Effects of Shoulder Surgery Performed on Patients with Obstetric Brachial Plexus Palsy on Remodelling and Periscapular Muscles
Objective: Internal rotation contracture of the shoulder area developing on the follow-up of pediatric patients with obstetric brachial plexus palsy (OBPP) can lead to glenoidal and humeral head dysplasia and glenohumeral joint (GHJ) posterior dislocation. OBPP patients accompanied by the shoulder area problems and made early surgical intervention, long-term effects (> 2 years) of the balance between internal and external rotator muscle groups provided with tendon transfers and reduction of the joint on GHJ remodelling and on periscapular muscle development have been evaluated through magnetic resonance imaging (MRI) guided. Patients and methods: 14 patients with OBPP having had secondary shoulder surgery were placed retrospectively under examination to be evaluated in terms of GHJ remodelling, volumetric changes of internal (subscapularis) and external rotator muscles (infraspinatus and teres minor) groups. Current MRI of healthy sides is assessed in order to assess whether changes on patient group having preoperative and postoperative shoulder MR reviews of side with palsy are at the close rate to the healthy side. Proximal humeral head anterior ratio (PHHA) has been used for the assessment of subluxation in MRI reviews. Measured glenoid version (GV) changes have been examined in terms of seeing responses of glenoid dysplasia to surgical treatment and elliptical index (EI) changes have also been examined in terms of seeing responses of humeral head dysplasia to surgical treatment. Subscapularis (SS) and external rotators (ER) muscle groups have also been examined into areas in MRI scans and change amount has been determined by converting these values into volumetric data. Results: GV and ER values from examined parametric changes have shown statistically significant (p <0.05) change as being very close to healthy shoulder side values. In terms of last GV and ER values obtained, statistically significant difference couldn’t be found between the shoulder values of the side with palsy and the shoulder values of the healthy side. Namely, even though significant and positive changes after the surgery have been observed in terms of PHHA and SS, these values cannot catch the healthy side values. The most negative results in the study have been obtained in ER changes. Any statistically significant changes haven’t been observed in terms of ER volumetric changes after surgery. Conclusion: In the cases with OBPP accompanied by the shoulder problems it has been found that significant osseous remodelling has been provided with surgery of early secondary shoulder region in long-term follow-up
Introduction
Obstetric brachial plexus palsy (OBPP) which is one of the most important issues of the department of orthopaedics and obstetrics, is a multidimensional injury situation known since ancient times [1, 2, 3, 4, 5, 6, 7, 8, 9]. Important studies on the natural history were done and injury mechanisms involved in its aetiology were studied to clarify [10, 11]. Techniques and results of early shoulder surgical procedures performed on the patients with OBPP accompanied by shoulder problems have been many times the subject of research and publication [2, 3, 4, 5, 6, 7, 8, 9, 12, 13, 14]. Occurrence usually together of shoulder muscle contractures which can develop during follow-up and osseous deformities and studies in direction of not being a prognostic indicator of a single factor in the development of this pathology indicate us that this issue needs a multi- dimensional measurements in terms of surgery [15]. The purpose of this study is to reveal recoveries on the transfer of the latissimus dorsi which is internal rotator muscles of the shoulder area and of teres major as external rotator to the humeral head, on GHJ reduction, on glenoid remodelling of the secondary shoulder interventions including the subscapularis release and axillary nerve decompression and the humeral head remodelling, on subluxation of joint and periscapular muscle volume changes in patients with OBPP requiring surgical treatment.
