Comparing the Effects of Mirror Theraphy and Neuromuscular Electrical Nerve Stimulation (NMES) in Enhancing the Hand Functional Recovery in Patients after Stroke: A Randomized Controlled Study
Objective: The purpose of this study was to assess the effectiveness of mirror theraphy and NMES in enhacing the upper extremity and hand motor and functional recovery , spasticity, and hand-related functioning and quality of life of patients after stroke. Design: Randomized, controlled, assessor-blinded, 4-week trial, with follow-up at 6 months. Setting: Rehabilitation education and research hospital. Participants: A total of 60 inpatients with stroke (mean age 61.45) were randomızed into three groups. Mirror (n:20), NMES (n:20) and Control(n:20) groups. Interventions: All patients received a conventional neuro rehabilitation treatment for 5 days a week, 2-4 hours a day for 4 weeks. In mirror group thirty minutes of mirror therapy program a day consisting of wrist and finger flexion and extension movements and NMES applied in front of a mirror, in NMES group; the mirror was covered than NMES applied and in control group neither NMES nor mirror was applied. Main Outcome Measures: Brunnstrom motor staging for upper extremity and hand, Modified Ashworth Scale (MAS), Functional Independence Measurement (FIM) self-care items of the FIM instrument), Nottingham Health Profile (NHP), Nine hole peg test (NHPT), superficial sense, deep sense (two point discrimination, steregnosia, graphestesia, joint position sense). Results: After the treatment, Brunnstrom motor stage improved in both mirror and NMES group but after 6 months statistically significant improvement was determinant only in mirror group(p:0.032). FIM was improved in three groups after treatment, but after 6 months improvement detected only in mirror group (p < 0,05). Spasticity ( MAS), was reduced only in the mirror group (p < 0,05). Hand skills ( NHPT) were improved only in mirror group and this improvement continued 6 months after the treatment ( p< 0,05). Quality of life was improved in both groups after treatment, but it was more in the mirror group. Conclusions: Aplication of NMES in front of a mirror is more effective on upper extremity and hand motor and functional development, hand skills and spasticity than NMES and standart theraphies of rehabilitation. This effect continues at 6 months after treatment.
Basaran PO¹*, Bolukbasi A² and Kutlay S²
Abbreviations: NMES: Neuromuscular Electrical Nerve Stimulation; MAS: Modified Ashworth Scale; FIM: Functional Independence Measurement; NHP: Nottingham Health Profile; NHPT: Nine Hole Peg Test.
Introduction
Impairment in upper extremity function is one of the main causes of disability in patients with post-stroke hemiplegia. This impairment is not only affects the daily life activities but also affects the patients’ quality of life. One of the main objectives in stroke rehabilitation is to acquire independence in daily living activities. Because of that hand rehabilitation in stroke patients is important for us.
A number of interventions have been published evaluating the effect of various rehabilitation methods in improving upper-extremity motor control and functioning, such as exercise training of the paretic arm, impairment- oriented training of the arm, functional electric stimulation, robotic-assisted rehabilitation, and bilateral arm training [1, 2, 3, 4, 5].
Change in somatosensory input has been shown to affect cortical organization in healthy subjects and subjects with brain injury [6]. Treatment with Neuromuscular electrical nerve stimulation (NMES) to the median nerve performed during functional magnetic resonance imaging (fMRI) in healthy subjects has been shown to activate the primary sensory and primary motor regions of the brain in the contralateral to the stimulation [7]. More recent studies showed that NMES has significant improvement in functional activity [8].
It has been suggested that mirror therapy is a simple, inexpensive and, most importantly, patient-directed treatment that may improve upper-extremity function. The findings from studies which was made by functional magnetic resonance supports this theory [9, 10].
