A Comparative Study of Scapular Clock Excercises Vs Scapular PNF in the Treatment of Adhesive Capsulitis
The aim of the study was to compare the effect of scapular clock exercises and scapular PNF techniques on pain and range of motion in the patients with adhesive capsulitis. In this study total 30 samples of Adhesive Capsulitis were screened according to the inclusion and exclusion criteria and were divided in two groups of 15 samples in each group respectively. Group A was treated with Scapular clock exercises whereas group B was treated with Scapular PNF techniques. Pretreatment and post treatment outcome measures were taken. Assessment was carried with the outcome measures Numerical pain rating scale (NPRS) for pain and a Universal Goniometer for Range of Motion. Subjects from both the groups were received treatment for 8 sessions a single session per day. The amount of change in the outcome measures were evaluated by the paired t test for comparing within the groups and t test was used to compare the results in between both the groups. The analysis of the study states, both the treatment groups shows significant reduction in pain, increase in Range of motion but Group B i.e. Scapular PNF group showed more significant improvement than Group A statistically. Study concluded that both Scapular Clock exercises and Scapular PNF techniques are effective on the pain and range of motion in Adhesive Capsulitis But Scapular PNF technique proved to be more effective than Scapular Clock exercises.
Introduction
Adhesive Capsulitis is a deceptive difficult condition with steady limitation of the considerable number of planes of development in the shoulder joint. It is a favorable self-constraining state of obscure etiology described by excruciating and restricted dynamic and detached glenohumeral scope of movement. Adhesive capsulitis ordinarily alluded to as solidified shoulder is related with synovitis and capsular contracture of the shoulder joint [1].
Neviaser, et al. [2] distinguished four phases of adhesive capsulitis, they are corresponded with clinical assessment as well as histological highlights. The stage one is the excruciating stage, described with gradual onset of manifestations. Manifestations continues for around
3months and additionally comprise aching pain alluded at the deltoid insertion point and unable to rest at the influenced side.
Patients might have a mellow restriction of ROM that perpetually settle along the organization of nearby sedative. The arthroscopic see, affirmed with biopsies, reveals a hypertrophic, well vascularized typical synovitis without attachments or any capsular contracture. The subsequent stage i.e., stage two is additionally termed as the “freezing stage”. Manifestations proceeds from 3 to 9 months that are portrayed with nighttime torment additionally when patients happens to be lying on the influenced side, moreover a critical loss in both dynamic as well inactive ROM is alluded. The Arthroscopic see reveals a thickened ipervascular synovitis. The Histological findings appears to be as perivascular plus subsynovial scar development along with testimony of confused collagen fibrils with hyper cellular appearance, yet no provocative invades had found. The shoulder organize stage number 3, the “solidified stage”, side effects endures since 9 to 14 months. The shoulder solidness is overwhelming and torment may in any case be available toward the finish of movement or around evening time. Arthroscopic assessments exhibits inconsistent synovial layer thickening with loss of axillary break; biopsy indicate thick, hyper cellular collagenous tissue. The final stage is the “defrosting stage” which is described by negligible torment along with slow improvement in ROM because of the capsular remodeling. This organize happens somewhere in the range of 15 and two years. Arthroscopic and histological relationship has not been examined [3].
The scapular position and motions on the thorax is a critical component of the normal glenohumeral function and plays great roles in facilitating optimal shoulder movements. In normal upper-quarter function, the scapula provides a stable base from which glenohumeral mobility occurs. Stability of the scapula depends on the surrounding musculature. These muscles must dynamically position the glenoid so that efficient glenohumeral movement can occur. During all movements of the glenohumeral joint especially overhead elevation of the arm, it is of great importance that the scapular stabilizing musculature should be strong enough to properly position the scapula. The main scapula stabilizers are the Levator Scapulae, Rhomboids major and minor, Serratus anterior, and Trapezii. These muscle groups function through synergistic co contraction with rotator cuff to control the scapular movement [4]. When weakness or dysfunction is present in the scapular musculature, normal scapular positioning and mechanics may become altered which result in abnormal stresses to the capsular structures, rotator cuff compression and reduced performance [5].
