Does Arthroscopic Lateral Retinacular Ligament Release in Patellofemoral Pain Syndrome Improve the Pain: Comparing the Techniques of Electrocautery or Scissors
Introduction: Pain is the main indication for surgical treatment of release in patellofemoral pain syndrome of knee. Arthroscopic lateral retinacular release in patellofemoral pain syndrome using the electrocautery or a new technique for arthroscopic lateral release with scissors. In this study we compare the VAS scale before and after the surgery in 1 month in electrocautery and scissors group and the amount of hemorrhage and time of release between the groups. Methods: 120 patients included in this prospective randomized controlled study. Inclusion criterias are over the age of eighteen and have anterior knee pain syndrome. Tightness in lateral part of knee. Despite receiving conservative treatment for 6 months. Exclusion Criteria: Diseases that prolong bleeding time. Drugs that prolong bleeding time. Abnormal APTTINR levels. Patients underwent anterior cruciate reconstruction surgery, microfracture surgery, meniscus repair surgery; synovectomy due to inflammatory diseases is excluded from the study. In this study 120 (42M 78W med age 50,24 ± 15,37 ) patients divided into three groups which was similar in age and sex. All patients underwent standard arthroscopic surgery for patellofemoral knee syndrome and meniscal debridement Group 1(Electrocautery) (n:40) Lateral Retinacular Ligament (LRL) was released with electrocautery. Group 2(Scissors)(n:40) LRL was released with Scissors .Group 3(Control)(n:40) LRL was preserved. Results: There was no difference between the groups in terms of socio-demographic characteristics. All lateral ligaments releases were performed under tourniquet. The release is not considered to be complete unless the patella can be stood on its medial edge without difficulty. In all patients, surgery duration was recorded. To calculate the amount of bleeding the blood in the drainage tube was recorded for 24 hours after surgery. For 80 patients based on clinical examination at surgery and in the immediate postoperative period, all releases were felt to be adequate. For all groups total bleeding at 24h postoperatively is the statistically same (p:0.8). In first 8 hours the amount of bleeding is more than scissors group (p:0.002). Lateral release time is longer in electrocautery group (370 seconds) than in scissors group (22 seconds). In release with electrocautery sometimes we used additional techniques for enough release. There was no difference between groups in terms of complications such as deep vein thrombosis, hemarthrosis or severe complications. Visual analog scale (VAS) was used to assess the pain in all patients before surgery and after surgery in 1 month. There were no statistically differences between the VAS in the groups before the surgery. VAS was improved in all groups after surgery, but the improvement was less in control group and this change is statistically significant. At 1 month after the surgery there was no statistically significant difference in electrocautery and scissors group. Conclusion: In this study the amount of bleeding was the same in the groups but surgery duration was longer in electrocautery group. Pain decreased after surgery at all patients but we find further improvement with lateral retinacular release. Lateral retinacular release decreases pain. Our new technique for intraarticular arthroscopy guided lateral retinacular release uses with scissors which is simple, effective, rapid and have resulted a few surgical complications such as superficial skin infection which responds oral antibiotics. Electrocautery is difficult and needs experience.
Introduction
Anterior knee pain is considered by orthopedic surgeons to be a difficult disease to treat. Treatment methods have been described since Roman times (Galen 129-200). As the extensor mechanism and patellofemoral joint were understood, the problem began to be solved, but there are still questions that need to be investigated. One of these questions is whether lateral retinacular release can be a treatment method for anterior knee pain. While many authors recommend lateral release together with proximal or distal realignment procedures, it is currently said that isolated lateral release can be recommended in cases where lateral tension is alone [1].
Pain is the main indication for surgical treatment of release in patellofemoral pain syndrome of knee. Arthroscopic lateral retinacular release in patellofemoral pain syndrome using the electrocautery or a new technique for arthroscopic lateral release with scissors. In this study we compare the VAS scale before and after the surgery in 1 month in electrocautery and scissors group and the amount of hemorrhage and time of release between the groups.