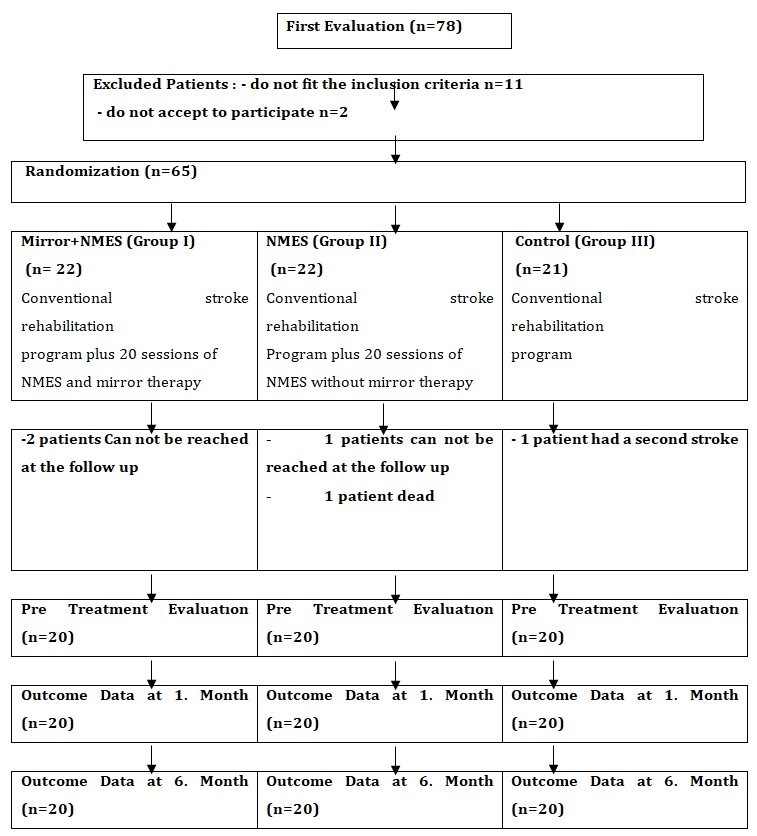
On the other hand there is no systematic study which investigates mirror and NMES therapy effects on upper extremity functional recovery and quality of life of. The purpose of this study was to assess the effectiveness of mirror and NMES therapyh in enhacing the upper extremity and hand motor and functional recovery, spasticity, and hand-related functioning and quality of life of patients after stroke and also wether a long term effect at 6 months after treatment (Figure 1).
Methods
Participants
This trial included 60 inpatients with hemiparesis after stroke (mean age 61,45) from July 2005 to September 2008 all of whom met the study criteria. Stroke was defined as an acute event of cerebrovascular origin causing focal or global neurologic dysfunction lasting more than 24 hours,17 as diagnosed by a neur_o_logist and confirmed by computed tomography or magnetic resonance imaging. The protocol was approved by the Ankara University Ethics Committee.
İnclusion Criterias 1) had a first episode of unilateral stroke with hemiparesis 2)Over the age of 18 3) des not have Concomitant non-cerebellar or brainstem lesion 4) have stable medical condition 5) were able to understand and follow simple verbal instructions Exclusion Criterias 1)Had contraindication for electrical nerve stimulation application such as pregnancy and pacemaker 2) had vision problems prevent to see the mirror 3) reduction in the affected extremity force with other neurological diseases 4) had severe cardiac arrhythmia, parkinson’s disease, epileptic seizures 5) had severe cognitive disorders
Study Design
This trial was planned as a randomized controlled assessor-blinded trial. All assessments were performed by the same investigator,who was blinded to the treatment assignment. Blinding of the patients or physical therapist was not possible because of the nature of the treatment. Patients were randomly assigned to three groups using a computer-generated random number (Figure 1). Blocks were numbered, and then a random-number generator program was used to select numbers that established the sequence in which blocks were allocated to one or the other group. A medical doctor who was blinded to the research protocol and was not otherwise involved in the trial operated the random number program.
Intervention
All patients participated in a conventional stroke rehabilitation program, 5 days a week, 1 to 4 hours a day, for 4 weeks. The conventional program is patient-specific and consists of neurodevelopmental facilitation techniques, physiotherapy, occupational therapy. For the same period, the mirror group received an additional 30 minutes of mirror therapy program.