Scapular stabilization exercises likewise help to keep up the length strain relationship of the scapular muscles in this manner giving stabilized scapula which adequately diminishes the time taken by the patient dealing with adhesive capsulitis of the glenohumeral joint [6].
PNF treatment has an idea of four hypothetical systems, alluded to as autogenic inhibition, reciprocal inhibition, stress relaxation, and the gate control hypothesis, that do upgrade ROM and muscular activation. Proprioceptive neuromuscular facilitation stretch is a technique commonly used in clinical environments to enhance both active and passive ROM with the ultimate goal being to optimize motor performance and rehabilitation. The literature regarding PNF has made the technique, the optimal stretching method when the aim is to increase ROM, especially in a short term changes [7]. PNF considered as viable in easing torment thus shows improvement in the functional capacities. PNF techniques, which includes reciprocal activation of the agonist muscles and antagonist muscles to the ideal movement leads to efficient muscle working. Among restorative methodologies, joint mobilization grades utilizing PNF techniques positively affects pain intensity, muscle power, and Range of Motion. Appropriate capacity involving furthest points require movement as well as soundness of the scapula. The scapular movement patterns characterized in the PNF techniques are activated in upper limb and scapular movements. The impacts of PNF techniques on the affected shoulder are usually researched in certain examinations [7].
The objectives of this study are to determine the effect of Scapular clock exercises on Shoulder Range of Motion and pain in Adhesive Capsulitis, to determine the effect of Scapular PNF on shoulder Range of Motion and pain in Adhesive Capsulitis, to compare scapular clock exercises and scapular PNF on shoulder Range of Motion and pain in Adhesive Capsulitis. The null hypothesis of the study is that there will be no difference in Range Of Motion and pain disability index between scapular clock and scapular PNF after 8sessions of treatment in patients with Adhesive Capsulitis. An Alternative hypothesis of the study are 1: There will be difference in Range Of Motion and pain disability index after 8 sessions in scapular clock exercise group in the patients with Adhesive Capsulitis. 2: There will be difference in ROM and pain disability index after 8 sessions in scapular PNF exercise group in the patients with Adhesive Capsulitis. So the aim of this study is to compare the effect of Scapular Clock Exercises Vs Scapular PNF in Adhesive Capsulitis.
Methods
In this Comparative study design, participants were recruited after approval from the Institutional Ethical Committee Clearance. Subjects were recruited for this study from in and around Dr. DY Patil Physiotherapy OPD and Dr. DY Patil Orthopaedic OPD, Pimpri, Pune. The objective of the study was clearly elaborated and written consent was taken from the subjects. The subjects fulfilling the inclusion and exclusion criteria were recruited using lottery method of simple random sampling technique and then were divided in group A( scapular clock exercises) and group B (scapular PNF). The subjects were explained the proposed benefits, risks and procedure involved in detail in the best possible language understood by them. The subjects then were assessed for the outcome measures using NPRS for pain and goniometry for shoulder ROM pre-intervention. After this procedure, treatment was administered to them for 8 sessions, 1 session per day and patient again were assessed post 8th session for the said outcomes.
Outcome Measure
- Range of Motion (Universal Goniometer)
- Numeric Pain Rating Scale (NPRS) Inclusion criteria was -Patients referred by Orthopaedican, Participants willing to participate, Stage 2 (frozen Stage) Adhesive capsulitis, Patients with unilateral involvement,Both the genders of age between 40-60 years. Exclusion criteria was- Previous shoulder manipulation under anesthesia, Osteoarthritis of shoulder or acromian clavicular joint, Metastasis or primary tumors if any Patients with Post traumatic shoulder or shoulder dislocation, Patients with cervical spondylosis, sprengel’s deformity or tuberculosis,Patients with Bilateral adhesive capsulitis, Intra articular cortico-steroid injection in affected shoulder in past 3 months, Recent upper limb fractures if any,Recent cardiac Surgery if any, done.