Methods
120 patients included in this prospective randomized controlled study. Inclusion Criteria: Over the age of eighteen and have anterior knee pain syndrome. Tightness in lateral part of knee. Despite receiving conservative treatment for 6 months. Exclusion Criteria: Diseases that prolong bleeding time. Drugs that prolong bleeding time .Abnormal APTT-INR levels. Patients underwent anterior cruciate reconstruction surgery, microfracture surgery, meniscus repair surgery; synovectomy due to inflammatory diseases is excluded from the study. In this study 120 (42M 78W) patients divided into three groups which were similar in age and sex. All patients underwent standard arthroscopic surgery for patellofemoral knee syndrome and meniscal debridement Group 1(Electrocautery) (n:40) LRL was released with electrocautery. Group 2(Scissors) (n:40) LRL was released with Scissors .Group 3(Control)(n:40) LRL was preserved.
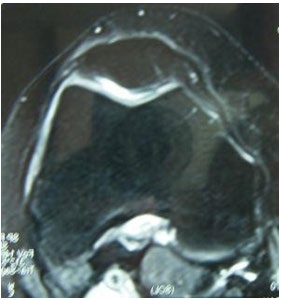
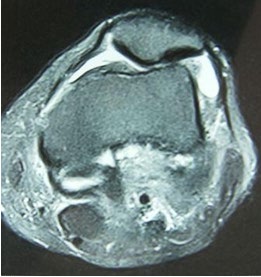
The aim of this study is to determine the effect of the surgical method on the amount of bleeding and duration of lateral release in patients undergoing lateral release. Patients who applied to Hacettepe University Faculty of Medicine (HUTF) orthopedics department outpatient clinic between June 2006 and August 2008 were included in the study. Patients over the age of 14 with anterior knee pain, lateral knee tension and conservative treatment for 6 months were included in the study. Patients with a disease that prolong bleeding time, taking drugs that prolong bleeding time, and those with normal APTT-INR values were not included in the study (Figures 1 & 2).
140 patients meeting these criteria were included in the study. All these patients have not been operated around the knee before. In addition, patients who underwent interventions to increase intra-knee hemorrhage such as synovioectomy, microfracture, ligament reconstruction, and meniscus repair were excluded from the study.
42 of the patients included in the study were male and 78 of them were female. The average age of the patients between the ages of 18-74 was 50.14 ± 14.17. Two patients who underwent lateral release had patellar dislocation. The patients were followed in 3 groups. The first group was patients who underwent lateral release with cautery were included. The second group included patients who had lateral release with scissors. In the third group taken as the control group to detect intra-knee fluid after arthroscopy and bleeding after standard arthroscopy. 80 patients were randomly distributed. There were 40 patients in the first group, 40 patients in the second group, and 40 patients in the third group.
Patellar mobility, Q angle, knee range of motion (ROM) was measured in the pre- and postoperative examination of the patients in the study group. In addition, preoperative complete blood count, blood biochemistry, aptt, and INR count were performed in all patients included in the study.
For radiological evaluation, anteroposterior knee X-ray, lateral knee X-ray at 30 degrees of flexion, patella skyline radiography (Merchant) was taken in all of them for radiological evaluation. Knee MRIs of all patients were evaluated in order to detect additional pathologies within the knee.
All patients were evaluated arthroscopically using a tourniquet under general or regional anesthesia. Chondroplasty using laser and radiofrequency was performed in patients with cartilage damage. Partial meniscectomy was performed in patients with central meniscal tears. Patients who underwent meniscus procedures, synovectomy, ACL repair, and microfracture that increase the possibility of bleeding were excluded from the study. Due to bleeding and fluid extravasation, lateral release was applied last. A needle inserted through the lateral superior pole of the patella was placed as a guide showing the estimated location of the lateral superior genicular artery. Loosening times with scissors or cautery were calculated in seconds. It was seen that lateral loosening with arthroscope was sufficient. After the operation, the fluid in the knee was aspirated as much as possible. A drain was placed in all patients. A sterile bandage was placed to push the patella laterally to the medial side of the patients who underwent lateral release, was wrapped compressively and a tourniquet was opened.
