Comparative Study between Low-Level Laser Therapy VS. Therapeutic Ultrasound along with Exercises in Patients with OA Knee
Study Design: Pre-post experimental study design. Background: Degenerative changes around knee joint involve ligaments and cartilages. It is heterogeneous group of conditions that leads to joint symptom and signs associated with integrity of articular cartilages. Objectives: Present study was undertaken to add on to available treatment methods for osteoarthritis knee and to find out the effectiveness of laser therapy and ultrasound therapy for treating osteoarthritis knee. Procedure: In this study, 30 participants were recruited based on inclusion and exclusion criteria. Laser therapy and ultrasound therapy was administered to them for a period of 2 weeks, 5 sessions per week. Pre and post assessment were taken using following outcome measures- Range of Motion (ROM), Numerical Pain Rating Scale (NPRS). Result: There was significant decrease in NPRS in patients which is suggestive of quality of life. Also, Knee ROM was found to be significantly increases amongst these participants. The outcome of NPRS and knee ROM was statistically analysed. It was found to be effective with significant P value<0.000. Conclusion: Ultrasound therapy is an effective treatment and can be used for treatment of patients with OA knee.
Introduction
Osteoarthritis (OA) is chronic degenerative musculoskeletal diseases, with higher prevalence in women. Knee is the common destruction of cartilage and bone changes a subchondral sclerosis and osteophyte. Due to inflammatory characteristics mainly of synovial membrane. Patient present pain and disability and consequently impaired quality of life. Physical modalities like Laser and Ultrasound therapies are usually prescribed in OA patients. The progress of osteoarthritis varies significantly from person to person.
Researcher Article
Some people have only mild changes that develop over a long period of time inside the joint. It is heterogeneous group of condition that leads to joint symptoms and signs which are associated with defective integrity of articular cartilage and changes in the underlying bone at the joint margin [1].
Symptoms
Knee pain: Pain is the most commonly reported symptoms of knee osteoarthritis. The description of pain will depend on the patient’s condition and situation.
Knee stiffness: Bone friction and swelling in the knee joint makes knee stiff and less flexible. Knee ROM can become more limited. Some people may only experience stiffness in the knee in the morning or after sitting for a long period. Knee swelling: When knee cartilage wears away, the femur and tibia bones can rub together, resulting in irritation and swelling of the knee. Knee popping: Feeling of crunching or bending a popping sound when bending the knee, are signs that cartilage has worn away and is not protecting the bones from friction [1].
Biomechanics
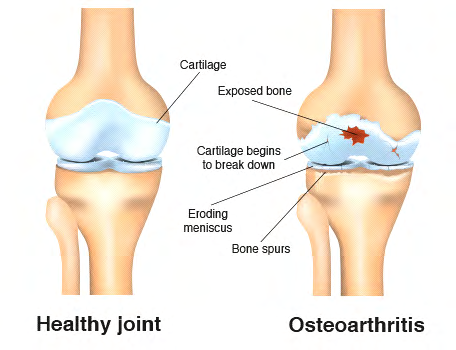
Osteoarthritis is morphological, biochemical, molecular and biomechanical changes of both cells and matrix, which leads to softening, fibrillation and loss of articular cartilage. The cartilage loses its elasticity and is more easily damaged by stress. At first, the degrades cartilage cells are replaced, but this repair process eventually begins to fail. The first major change in a joint affected with osteoarthritis is that the smooth cartilage surface softens and becomes pitted and frayed. As the cartilage continuous to breakdown, the joint loses its normal shape and mechanical structures (Figure 1). The bone ends thickens due to growth of cartilage and bone and forms “Spur” of bone called osteophytes at the point where the ligaments and joint capsule attach to the bone. Fluid filled sacs sometimes form in the bone near the joint and bits of bone or cartilage called “joint mice” may float loosely in the joint space, leading to the pain that occurs with movement [1].
Ultrasound Therapy: Ultrasound therapy utilises high- energy sound waves, which converts to heat and can be delivered to the deeper joint area. Along with improving joint movement, Ultrasound treatment also warms injured tissues, relieves muscle tension and increases blood circulation. Ultrasound is the effective in treatment of OA knee [2, 3]. Low-Level Laser therapy: Low-Level Laser therapy is therapeutic approach which uses low-intensity light emitting in range of 540-830mm light. Low-Level Laser therapy is used in many different diseases and mainly in pain control. They are named as low power lasers because they have a density of less than 5.0 W/cm2 [4, 5].