Intervention for group A included the following techniques:
- Hot moist pack (5-10min)
- Scapular clock exercises (2 sets of 10 reps followed by 3 sets of 10 reps)
- Posterior capsular stretches(corner stretch, crossed arm stretch, sleeper stretch)
- Maitland’s grade III and Grade IV mobilization(inferior glide, posterior glide, anterior glide)
- Cryotherapy (5-10min). Intervention for group B included the following techniques:
- Hot moist pack (5-10min)
- Scapular PNF exercises (2 sets of 10 reps followed by 3 sets of 10 reps)
- Posterior capsular stretches(corner stretch, crossed arm stretch, sleeper stretch)
- Maitland’s grade III and Grade IV mobilization(inferior glide, posterior glide, anterior glide)
- Cryotherapy (5-10min).
Scapular Clock Exercises: Patient is in kneeling position with the affected arm placed on Swiss ball with elbow fully extended, places the finger pointed towards the 3’o clock- scapula is protracted, 6’o clock- the scapula is depressed & 9’o clock- the scapula is retracted, 12’ o clock- shoulder is elevated [1]. Scapular PNF techniques: Patient was asked to lie on the uninvolved side and the therapist will stand along the line of desired movement. Initially, the examining therapist pulls the involved scapula in the elongated position while instructions will be given to perform required movement. Application of Rhythmic Initiation and Repeated Contractions techniques in all the patterns are ideally matched scapular facilitation techniques considering PNF agonistic techniques. The Rhythmic Initiation Techniques educates the motion, aids relaxation, improve co-ordination also normalize the motion of the scapula (Figures 1a-1d). The Repeated Contraction technique improves ROM, strength and movement towards required movement (Figures 2a-2d). The resting period in between repetitions will be 20seconds [7].

Figure 1a: 12’o clock position.
Figure 1b: 9’o clock position.
Figure 1c: 6’o clock position.
Figure 1d: 3’o clock position.
Figures 2a&b: Anterior elevation with posterior depression.
Figures 2c&d: Posterior elevation and anterior depression.
Results
A total of 30 samples with Adhesive Capsulitis were recruited for treatment intervention. A total of 30 samples were randomized into two groups and all evaluated before the treatment and after 8 sessions of the treatment.
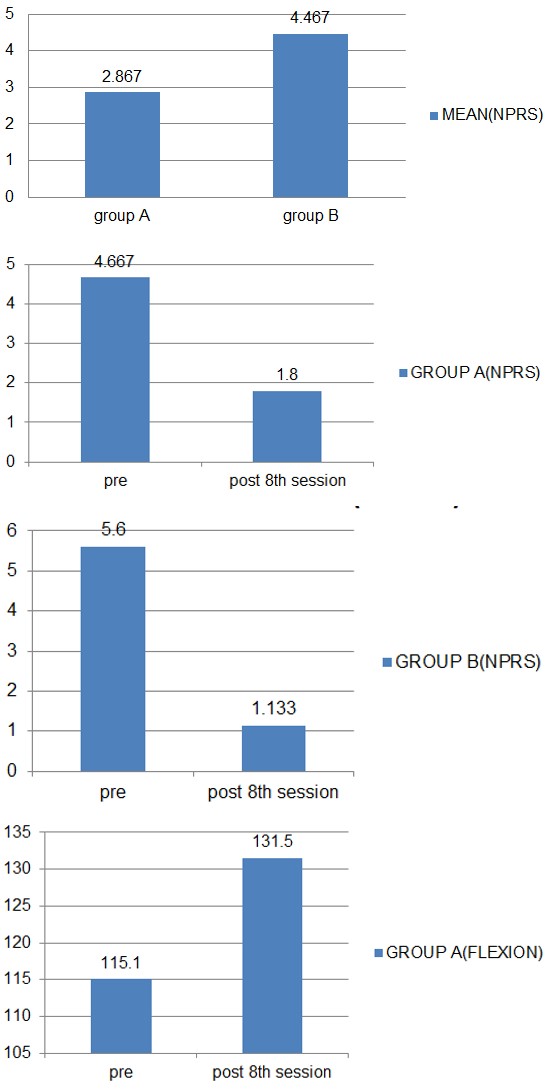
Table 1 & Graph 1 show that out of 30 subjects, 13 subjects were male while 17 subjects were female.
| Gender | Gender Distribution |
|---|---|
| Male | 13 |
| Female | 17 |
Table 3: Subjects.