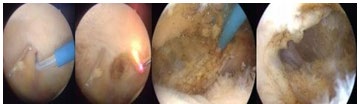
While lateral loosening was applied with scissors, the needle was inserted from the upper pole of the patella. The area to be loosened was seen with the arthroscope. Scissors were inserted through the lateral portal. The lateral retinaculum was cut as far as the needle was. The medial migration and medial rotation of the patella were examined. If the relaxation was insufficient, relaxation was performed again (Figures 3 & 4).
![Figure 3: Lateral release with Yerys technique [2].](/fulltextimages/6103/fig_3.jpeg)
While applying lateral loosening with cautery, after the needle marked the upper pole of the patella, we brought the 90-degree cautery tip from the lateral portal to the retinaculum. With cautery, we cut the lateral retinaculum up to the mark. It was checked whether the loosening was sufficient or not. As a criterion of adequacy, the patella can be eversioned 45 degrees after relaxation or the medial translation of 25% of the patella was taken. If it was insufficient, loosening was performed again with cautery or scissors. A sterile bandage was placed on the lateral of the patella and the patella was pushed medially in patients who underwent lateral release after surgery (Figure 5 & 6).
![Figure 4: Lateral release with Michael J. Lord technique [3].](/fulltextimages/6103/fig_4.jpeg)
Thrombolytic agents were not started in the operated patients because early mobilization was initiated in the postoperative period. First generation cephalosporin (cefazolin 1g) was given to all patients as prophylactic four times for 24 hours. Pain control was provided by giving NSAIDs and narcotic painkillers if necessary. Pain and edema were prevented by applying ice on the knee at intervals of 24 hours and 2 hours.
During the postoperative drainage follow-up of the patients, the fluid collected at 8-hour intervals was taken into the measuring cup and measured. The amount of bleeding at the 8th, 16th and 24th hours was calculated. Drains were removed 24 hours postoperatively. Knee exercises that strengthen the quadriceps were started in the bed. All patients were mobilized by standing up. The medial pushing of the patella was continued for 2 weeks.
Results
Of the 120 patients participating in this study, 42 were male (35%) and 78 were female (65%). There was no statistically significant difference between the groups in terms of sociodemographic data (age, gender, comorbidity (hypertension, diabetes mellitus, depression, thyroid disease) and additional drugs they used. Right knee arthroscopy was performed in 63 patients and left knee arthroscopy in 57 patients participating in the study. There is no statistically significant difference between the right and left knees relaxed by both methods. When the range of motion of the knees to be applied lateral relaxation of 80 patients were compared, there was no statistically significant difference between the two groups.
When the clinical examinations, radiographs, magnetic resonance films and reports of the patients were evaluated, anterior cruciate tears, medial and lateral meniscus tears, chondromalasias, and free bodies were detected as an additional diagnosis. Meniscus partial debridement, stage 1-2 chondromalastic patients, and patients with free body excisions who underwent standard arthroscopy and did not increase the amount of bleeding were included in the study, and when these criteria were taken into account, no statistically significant difference was found between the study groups.
In the early postoperative period, superficial skin rash was observed in 2 patients. One patient from each group was treated with oral antibiotics with a pre-diagnosis of cellulite. Patients who were called for control after 1 week showed improvement.
In order to evaluate postoperative hemarthrosis, which is one of the main research topics of the study, there is no statistically significant difference between the minimum and maximum amount of fluid and total bleeding in all three groups. However, when the fluids collected at time intervals of 8 hours were compared, a statistically significant difference was found between the groups that were loosened with scissors and the other groups. While the amount of fluid collected in the first eight hours of loosening with scissors was 53.03 ± 17.71 milliliters, the fluid from the first eight hours of relaxation with cautery was 43.52 ± 19.71 milliliters; in control patients it was 43.5 ± 19militers. The amount of bleeding is higher in patients who use scissors in the first 8 hours.
When the second parameter evaluated in the study, the relaxation times, were evaluated in seconds, it was seen that the lateral release with scissors was superior to the relaxation with cautery. Loosening is completed in 24 seconds with scissors on average, while it is completed in 380 seconds with cautery. This difference was found to be statistically significant.