İn the mirror group, patients were seated close to a table on which a mirror (35x35cm) was placed vertically. The involved hand was placed behind the mirror and the noninvolved hand in front of the mirror. The practice consisted of nonparetic-side wrist and finger flexion and extension movements while patients looked into the mirror, watching the image of their noninvolved hand, thus seeing the reflection of the hand movement projected over the involved hand. Patients could see only the noninvolved hand in the mirror; otherwise, the noninvolved hand was hidden from sight. During the session patients were asked to try to do the same movements with the paretic hand while they were moving the nonparetic hand. After the exercises electrical nerve stimulation was applied to the hemiparetic hand for 30 minutes and patients look into the mirror watching the image of their noninvolved hand during stimulation. İn the NMES group mirror was cover with a cloth exercises and NMES continued. The control group performed the same exercises for the same duration without mirror and NMES application. The same therapist delivered the mirror or sham treatment to the patients.
Main Outcome Measures
Brunnstrom motor staging for upper extremity and hand, Modified Ashworth Scale (MAS), Functional Independence Measurement (FIM) self-care items of the FIM instrument), Nottingham Health Profile (NHP), Nine hole peg test (NHPT), superficial sense, deep sense (two point discrimination, steregnosia, graphestesia, joint position sense) was measured at 0 months (pretreatment), 4weeks (posttreatment), and 6 months (follow-up). Pretreatment and posttreatment assessments were performed while patients were in the rehabilitation programme in hospital 6 month assessment were performed after the discharge. All patients invited to the hospital by phone.
Motor Recovery
Brunnstrom upper extremity and hand scales was used in this trial. Brunnstrom defined 6 sequential stages of motor recovery and described how the hemiplegic arm and hand progress through these stages as a method for assessing recovery [11]. Lowest stage Level I(flaccidity) highest stage level VI (all prehensile types under control). Higher Brunnstrom scores indicate better motor recovery.
Spasticity
The MAS was used to grade the spasticity of the wrist flexor muscles. The MAS is a 5-point ordinal rating scale. MAS scores range from 0 to 4: a MAS score of 0 represents “no increase in muscle tone,” and a score of 4 is “limb rigid in flexion or extension12.
Hand Releated Motor Functioning
FIM
İn this trial we used the self carepart of FIM. The FIM is a composite measure consisting 18 items assessing 6 areas13 . Each item is scored on a 7-point Likert scale indicative of the amount of assistance required to perform the item.
Nine Hole Peg Test
Fine motor function was evalated by Nine Hole Peg Test [14]. Patiens were asked to put of and put on 9 pieces of roller wood from the board, and time was calculated.
Quality of Life
The Quality of Life was assessed by Nottingham Health Profile (NHP). Turkish validation of this form was done [15]. NHP consists of 38 questions in 6 domains (energy, pain, emotional reactions, sleep, social isolation and physical mobility). Each domain scores range from 0 to 100.
Superficial Sense
Tactile sense was assessed by cotton touch. İt was scored as normal, abnormal and anesthetic.
Deep Sense
Two point discrimination: İt was assessed from the third finger distal part both anterior and posterior sides [16, 17]. While the patients eyes were shut, an esthesiometer was touched and asked to the patient feel one point or two. Under 17 milimeters was accepted as normal.
Steregnosia: Patients with their eyes closed asked to recognıse the items put on their hands. 12 items on different sizes and shapes are used for this evaluation( bottle cap, box, cotton, eraser, pen, key, screwdriver, screw, coin, spoon, safety pin, clock) [18].
Graphestesia: Patients with their eyes closed asked to recognıse the letter written on their hand. İt was recorded as normal or abnormal [16, 17].
Joint position sense: Proprioceptive sense was evaluated in this trial. Patients with their eyes closed asked to recognıse the thumb position of hand and feet. İt was recorded as normal or abnormal.
Statistical Analysis
The statistical evaluation of data “SPSS 11.5 Statistical Programme” was used. Chi-square test was used for categorical data. Cochran q test was used if there is a statistically significant difference between the pretreatment and after treatment results in each group itself. Kruskall Wallis Analysis of Variance was used between groups of treatment effectiveness. İf there is a statistically significant difference between groups Mann Whitney U Test was used to in order to determine the difference. Significance was set at .05.