Graph 1: Gender distribution in the study.
Table 2 & Graph 2 shows that out of 15 subjects from Group A, six consisted of males & 9 were females, whereas out of 15 subjects from Group B, seven were males, while 8 were females.
| Group A | Group B | |
|---|---|---|
| (n=15) | (n=15) | |
| Male | 6 | 7 |
| Female | 9 | 8 |
Table 1: Genders.
Graph 2: Gender distribution in both the groups.
Table 3 & Graph 3 shows that in 40-45 age group category there were 13 subjects, in 46-50 age group category there were 4 subjects, whereas in 51-55 age group category there were 8 subjects & in 56-60 age group category there were 5 subjects respectively.
| Age | Total subjects | |
|---|---|---|
| Gender | Gender Distribution | |
| Male | 13 | |
| Female | 17 |
Table 2: Subjects.
Graph 3: Age distribution.
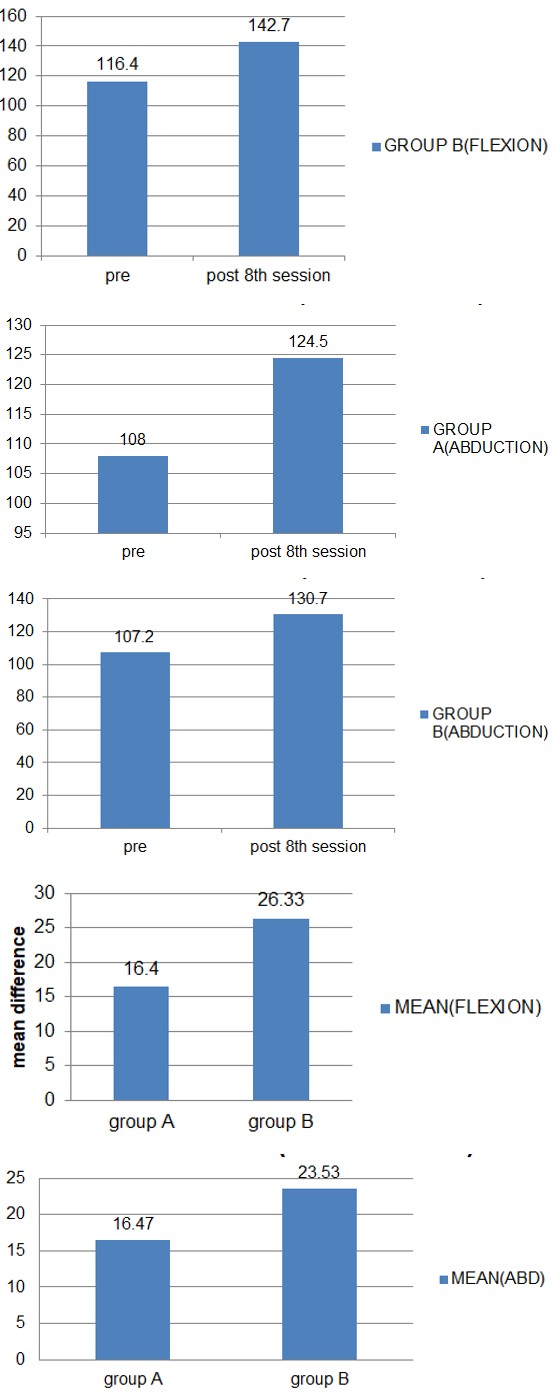
Table 4a-b & Graph 4a-b, NPRS scores for Group A decreased from 4.66 to 1.8 whereas in Group B, NPRS scores decreased from 5.6 to 1.33. There was significant improvement in NPRS scores in both the groups with p<0.05 respectively in both groups.
| NPRS | Group A | |
|---|---|---|
| Pre | Post | |
| Mean | 4.66 | 1.8 |
| S.D | 2.498 | 1.424 |
| P value | P=0.000 |
| NPRS | Group B | |
|---|---|---|
| Pre | Post | |
| Mean | 5.6 | 1.133 |
| S.D | 1.639 | 0.9904 |
| P value | P=0.000 |
| NPRS | Group A | Group B |
|---|---|---|
| Mean Difference | 2.867 | 4.467 |
| S.D | 1.552 | 1.457 |
| P value | P=0.007 |
Tables 4a-c: Numerical Pain Rating Scale.