Visual analog scale (VAS) was used to assess the pain in all patients before surgery and after surgery in 1 month. There was no statistically difference between the VAS in the groups before the surgery. VAS was improved in all groups after surgery, but the improvement was less in control group and this change is statistically significant. At 1 month after the surgery there was no statistically significant difference in electrocautery and scissors group (Tables 1 & 2).
| Pre surgery | After Surgery (1month) | p | |
|---|---|---|---|
| Electrocauter (group1) | 7,35±0,9 | 5,20±1,07 | 0.001 |
| Scissors (group2) | 7,35±0,9 | 4,60±1,07 | 0.001 |
| Control (group3) | 6.50±1,1 | 5,60±1,03 | 0.001 |
Table 1: Comparing VAS after surgery.
| Electrocauter (group1) | Control (group3) | p | |
|---|---|---|---|
| VAS 1-2 | 2,15±0,85 | 0.9±0.1 | 0.023 |
| Electrocauter (group1) | Scissors (group2) | p | |
| VAS 1-2 | 2,15±0,85 | 2,75±0,7 | 0.91 |
| Scissors (group2) | Control (group3) | p | |
| VAS 1-2 | 2,75±0,7 | 0.9±0.1 | 0.006 |
Table 2: Comparing effects of surgery between groups.
Conclusion
In a study published by Panni AS, et al. [4]. In 2005, long-term results of lateral relaxation were evaluated. 100 patients, 23 years old, were evaluated with the setting. While 50 patients had a taut lateral retinaculum, the other 50 patients had patellar instability. The cartilages were evaluated using the inferolateral and super lateral portals under the tourniquet. Cartilages of Outer Bridge 2-3-4 are shaved. The subcutaneous tunnel was opened through the inferolateral portal. The lateral retinaculum capsule, synovial tissues, and distal structures of the vastus lateralis were cut up to 2 cm superior to the patella. The ability to turn the patella outwards by 90 degrees is considered sufficient loosening. If the relaxation is insufficient, it is cut 1-2 cm more from the distal and proximal. As a result, it was stated that application of lateral release to painful but stable patellae yields better results and lateral release can be added to patellar alignment-providing operations for unstable patella. Hemarthrosis was encountered at a rate of 5 percent. However, in the article published by Fulkerson in 2002, it was shown that pain may occur due to medial subluxation in relaxation where excessive lateral relaxation is performed [4, 5, 6, 7, 8].
In the study conducted by Doral, et al. [9] treatment methods for bipartite patella, one of the causes of anterior knee pain in adolescence, were discussed. In non-surgical treatments, rest, interrupting sports activities, non-steroid painkillers, physical therapy, device immobilizing the knee at 30 degrees flexion, and local steroid injections were counted. It has been stated that in cases where these treatment regimens cannot provide treatment, fragment excision, fragment fixation or lateral release may be applied. Especially lateral relaxation is recommended in these patients because of its effect in reducing pain and accelerating healing. In this study, while vastus lateralis relaxation is performed while lateral relaxation is performed, in our study, in order not to disturb the muscle balance; In order to avoid medial subluxation of the patella; vastus lateralis fibers are preserved. In addition, it reduces the risk of injury to the upper lateral geniculate artery in the upper pole of the patella [9, 10, 11, 12].
In a study conducted by Çalpur, et al. [13]. In 2004, 169 patients with a pre-diagnosis of lateral compression syndrome underwent lateral release with a hook knife through the anterolateral portal. Arthroscopically, femoral and patellar cartilage injuries were evaluated. Before and after the operation, patella compliance angle was checked. The compliance angle decreased from -16 to +7 on average. They stated that anterior knee pain improved with lateral release in young and elderly patients. They found an increase in cartilage lesions with age. They attributed the fact that although the patella was thicker, there were more severe cartilage lesions than the femoral condyle, the larger femoral cartilage surface. The most important complication seen in patients with lateral release is fibrosis of the lateral release area. They state that with local corticosteroids, fibrosis passes. They state that hemarthrosis and hematoma, which are the most important complications of lateral release, were never seen. In our study, no fibrosis or lateral adhesion was observed. This may be due to the bandage pushing the patella placed after lateral release and early mobilization. Although we did not control bleeding, hemarthrosis and hematoma were not observed in our patients after sufficient release. This was attributed to the loosening up to the upper pole of the patella and the absence of further incision, the absence of an acute bleeding focus, the use of compressive dressing before the tourniquet was opened, and the hemorrhage remaining for a day [7, 9, 13, 14].