Method
In this study, subjects were recruited after Ethical clearance from the Institution. The study included 30 subjects between the age of 40-60yrs and was randomly assigned into two groups of 15 in each group. Group A was treated with Ultrasound therapy and Group B was treated with Low-level laser therapy with the isometric exercises like static quadriceps, static hamstrings were given for both the groups. All subjects was evaluated for pain using NPRS scale method used on Day 1 pre-treatment and day 10 post- treatment [6].
For Group A and Group B isometric exercises like static quadriceps, static hamstrings were given. The physiotherapy programme was conducted five times weekly for two weeks, for total 10 sessions for 15-20 minutes.
Inclusion Criteria
- Subjects with knee joint osteoarthritis as diagnosed by orthopaedican.
- Subjects above 40-60 yrs. age of both the genders.
- Subjects having anterior knee pain and to some extent generalised knee pain.
Exclusion Criteria
- Subjects with history of knee surgery.
- Subjects unable to walk without cane or crutch.
- Secondary osteoarthritis due to trauma.
- Cardiac patients.
Intervention Procedure
Before starting with the test participants were instructed not to undergo any other intervention for knee pain.
Intervention Included Following Techniques Ultrasound Therapy: During the therapy session ultrasound therapy was applied to the anterior aspect of the knee by the therapist stroking the applicator in circular movements. Continuous ultrasonic waves with 1 MHz frequency and 1 W/cm2 power was applied with a 4 cm diameter applicator Low Level Laser Therapy: Laser was used with wavelength of 830nm. The treatment was applied to the anterior aspect of the knee joint (Figures 2 & 3).

Result
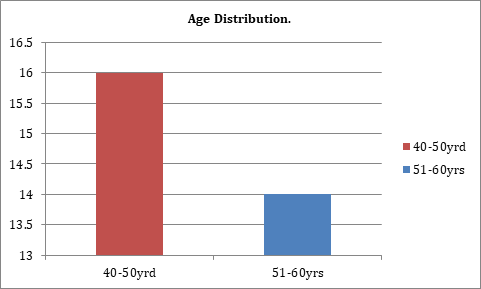
Table 1 and Graph 1 interpret the age difference between 40-60 yrs. of age is 16 and between 51-60 yrs. of age is 14. Table 2 and Graph 2 interprets the gender distribution between male which was 14 and female was 16. Table 3 and Graph 3 interpret the pre-treatment knee flexion within Group A (Ultrasound) was 102 and post- treatment knee flexion within Group A was 126.3 shows non-significant result. Table 4 and Graph 4 interprets the pre-treatment knee flexion within Group B (Laser) was 98 and post-treatment knee flexion within the Group B was 109.3 which shows no-significant result. Table 5 and Graph 5 interprets pre-treatment NPRS within the Group A was 6.6 and post-treatment NPRS within the Group A was 1.4 which shows non-significant result. Table 6 and Graph 6 interprets pre-treatment NPRS within the Group B was 6.6 and post-treatment NPRS within the Group B was 1.4which shows non-significant result. Table 7 and Graph 7 interpret the difference between pre and post knee flexion of Group A was 24.33 and Group B was9.33 which shows non-significant result. Table 8 and Graph 8 interpret the difference between pre and post NPRS for Group A was5.2 and for Group B was 4.533 which shows non-significant result.
| Age | 40-50yrd | 51-60yrs |
|---|---|---|
| Total no | 16 | 14 |
Table 1: Age and years.

Graph 1: Age distribution.
| Male | Female | |
|---|---|---|
| Total No. | 14 | 16 |
Table 2: Gender.