Graph 4a: Group A Mean (NPRS).
Graph 4b: Group b means (NPRS).
Table 4c & Graph 4c, mean diff. of NPRS scores in Group A was found to be 2.867 while Group B was 4.467 with p>0.05, suggesting that both techniques were equally effective in reducing pain.
Graph 4c: Between the groups mean difference (NPRS).
Table 5a-b & Graph 5a-b, Shoulder Flexion ranges for Group A increased from 115.1 to 131.5 whereas in Group B, Shoulder Flexion ranges increased from 116.4 to 142.7. The graphical presentation showed improvement in Shoulder Flexion ranges in both the groups with p<0.05 respectively which is statistically significant.
| Shoulder Flexion | Group A | |
|---|---|---|
| Pre | Post | |
| Mean | 115.1 | 131.5 |
| S.D | 18.04 19.7 | |
| P value | P=0.000 |
| Shoulder Flexion | Group B | |
|---|---|---|
| Pre | Post | |
| Mean | 116.4 | 142.7 |
| S.D | 9.941 | 13.43 |
| P value | P=0.000 |
| Shoulder Flexion | Group A | Group B |
|---|---|---|
| Mean Difference | 16.4 | 26.33 |
| S.D | 5.816 | 6.997 |
| P value | P=0.000 |
Tables 5a-c: Shoulder Flexion.
Graph 5a: Group a mean (flexion).
Graph 5b: Group b mean (flexion).
Table 5c & Graph 5c, mean diff. of Shoulder Flexion ranges in Group A was found to be 16.4 while Group B was 26.33 with p>0.05, suggesting that both techniques were effective in improving Shoulder Flexion ranges but Group B showed better results as compare to Group A.
Graph 5c: Between the groups mean difference (flexion).
Table 6a-b & Graph 6a-b, Shoulder Abduction ranges for Group A increased from 108 to 124.5 whereas in Group B, Shoulder Abduction ranges increased from 107.2 to 130.7. There was significant improvement seen in Shoulder Abduction ranges in both the groups with p<0.05 respectively in both groups.
| S.Abuction | Group A | |
|---|---|---|
| Pre | Post | |
| Mean | 108 | 124.5 |
| S.D | 11.51 12.35 | |
| P value | P=0.000 |
| S. Abuction | Group B | |
|---|---|---|
| Pre | Post | |
| Mean | 107.2 | 130.7 |
| S.D | 8.029 | 6.63 |
| P value | P=0.000 | |
| S.Ex.Rotation | Group A | |
| Pre | Post | |
| Mean | 36.73 | 44.13 |
| S.D | 6.307 13.91 | |
| P value | P=0.037 |
| S. Abduction | Group A | Group B |
|---|---|---|
| Mean Difference | 16.47 | 23.53 |
| S.D | 8.871 | 6.556 |
| P value | P=0.019 |
Tables 6a-c: Shoulder Abduction.
Graph 6a: Group a mean (abduction).
Graph 6b: Group b mean (abduction).
Table 6c & Graph 6c, in Table 6b & Graph 6b, mean diff. of Shoulder Abduction ranges in Group A was found to be 16.47 while Group B was 23.53 with p<0.05, suggesting that Group B technique was more effective in improving Shoulder Abduction ranges as compared to Group A technique.
Graph 6c: Between the group mean difference (abduction).
