well-designed clinical trials testing effectiveness.
The Authors Confirm that there is no Conflict of Interest
This research was funded through a Thesis Operating Grant from the University of Alberta Faculty of Graduate Research and Studies. The Alberta Cancer Exercise study is funded by Alberta Innovates and the Alberta Cancer Foundation.
References
-
de Boer AG, Taskila T, Tamminga SJ, Frings-Dresen MH, Feuerstein M, et al. (2015) Interventions to enhance return-to-work for cancer patients. Cochrane database of systematic reviews 9(2): CD007569.
-
van Egmond MP, Duijts SFA, Loyen A, Vermeulen SJ, van der Beek AJ, et al. (2017) Barriers and facilitators for return to work in cancer survivors with job loss experience: a focus group study. European journal of cancer care 26(5): e12420.
-
Mehnert A (2011) Employment and work-related issues in cancer survivors. Critical reviews in oncology/hematology 77(2): 109-130.
-
Parkinson M, Schultz IZ (2018) Cancer and work: a Canadian perspective. Toronto, ON: Canadian Association of Psychosocial Oncology 29(4): 258-266.
-
McNeely ML, Dolgoy N, Onazi M, Suderman K (2016) The Interdisciplinary Rehabilitation Care Team and the Role of Physical Therapy in Survivor Exercise. Clinical journal of oncology nursing 20(S6): S8-S16.
-
Monique C J Leensen, Iris F Groeneveld, Iris van der Heide, Tomas Rejda, Peter L J van Veldhoven, et al. (2017) Return to work of cancer patients after a multidisciplinary intervention including occupational counselling and physical exercise in cancer patients: a prospective study in the Netherlands. BMJ open 7(6): e014746.
-
Adam K, Gibson E, Strong J, Lyle A (2011) Knowledge, skills and professional behaviours needed for occupational therapists and physiotherapists new to work-related practice. Work 38(4): 309-318.
-
Bower JE, Bak K, Berger A, Breitbart W, Escalante CP, et al. (2014) Screening, Assessment, and Management of Fatigue in Adult Survivors of Cancer: An American Society of Clinical Oncology Clinical Practice Guideline Adaptation. Journal of Clinical Oncology 32(17): 1840-1850.
-
Ute Bültmann, Ute Bültmann (2013) Individual-Level Psychosocial Factors and Work Disability Prevention. In Loisel, P. & Anema, J.R., Handbook of Work Disability, pp: 149-162.
-
Law M, Baptiste S, McColl M, Opzoomer A, Polatajko H, et al. (1990) The Canadian occupational performance measure: an outcome measure for occupational therapy. Canadian Journal of Occupational Therapy 57(2): 82-87.
-
Margaret L McNeely, Christopher Sellar, Tanya Williamson, Melissa Shea-Budgell, Anil Abraham Joy, et al. (2019) Community-based exercise for health promotion and secondary cancer prevention in Canada: protocol for a hybrid effectiveness- implementation study. BMJ open 9(9): e029975.
-
Kendig CE (2016) What is proof of concept research and how does it generate epistemic and ethical categories for future scientific practice?. Science and engineering ethics 22(3): 735-753.
-
Richardson LA, Jones GW (2009) A review of the reliability and validity of the Edmonton Symptom Assessment System. Current Oncology 16(1): 55.
-
Yellen SB, Cella DF, Webster K, Blendowski C, Kaplan E (1997) Measuring fatigue and other anemia-related symptoms with the Functional Assessment of Cancer Therapy (FACT) measurement system. Journal of pain and symptom management 13(2): 63-74.
-
Bultz BD, Groff SL, Fitch M, Blais MC, Howes J, et al. (2011). Implementing screening for distress, the 6th vital sign: a Canadian strategy for changing practice. Psycho-Oncology 20(5): 463-469.
-
Matheson LN, Isernhagen SJ, Hart DL (2002) Relationships among lifting ability, grip force, and return to work. Physical therapy 82(3): 249-256.
-
Gross DP, Battié MC (2002) Reliability of safe maximum lifting determinations of a functional capacity evaluation. Physical Therapy 82(4): 364-371.
-
Kuijer PP, Gouttebarge V, Brouwer S, Reneman MF, Frings-Dresen MH (2012) Are performance-based measures predictive of work participation in patients with musculoskeletal disorders? A systematic review. International archives of occupational and environmental health 85(2): 109-123.