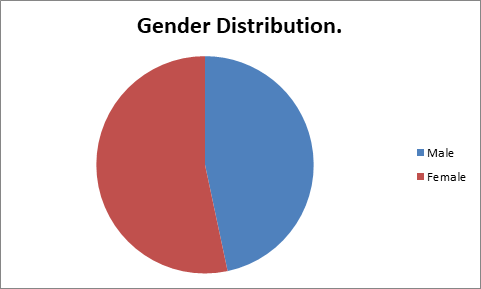
Graph 2: Age distribution.
| Group | Mean | SD | p value |
|---|---|---|---|
| Pre Treatment | 102 | 10.82 | 0 |
| Post Treatment | 126.3 | 10.93 | |
| Pre treatment | 6.6 | 0.6325 | 0 |
| Post Treatment | 1.4 | 0.6325 |
Table 3: Groups.
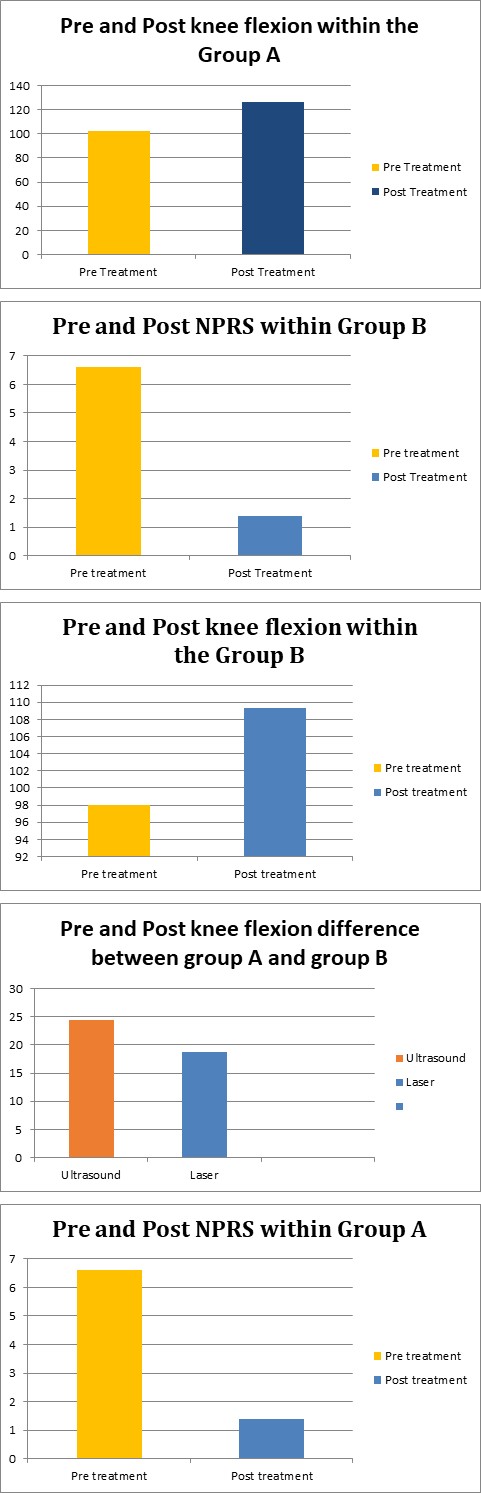
Graph 3: Pre and Post knee flexion within the Group A.
| Mean | SD | p value | |
|---|---|---|---|
| Pre treatment | 98 | 8.619 | 0 |
| Post treatment | 109.3 | 8.423 |
Table 4: Groups.
Graph 4: Pre and Post knee flexion within the Group B.
| Group | Mean | SD | p value |
|---|---|---|---|
| Pre treatment | 6.6 | 0.6325 | 0 |
| Post treatment | 1.4 | 0.6325 |
Table 6: Pre-treatment and Post treatment.
Graph 5: Pre and Post NPRS within Group A.
Graph 6: Pre and Post NPRS within Group B.
| Mean | SD | p value | |
|---|---|---|---|
| Ultrasound | 24.33 | 6.51 | 0.097 |
| Laser | 9.33 | 3.71 |
Table 5: Group of ultrasound and laser.
Graph 7: Pre and post knee flexion between Ultrasound and laser.
| Group | Mean | SD | p value |
|---|---|---|---|
| Ultrasound | 5.2 | 0.8619 | 0.101 |
| Laser | 4.533 | 1.06 |
Table 7: Group of ultrasound and laser.