In this study the amount of bleeding was the same in the groups but surgery duration was longer in electrocautery group. Pain decreased after surgery at all patients but we find further improvement with lateral retinacular release. Lateral retinacular release decreases pain. Our new technique for intraarticular arthroscopy guided lateral retinacular release uses with scissors which is simple, effective, rapid and have resulted a few surgical complications such as superficial skin infection which responds oral antibiotics. Electrocautery is difficult and needs experience.
Conflicts of Interest
No benefits or funds were received in support of this study. The authors report no conflict of interests
References
-
Fulkerson JP (1994) Patellofemoral Pain Disorders: Evaluation and Management. J Am Acad Orthop Surg 2(2): 124-132.
-
Yerys P (1985) A Technique for Lateral Retinacular Release Arthroscopy: The Journal of Arthroscopic and Related Surgery 1(4): 233-236.
-
Lord MJ, Maltry JA, Shall LM (1991) Thermal Injury Resulting from Arthroscopic Lateral Retinacular Release by Electrocautery: Report of Three Cases and a Review of the Literature. Arthroscopy 7(1): 33-37.
-
Panni AS, Tartarone M, Patricola A, Paxton EW, Fithian DC (2005) Long-term Results of Lateral Retinacular Release. Arthroscopy 21(5): 526-531.
-
Fulkerson JP, Schutzer SF (1986) After failure of conservative treatment for painful patello-femoral malalignment: lateral release or realignment?. Orthop Clin North Am 17(2): 283-288.
-
Fulkerson JE, Schutzer SE, Ramsby GR, Bernstein RA (1987) Computerized Tomography of the Patellofemoral Joint Before and After Lateral Release or Realignment. Arthroscopy 3(1): 19-24.
-
Fulkerson JP (2002) Diagnosis and treatment of patients with patellofemoral pain. Am J Sports Med 30(3): 447- 456.
-
Karamehmetoglu M, Ozturkmen Y, Azboy I, Caniklioglu M (2007) Kronik patellofemoral dizilim bozukluğu tedavisinde Fulkerson osteotomisinin yeri. Acta Orthop Traumatol Turc 41(1): 21-30.
-
Doral MN, Atay OA, Leblebicioğlu G, Tetik O (2001) Arthroscopic fixation of the fractures of the intercondylar eminence via transquadricipital tendinous portal. Knee Surg Sports Traumatol Arthrosc 9(6): 346-349.
-
Fulkerson JP (1983) Anteromedialization of the tibial tuberosity for patello-femoral malalignment. Clin Orthop 177: 176-181.
-
Fulkerson JP (1982) Awareness of the retinaculum in evaluating patello-femoral pain. Am J Sports Med 10(3): 147-149.
-
Atesok K, Doral MN, Lowe J, Finsterbush A (2008) Symptomatic Bipartite Patella: Treatment Alternatives. J Am Acad Orthop Surg 16: 455-461.
-
Calpur OU, Ozcan M, Gurbuz H, Turan FN (2005) Full arthroscopic lateral retinacular release with hook knife and quadriceps pressure-pull test: long-term follow-up. Knee Surg Sports Traumatol Arthrosc 13(3): 222-230.
-
O’neill DB (1997) Open Lateral Retinacular Lengthening Compared With Arthroscopic Release A Prospectıve, Randomızed Outcome Study. J Bone Joint Surg Am 79(12): 1759-1769.
- Electrolyte Considerations for Athletes
- Comprehensive Rehabilitation in Adults with Diabetic Peripheral Neuropathy: A Literature Review on Frequency, Intensity, and Duration Parameters
- Exercise Duration and Its Association with ADHD Symptom Severity in Children and Adolescents: A Parent-Reported Survey Study
- Adaptation of the Adult Neurophysiology of Pain Questionnaire for Use in Pediatrics
- A Non-Pharmacological Multidisciplinary Pain Program within a Hospital Wellness Program: A Mixed Methods Study
- The Effect of Frenkel's Exercise with PNF on Functional Reach in Stroke Survivors: A Randomized Control Trial