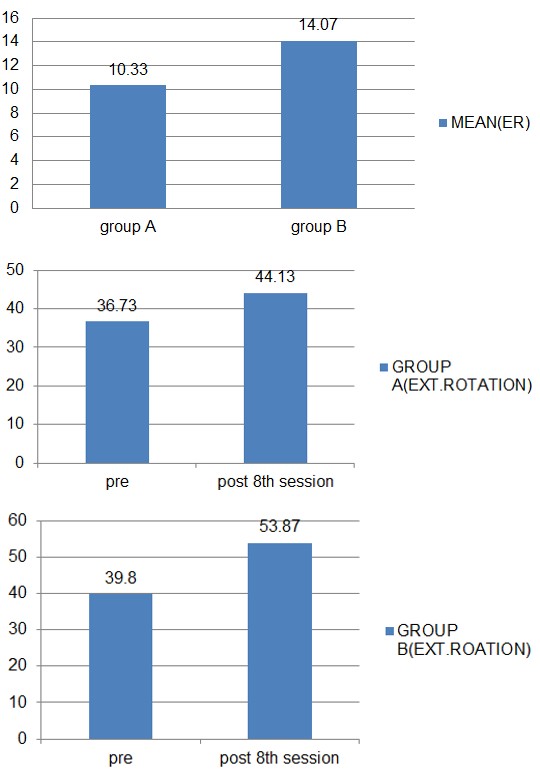
Table 7a-b & Graph 7a-b, Shoulder Ext. Rotation ranges for Group A increased from 36.73 to 44.13 whereas in Group B, Shoulder Ext. Rotation ranges increased from 39.8 to 53.87. There was significant improvement seen in Shoulder Ext. Rotation ranges in both the groups with p<0.05 respectively in both groups.
| S.Ex.Rotation | Group B | |
|---|---|---|
| Pre | Post | |
| Mean | 39.8 | 53.87 |
| S.D | 6.038 | 6.128 |
| P value | P=0.000 |
| S. Abduction | Group A | Group B |
|---|---|---|
| Mean Difference | 10.33 | 14.07 |
| S.D | 4.152 | 1.668 |
| P value | P=0.003 |
Tables 7a-c: Shoulder External rotation.
Graph 7a: Group a mean (ext. rotation).
Graph 7b: Group B Mean (Ext. Roation).
Table 7c & Graph 7c, mean diff. of Shoulder Ext.Rotation ranges in Group A was found 10.33 while Group B was 14.07 with p<0.05, suggesting that Group B technique was more effective in improving Shoulder Ext. Rotation ranges as compared to Group A technique.
Graph 7c: Between the group mean difference (ext. rotation).
Discussion
Painful shoulder joint and dynamic confinement of both active and passive movement in the influenced shoulder is the characteristic feature of Adhesive Capsulitis. Keeping this thought, the point of our investigation is to analyze the scapular clock exercises and scapular PNF methods in managing adhesive capsulitis [8]. Different clinical practioners recommend increasingly concentrated managed physiotherapy regimen but simple home exercise protocol are proven powerful . A prospective report of two year follow-up analyzed intensive regimen of physiotherapy including stretching done passively and mobilization given manually with steady treatment and activities inside pain limits as reported. The investigation revealed activities within pain limits were found more viable as compare to intensive physiotherapy program [9].
Hot moist warmth, anti-inflammation causing medication, and a doctor coordinated recovery regimen were appeared to reliably bring about goals of symptoms [10]. A review study done by Shaffer et al. demonstrated that following a normal of a half year of physiotherapy (Codman’s activities, Ultrasound, TENS, uninvolved joint activation, and fortifying activities), statistically proven enhancements in active Range Of Motion were accomplished (99% flexion, 101% abduction, 62% lateral rotation) [11]. Then again, Rizke, et al. [12] noticed upto 60% of the patients treated with physiotherapy accomplished the capacity of resting free of pain following 5 months & Hazleman, et al. [13] announced 33% of the patients detailed expanded pain right after seeking physiotherapy treatment while 50% revealed notable results after treatment with rehabilitation exercises.
The shortcoming of the muscles around the scapula prompts scapular instability. At the point when the scapula isn’t steady it might cause adhesive capsulitis. The scapular stabilization practices were given to fortify the muscles, for example, (pectoralis major, lattisimus dorsi and teres major, trapezius, rhomboidus major and minor muscles) [1]. In past investigations scapular modifications were evaluated in patients with adhesive capsulitis however physiotherapy protocol was for the most part centered around help with discomfort and enhancement in ROM.