Results
Demographic and clinical characteristics of the 3 groups are presented in Table 1. Demographic and clinical characteristics of baseline comparisions did not differ between groups except time since stroke. In control group patients are mostly in subacute stage but in mirror and NMES group patients are mostly in acute stage. After the treatment, Brunnstrom motor stage for hand and upper extremity improved in both mirror and NMES group but after 6 months statistically significant improvement was determinant only in mirror group (Table 2). FIM was improved in three groups after treatment, but after 6 months improvement detected only in mirror group (p < 0,05). Spasticity ( MAS), was reduced only in the mirror group (p < 0,05). At the pretreatment evaluation of nine hole peg test (NHPT) were applied 8 patients in Mirror group, 4 in NMES group, 7 in control group. Other patients can not hold the board. At the 1. Month 3 more patients from mirror group, 2 more from NMES group could completed the test. Same patients completed the NHPT at the 6. Month evaluation. NHP Test duration improved only in mirror group and this improvement continued 6 months after the treatment ( p< 0,05). Quality of life (NHP) was improved in all groups after treatment, but it was more in the mirror group. Baseline, 1.month and 6. Month comparisions did not differ between groups for evaluations of superficial sense and deep sense (two point discrimination, steregnosia, graphestesia, joint position sense). In patients with disorders about these parameters: disorders continued after treatment. Except two point discrimination sense we can not state an improvement after treatment but it was statistically unsignificant.
| Mirror+NMES (n=20) | NMES (n=20) | Control (n=20) | p | |
|---|---|---|---|---|
| Age(year) mean±SD | 61±9.17 | 60.35±10.28 | 63±9.42 | 0.123 |
| Time since stroke (month)mean±SD | 13.35±8.25 | 4.25±7.17 | 10.4±7.54 | *0.033 |
| Sex (%) Woman/Man | 45/65 | 45/65 | 40/60 | 0.934 |
| Paralayzed Side R/L | 60/40 | 55/45 | 55/45 | 0.934 |
| Etiology(%) lsc/Heam | 90/10 | 95/5 | 85/15 | 0.362 |
| Dominant side (%)R/L | 95/5 | 100/0 | 100/0 | 0.362 |
| Brunnstron stage(Hand) | 3.00±1.65 | 2.30±1.65 | 3.00±2.07 | 0.282 |
| Brunnstron stage (UE) | 3.15±1.66 | 2.45±1.79 | 3.25±2.12 | 0.294 |
| FIM self care | 18.40±8.11 | 16.45±8.91 | 19.90±12.34 | 0.655 |
| MAS elbow flexor | 1.15±1.22 | 0.85±1.08 | 0.95±1.31 | 0.72 |
| MAS wrist and hand flexor | 1.25 ±1.20 | 0.95±1.09 | 0.85±1.30 | 0.885 |
Table 1: Demographic Characteristics of the Mirror, NMES and Control Groups and Baseline Measurements. Egitim meslek lezyon bolge
| Mirror+NMES (n=20) | NMES (n=20) | Control (n=20) | |
|---|---|---|---|
| UE 0.month Mean±SD | 3.15±1.66 | 2.45±1.79 | 3.25±2.12 |
| UE 1.month Mean±SD | 4.10±1.55 | 3.10±1.94 | 3.30±2.17 |
| UE 6.month Mean±SD | 4.55±1.53 | 3.15±1.95 | 3.35±2.15 |
| p | *0.000 | *0.000 | 0.472 |
| Hand 0.month Mean±SD | 3.00±1.65 | 2.30±1.65 | 3.00±2.07 |
| UE 1.month Mean±SD | 3.95±1.76 | 2.85±1.81 | 3.15±2.15 |
| UE 6.month Mean±SD | 4.30±1.55 | 2.85±1.81 | 3.20±2.11 |
| p | *.000 | *.000 | 0.115 |
Table 2: Comparing Brunnstrom UE scales at pretreatment ,1.month and 6. Month after treatment in groups.