-
De Baets S, Calders P, Schalley N, Vermeulen K, Vertriest S, et al. (2018) Updating the evidence on functional capacity evaluation methods: a systematic review. Journal of occupational rehabilitation 28(3): 418-428.
-
Government of Canada (2018) National Occupational Classification (NOC) system, Career Handbook, 3rd (Edn.), Ottawa, Canada.
-
Banks JJ, Caldwell GE (2019) Are psychophysically chosen lifting loads based on joint kinetics? Appl Ergon 74: 17-23.
-
Snook SH (1999) Future directions of psychophysical studies. Scand J Work Environ Health 25(S 4): 13-18
-
Gross DP, Haws C, Niemeläinen R (2012) What is the rate of functional improvement during occupational rehabilitation in workers’ compensation claimants? Journal of occupational rehabilitation 22(3): 292-300.
-
Dedding C, Cardol M, Eyssen IC, Dekker J, Beelen A (2004). Validity of the Canadian Occupational Performance Measure: a client-centred outcome measurement. Clinical rehabilitation 18(6): 660-667.
-
Mary Vining Radomski, Catherine A Trombly Latham (2002) Occupational therapy for physical dysfunction.
-
Mark V Johnston, Roger O Smith (2010) Single subject designs: current methodologies and future directions. OTJR: Occupation, Participation and Health 30(1): 4- 10.
-
Van Egmond MP, Duijts SFA, Scholten APJ, van der Beek AJ, Anema JR (2016) Offering a tailored return to work program to cancer survivors with job loss: a process evaluation. BMC public health 16(1): 940.
-
Tamminga SJ, Braspenning AM, Haste A, Sharp L, Frings-Dresen MH, et al. (2019) Barriers to and Facilitators of Implementing Programs for Return to Work (RTW) of Cancer Survivors in Four European Countries: A Qualitative Study. Journal of occupational rehabilitation 29(3): 550-559.
-
Gagliardi AR, Dobrow, MJ, Wright FC (2011) How can we improve cancer care? A review of interprofessional collaboration models and their use in clinical management. Surgical oncology 20(3): 146- 154.
-
Feuerstein M, Todd BL, Moskowitz MC, Bruns GL, Stoler MR, et al. (2010) Work in cancer survivors: a model for practice and research. Journal of Cancer Survivorship 4(4): 415-437.
-
Enemark Larsen A, Rasmussen B, Christensen JR (2018) Enhancing a client-centred practice with the Canadian Occupational Performance Measure. Occupational therapy international, pp: 11.
-
Silver JK, Gilchrist LS (2011) Cancer rehabilitation with a focus on evidence-based outpatient physical and occupational therapy interventions. American journal of physical medicine & rehabilitation 90(5): S5-S15.
-
Roberts AEK, James A, Drew J, Moreton S, Thompson R, et al. (2008) Measuring occupational performance and client priorities in the community: The COPM. International journal of Therapy and Rehabilitation 15(1): 22-29.
-
Désiron HA, Donceel P, de Rijk A, Van Hoof E (2013) A conceptual-practice model for occupational therapy to facilitate return to work in breast cancer patients. Journal of occupational rehabilitation 23(4): 516-526.
-
Wolvers MDJ, Leensen MCJ, Groeneveld IF, Frings- Dresen MHW, De Boer AGEM (2018) Predictors for earlier return to work of cancer patients. Journal of Cancer Survivorship 12(2): 169-177.
-
Lillie EO, Patay B, Diamant J, Issell B, Topol EJ, et al. (2011) The n-of-1 clinical trial: the ultimate strategy for individualizing medicine?. Personalized medicine 8(2): 161-173.
- Electrolyte Considerations for Athletes
- Comprehensive Rehabilitation in Adults with Diabetic Peripheral Neuropathy: A Literature Review on Frequency, Intensity, and Duration Parameters
- Exercise Duration and Its Association with ADHD Symptom Severity in Children and Adolescents: A Parent-Reported Survey Study
- Adaptation of the Adult Neurophysiology of Pain Questionnaire for Use in Pediatrics
- A Non-Pharmacological Multidisciplinary Pain Program within a Hospital Wellness Program: A Mixed Methods Study
- The Effect of Frenkel's Exercise with PNF on Functional Reach in Stroke Survivors: A Randomized Control Trial