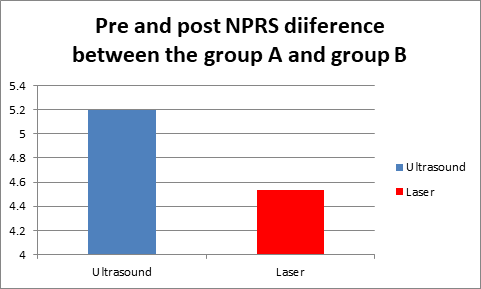
Graph 8: Pre and post NPRS difference between ultrasound and laser group.
Discussion
Osteoarthritis is chronic degenerative musculoskeletal disease affecting 20% of population. Knee is the common destruction of cartilage and bone changes as subchondral sclerosis and osteophyte. Patient present with pain and disability and consequently impaired quality of life. Physical modalities like Ultrasound therapy and Laser therapy are effective in treating OA patients. It is heterogeneous group of condition that leads to joint symptoms and signs which are associated with defective integrity of articular cartilage and changes in the underlying bone at joint margin.
The purpose of the study is to compare the effect between laser therapy and Ultrasound Therapy (UST) in treatment of OA knee in reducing pain and improve ROM.
In this study Group A i.e. patients treated with ultrasound therapy show better improvement than Group B i.e. patients were treated with laser therapy. Both the groups showed improvement in treating osteoarthritis knee joint, but group A showed better improvement than Group B.
UST was given in continuous mode for 10 sessions each with 1 MHz for 10 min, showed significant improvement in pain and ROM.UST was given around the anterior portion of the knee joint targeting the soft tissues.
Scanning LASER was given with power output of 25 Mw and wavelength of 830nm. UST have the effect of reducing pain and muscle spasm and promoting healing processes. Laser also helps in pain control and tissue healing.
Patients were assessed pre-treatment and post- treatment with NPRS in Group A as well as in Group B. Both the groups showed improvement in OA knee joint but Group A showed better result than Group B.
Yet UST when performed on patient, the rotation of transducer head created Micro-massage over the painful part, that gave a sense of well-being and psychologically feeling of betterment. Whereas in Laser, patients were sceptic about the modality as there was no feeling of getting treated during treatment session. So psychologically they might be anxious hence the improvement was not as per as patient treated with UST. Thus it can be the reason for ultrasound therapy to be more effective as compared to laser therapy in improving Range of motion and reducing pain in patients with OA knee joint.
Conclusion
Thus, the study concluded that both Ultrasound therapy and Low level laser therapy are effective in increasing ROM and decreasing pain in OA Knee. But Ultrasound therapy was found to be more effective than laser therapy in improving ROM and decreasing pain.
References
-
Fisher AGL (1992) A contribution to the pathology and etiology of osteoarthritis with observation upon the principles underlying its surgical treatment. Br J Surg 10(37): 52-80.
-
Falconer J, HayesKW, Chang RW (1992) Effect of Ultrasound on Mobility in Osteoarthritis of the Knee. pp: 29-35.
-
Marks R, Hannnnnnagarja SG, Ghassemi M (2000) Ultrasound for osteoarthritis of a knee a systemic review. Physiotherapy 86(9): 452-463.
-
Bjordal M Green (2003) significant pain relief after low laser treatment for knee osteoarthritis. Lasers Surg Med 5: 330-338.
-
Don Fitz-Ritson (2000) Laser and osteoarthritis. Dynamic chiropractic.
-
Ferraz MB, Quaresma MR (1990) Reliability of pain scales in the assessment of literate and illiterate patients with rheumatoid arthritis. J Rheumatol 17(8): 1022- 1024.
- Electrolyte Considerations for Athletes
- Comprehensive Rehabilitation in Adults with Diabetic Peripheral Neuropathy: A Literature Review on Frequency, Intensity, and Duration Parameters
- Exercise Duration and Its Association with ADHD Symptom Severity in Children and Adolescents: A Parent-Reported Survey Study
- Adaptation of the Adult Neurophysiology of Pain Questionnaire for Use in Pediatrics
- A Non-Pharmacological Multidisciplinary Pain Program within a Hospital Wellness Program: A Mixed Methods Study
- The Effect of Frenkel's Exercise with PNF on Functional Reach in Stroke Survivors: A Randomized Control Trial