Peter J, et al. [14] inferred that glenohumeral ROM deficiencies comparative with the trunk and the involved scapula are available in subjects with frozen shoulder. Fayad F, et al. [15] did a study on three dimentional kinematics of scapula concluded that scapulohumeral rhythm of the involved shoulder is conversely identified with seriousness of the shoulder range of movement, expanded rotation of the scapula is confined to frozen shoulder as its compensatory design. The after effect of glenohumeral movement consists of the underlying 30 degrees of arm abduction while from 30 degrees of arm abuction to full arm abduction, the movement happens to be at involved glenohumeral & scapulothoracic joints. The sternoclavicular and acromioclavicular joints results into the movement of scapula. The proportion of Glenohumeral to Scapulothoracic movement is accounted for as 2:1. Significant muscular activity during early elevation of scapula are brought by upper and lower projections of the Serratus anterior muscle, the Levator scapulae muscle, the Rhomboid major and minor muscles, and the lower fibres of the Trapezius muscle. Taking into consideration the powers & movements created around the base of the spine of the scapula during the beginning periods of abduction activity of the arm, a predictable mechanical example is noted. The significant impact of the uppercase fibres of the Serratus anterior muscle also the abduction force applied at the scapula by the rotator cuff muscles are adjusted by the Rhomboid, Levator scapulae, and lower fibres of the Trapezius muscles. The impact of this activity balances out the root of the spine of the scapula, which acts as the focal point for rotation movement of around 90- 100 degrees of abduction activity. When the rotation of the scapula is advanced past this point, the chief wellspring of movement is the lowercase portion of the Serratus anterior muscle. The uppercase of the trapeziums activity basically restricts drawing of the deltoid activity, and has a constrained impact on scapular rotation motion. The fundamental factor is Serratus anterior muscle which balances out the scapula in its early period of progressing towards abduction also notwithstanding upwardly rotation the Scapula. In the cases of frozen shoulder, pre examination reveals limitation in the glenohumeral ROM because of capsule snuging, this forestalls out lateral rotation of the head of humerus, and the head of humerus shows sliding beneath the acromion process during elevation of the humerus. Right now humeral elevation, the scapula scopes as far as possible of the range sooner than humerus [16].
The impact neurophysiologically is instigated through Joint Mobilization depending on the incitement of Peripheral Mechanoreceptors also the hindrance of Nociceptors. Moreover, Mobilization strategies should increment or keep up the mobility of the joints by the prompt rheological changes observed in the synovial liquid, upgraded trade of the synovial liquid & the cartilage matrix, and the expansion of the synovial liquid turnover, is likely the only explanation for the pain level and ROM to be improved essentially [17].
Proprioceptive Neuromuscular Facilitation (PNF) systems help in improving range of movement as it lengthens the Golgi ligament organ that encourages unwinding of the antagonists. An examination directed by Gonzalez Rave et al., expressed that after the utilization of PNF procedures there is an improvement in patients shoulder and hip joint range of movement. It has been seen that when contrasted with different group the group which got PNF strategy was found to have expanded useful exercises and range of movement alongside the decrease in pain [18].
Given the results, both the techniques were found to have similar effects in terms of pain and disability Both the groups received conventional exercises such as hot moist pack, maitland grade III-IV mobilization, codman’s exercises, posterior capsular stretches & cryotherapy at the end of each treatment session. These exercises might have shown the added effects in both groups by activation of muscle stretch receptors, release of endomorphins and opiate substances, enhanced blood supply to the influenced areas resulting in changes in the viscoelastic properties of collagenous tissues of the shoulder region thereby improving ROM and reducing pain and disability.
Conclusion
From the above study it is concluded that both the techniques showed reduction in pain and improvement in Range Of Motion at the shoulder joint in stage 2 of Adhesive Capsulitis. However, the Scapular PNF techniques was found to be superior in terms of reducing pain intensity and improving shoulder ranges especially shoulder flexion, abduction and external rotation in patients with Adhesive Capsuitis.
References
-
Kirthika SV, Bhavani PB, Rajlakshmi V (2015) Effect of combining scapular stabilization techniques with conventional physiotherapy in improving range of motion and functional ability in subjects with phase II adhesive capsulitis of the shoulder joint. Journal of Physiotherapy & Occupational Therapy 1(1): 25-34.
-
Hannafin JA, Dicarlo EF, Wickiewicz TL (1994) Adhesive capsulitis: capsular fibroplasia of the glenohumeral joint. J Shoulder Elbow Surg 3: 435-440.