Discussions
This study shows that mirror therapy and NMES in addition to a conventional rehabilitation program was more beneficial in terms of motor recovery and hand-related functioning than a similar treatment without mirroring or NMES. The beneficial effect on hand functioning started at posttreatment in mirror and NMES group but continued during the 6-month follow-up evaluation only in the mirror group. However, spasticity was decreased only in mirror group and this was continued during the 6-month follow-up evaluation .
Hemiparesis due to stroke is one of the most common neurological problems all over the world. As a result of advances in acute treatment of stroke, the number of patients living after stroke is increasing rapidly for this reason the number of patients in need of rehabilitation is increased. But there is no consensus about the effectiveness of the treatment options.
Several underlying mechanisms for the effect of mirror therapy on motor recovery after stroke have been proposed. For example, Altschuler, et al. [19] suggested that the mirror illusion of a normal movement of the affected hand may substitute for decreased proprioceptive information, thereby helping to recruit the premotor cortex and assisting rehabilitation through an intimate connection between visual input and premotor areas. Stevens, et al. [20] suggested that mirror therapy related to motor imagery and that the mirror creates visual feedback of successful performance of the imagined action with the impaired limb. Mirror theraphy thought to trigger neuronal connectivity in the motor cortex about the motor imaginary area. Findings obtained from studies with functional magnetic resonance is support this theory [21, 22].
Treatment with Neuromuscular electrical nerve stimulation (NMES) has been shown to activate the primary sensory and primary motor regions of the brain in the contralateral to the stimulation [7, 23]. More recent studies [24] purpose that NMES has provides the motor facilitation and reeducation in brain activities. Mirjana, et al. [25] upper extremity functions improved with NMES therapy and he suggested that his improvement may be depending on the effect of NMES on brain plasticity. Our results are similar with Mirjana and we suppose that mirror and NMES therapy improves hand and upper extremity functions by improving brain plasticity.
Study Limitations
Acute subacute and chronic hemiplegic patients involved to this study. If times since stroke is smilar between groups the results would be more accurate to generalize. We have a small sample size . We need more studies on large populations.
Conclusion
In our group of stroke patients, hand function improved more after mirror therapy and NMES theraphy in addition to a conventional rehabilitation program compared with a control treatment directly after 4 weeks of treatment whereas improvement continued only with mirror theraphy at the 6-month follow-up. Spasticity was decreased only with mirror theraphy.Quality of life of patients was improved in patients but it was more with mirror theraphy. These results show that combined mirror and NMES theraphy could be effective at restoring motor function poststroke and that it has potentiel use during the rehabilitation of poststroke patients.
References
-
Kwakkel G, Wagenaar RC, Twisk JW, Lankhorst GJ, Koetsier J (1999) Intensity of leg and arm training after primary middle-cerebralartery stroke: a randomised trial. Lancet 354(9174): 191-196.
-
Platz T, Eickhof C, Van Kaick S, Engel U, Pinkowski C, et al. (2005) Impairment-oriented training or Bobath therapy for severe arm paresis after stroke: a single-blind, multicentre randomized controlled trial. Clin Rehabil 19: 714-724.
-
Ring H, Rosenthal N (2005) Controlled study of neuroprosthetic functional electrical stimulation in sub- acute post-stroke rehabilitation. J Rehabil Med 37(1): 32-36.
-
Masiero S, Celia A, Rosati G, Armani M (2007) Robotic- assisted rehabilitation of the upper limb after acute stroke. Arch Phys Med Rehabil 88(2): 142-149.
-
Summers JJ, Kagerer FA, Garry MI, Hiraga CY, Loftus A, et al. (2007) Bilateral and unilateral movement training on upper limb function in chronic stroke patients: a TMS study. J Neurol Sci 252(1): 76-82.
-
Nudo RJ, Plautz EJ, Frost S (2001) Role of adaptive plasticity in recovery of function after damage to motor cortex. Muscle Nerve 24(8): 1000-1019.
-
Spiegel J, Tintera J, Gawehn J, Stoeter P, Treede R (1999) Functional MRI of human primary somatosensory and motor cortex during median nerve stimulation. Clinical Neurophysiology 110(1): 47-52.
-
Kimberly J, Auerbach J, Jeanne M (2004) Electrical stimulation driving functional improvements and cortical changes in subjects with stroke. Exp Brain Res 154(4): 450-460.
-
Ramachandran VS, Rogers Ramachandran D (1996) Synaesthesia in phantom limbs induced with mirrors. Proc R Soc Lond B Biol Sci 263(1369): 377-386.
-
Ramachandran VS, Hirstein W (1998) The perception of phantom limbs. The D. O. Hebb lecture. Brain 121(9): 1603-1630.
-
Sawner K, Lavigne J (1992) Brunnstrom’s movement therapy in hemiplegiaia neurophysiological approach. Philadelphia: JB Lippincott.
-
Bohannon RW, Smith MB (1987) Interrater reliability of a Modified Ashworth Scale of muscle spasticity. Phys Ther 67(2): 206-207.
-
Kucukdeveci AA, Yavuzer G, Elhan AH, Sonel B, Tennant BA (2001) Adaptation of the Functional Independence Measure for use in Turkey. Clin Rehabil 15(3): 311-319.
-
Sunderland A, Thinson D, Bradley L, Hewer RL (1989) Arm function after stroke:an evaluation of grip strenght as a measure of recovery and a prognostic indicator. J Neurol Neurosurg Psychiatr 52(11): 1267-1272 .
-
Kucukdeveci AA, McKenna SP, Kutlay S, Gursel Y, Whalley D, et al. (2000) The development and psychometric assessment of the Turkish version of the Nottingham Health Profile. International Journal of Rehabilitation Research 23(1): 31-38.
-
Corkin S, Milner B, Rasmussen T (1970) Somatosensory thresholds: contrasting effects of postcentral-gyrus and posterior parietal-lobe excisions. Arch Neurol 23(1): 41- 58.
-
Carey LM, Matyas TA, Oke LE (1993) Sensory loss in stroke patients: effective training of tactile and proprioceptive discrimination. Arch Phys Med Rehabil 74(6): 602-611.
-
Dannenbaum RM, Jones LA (1993) The assessment and treatment of patients who have sensory loss following cortical lesions. J Hand Ther 6(2): 130-138.
-
Altschuler EL, Wisdom SB, Stone L, C Foster, D Galasko, et al. (1999) Rehabilitation of hemiparesis after stroke with a mirror. Lancet 353(9169): 2035-2036.
-
Stevens JA, Stoykov ME (2003) Using motor imagery in the rehabilitation of hemiparesis. Arch Phys Med Rehabil 84(7): 1090-1092.
-
Garry MI, Loftus A, Summers JJ (2005) Mirror, mirror on the wall: viewing a mirror reflection of unilateral hand movements facilitates ipsilateral M1 excitability. Exp Brain Res 163(1): 118-122.
-
Giraux P, Sirigu A (2003) Illusory movements of the paralyzed limb restore motor cortex activity. Neuroimage 20(Suppl 1): S107-S111.
-
Kampke K, Jones R, Auer D (2000) Frequency dependence of the functional MRI response after electrical median nerve stimulation. Hum Brain Mapp 9(2): 106-114.
-
Kowalczewski J, Gritsenko V, Ashworth N (2007) Upper extremity functional electric stimulation assisted exercises on a workstation in the subacute phase of stroke recovery. Arch Phys Rehab 88(7): 833-839.
-
Mirjana B, Dejan B, Sinkjear T (2003) Clinical evaluation of functional electrical therapy in acute hemiplegic subjects. Journal of Rehab R&D 40(5): 443-454.
- Electrolyte Considerations for Athletes
- Comprehensive Rehabilitation in Adults with Diabetic Peripheral Neuropathy: A Literature Review on Frequency, Intensity, and Duration Parameters
- Exercise Duration and Its Association with ADHD Symptom Severity in Children and Adolescents: A Parent-Reported Survey Study
- Adaptation of the Adult Neurophysiology of Pain Questionnaire for Use in Pediatrics
- A Non-Pharmacological Multidisciplinary Pain Program within a Hospital Wellness Program: A Mixed Methods Study
- The Effect of Frenkel's Exercise with PNF on Functional Reach in Stroke Survivors: A Randomized Control Trial