-
Mengiardi B, Pfirrmann CW, Gerber C, Hodler J, Zanetti M (2004) Frozen shoulder: MR arthrographic findings. Radiology 233: 486-492.
-
Yano Y, Hamada J, Tamai K, Yoshizaki K, Sahara R, et al. (2010) Different scapularkinematics in healthy subjects during arm elevationand lowering: glenohumeral and scapulothoracicpatterns. Journal of shoulder and elbow surgery 19(2): 209-215.
-
Voight ML, Thomson BC (2000) The role of the scapula in the rehabilitation of shoulder injuries. Journal of Athletic training 35(3): 364.
-
Jobe FW (1993) Adhesive Capsulitis: A Case Report.
-
Balci NC, Yuruk ZO, Zeybek A, Gulsen M, Tekindal MA (2016) Acute effect of scapular proprioceptive neuromuscular facilitation (PNF) techniques and classic exercises in adhesive capsulitis: a randomized controlled trial. The journal of Physical Therapy Science 28(4): 1219-1227.
-
Vermeulen HM, Obermann WR, Burger BJ (2000) End- range mobilization techniques in adhesive capsulitis of the shoulder joint: a multiple-subject case report. Phys Ther 80: 1204-1213.
-
Jain TK, Sharma NK (2014) The effectiveness of physiotherapeutic interventions in treatment of frozen shoulder/adhesive capsulitis: a systematic review. J Back Musculoskeletal Rehabil 27(3): 247-273.
-
Miller MD, Wirth MA, Rockwood CA (1996) Thawing the frozen shoulder: the “patient” patient. Orthopedics 19: 849-853.
-
Shaffer B, Tibone JE, Kerlan RK (1992) Frozen shoulder. A long-term follow-up. J Bone Joint Surg Am 74(5): 738- 746.
-
Rizk TE, Pinals RS, Talaiver AS (1991) Corticosteroid injections in adhesive capsulitis: investigation of their value and site. Arch Phys Med Rehabil 72(1): 20-22.
-
Hazleman BL (1972) The painful stiff shoulder. Rheumatol Phys Med 11: 413-421.
-
Peter JR, Anderson DD, Carlos AG, Paula ML (2003) Shoulder Kinematics in Subjects with Frozen Shoulder. Arch Phys Med Rehabil 84: 1473-1479.
-
Fayad F, Roby BA, Yazbeck C, Hanneton S, Lefevre Colau MM (2008) Three-dimensional scapular kinematics and scapulohumeral rhythm in patients with glenohumeral osteoarthritis or frozen shoulder. Journal of Biomechanics 41: 326-332.
-
Vermeulen HM, Stokdijk M, Eilers PHC, Meskers CGM, Rozing PM (2002) Measurement of three dimensional shoulder movement patterns with an electromagnetic tracking device in patients with a frozen shoulder. Ann Rheum Dis 61: 115-120.
-
Vermeulen HM, Rozing PM, Obermann WR, Cessie SL, Vlieland TPV (2006) Comparison of High-Grade and Low-Grade Mobilization Techniques in the Management of Adhesive Capsulitis of the Shoulder, Randomized Controlled Trial. Physical therapy journal 86: 355-368.
-
Prasanna KJ, Rajeswari R, Sivakumar VPR (2017) Effectiveness of Scapular Proprioceptive Neuromuscular Facilitation (PNF) Techniques in Adhesive Capsulitis of the Shoulder Joint. Journal of Physiotherapy Research 1(2).
- Electrolyte Considerations for Athletes
- Comprehensive Rehabilitation in Adults with Diabetic Peripheral Neuropathy: A Literature Review on Frequency, Intensity, and Duration Parameters
- Exercise Duration and Its Association with ADHD Symptom Severity in Children and Adolescents: A Parent-Reported Survey Study
- Adaptation of the Adult Neurophysiology of Pain Questionnaire for Use in Pediatrics
- A Non-Pharmacological Multidisciplinary Pain Program within a Hospital Wellness Program: A Mixed Methods Study
- The Effect of Frenkel's Exercise with PNF on Functional Reach in Stroke Survivors: A Randomized Control Trial