Patients and Methods
Cases in the study were analyzed by retrospective analysis method. Performed shoulder area secondary surgical procedure by diagnosing OBPP between 08.06.2006 and 23.02.2010 in Hacettepe University Faculty of Medicine, Department of Orthopaedics and Traumatology, having preoperative and postoperative bilateral shoulder MRI taken after average of 41.8 months, 14 pediatric patients with close follow-up and adequate documentation have set the material by being included in the scope of the study. 9 of OBPP cases are female and 5 are male. The age distribution, length of follow-up and involvement sides of the patients is indicated in Table 1. According to this table, ages of the patients in the study stage vary between 5 and 11 and the average is calculated as 6.4; the ages during surgery vary between 13 and 82 months and the average is calculated as 28.4. The cases were evaluated clinically in controls at 3 and 6 months from the moment of d3iagnosis until the end of study. Length of radiological follow-up with MRI of the patients in the study varies between 29 months and 71 months. There is involvement of left side on 6 patients and involvement of the right side on 8 patients. Rate of involvement of right side were calculated higher (%57.1) in accordance with the literature [11].
| Patient number | Side (Right:+1, Left:-1) | Surgery age (Months) | Age (Year) | MR Follow-up time (Months) |
|---|---|---|---|---|
| I | -1 | 82 | 11 | 57 |
| II | -1 | 35 | 7 | 33 |
| III | 1 | 17 | 6 | 36 |
| IV | 1 | 21 | 5 | 41 |
| V | -1 | 13 | 5 | 35 |
| VI | -1 | 20 | 6 | 41 |
| VII | 1 | 14 | 5 | 36 |
| VIII | -1 | 15 | 6 | 39 |
| IX | 1 | 16 | 6 | 36 |
| X | 1 | 22 | 8 | 71 |
| XI | 1 | 26 | 6 | 50 |
| XII | 1 | 21 | 5 | 47 |
| XIII | -1 | 23 | 5 | 34 |
| XIV | 1 | 73 | 8 | 29 |
| Mean value | 28.4±21.6 | 6.4±1.7 | 41.8±11.2 |
Table 1: The age distribution, length of follow-up and involvement sides of the patients.
Release of subscapularis from insertion, open reduction of GHJ, combined transfer of teres major and latissimus dorsi as the external rotator to the humeral head and also axillary nerve decompression were performed as surgical procedure on the patients taken into the study. The patients were performed plaster of brachial plexus with external fixation in the pursuit of suture anchor fixation of tendon transfer. Patients with preoperative clinical examination, photographs, radiographs and MRI of the shoulder side with palsy were assessed in the follow-up period with MRIs of the shoulder side with palsy and healthy side taken at least 2 years later after the operation. Remodelling of the glenoid and humeral head in T2 sequences, muscular volumetric changes in T1 sequences were especially examined in scans. In MRI scans, values of side with palsy are taken into measurement between each other as preoperative and postoperative in terms of linear and volumetric parameters; in the current MRI scans, the differences between healthy side and side with palsy are taken into measurement between each other.
In the analysis of the data obtained in this study IBM SPSS Statistics 21.0 software package was used. Mann- Whitney U test was used to investigate whether there is a significant difference between values of preoperative and postoperative side with palsy and values of postoperative side with palsy- postoperative healthy side for osseous and muscular variables. In all applied tests significance level of p = 0.05 is grounded.
The Parameters Evaluated in this Study
a. GV (Glenoid version): This measurement was conducted to determine the glenoid dysplasia obtained in MRI shoulder axial sections taken by subtracting 90 degrees from the angle forming in the posteromedial in between the line passing through the most medial border of the scapula and the midpoint of glenoid fossa and, the line passing through the most anteromedial and the most posterolateral protrusions of the glenoid cartilage at the widest GHJ level.
b. PHHA (Proximal humeral head anterior): these are the values obtained as the ratio of the largest length of the humeral head diameter, staying at anterior of the line passing through the midpoint of the glenoid fossa and medial border of the scapula at the widest glenoid level, to the humerus in the same direction. This measurement was conducted to assess subluxation or dislocation degree of humeral head. Normal value should be around 50% [12].
c. EI (Elliptic index): It was evaluated as the ratio of the widest diameter of the humeral head at the widest level of GHJ in MRI shoulder axial sections taken to each other with the narrowest diameter. It was evaluated to determine whether humeral head was in elliptical or ovoid structure or not. Values close to 1 represent a more ovoid structure.
d. Muscular volumetric measurements (SS: Subscapularis, ER: External rotators): in MRI shoulder axial sections taken, especially in the images obtained in T1 sequences, planned muscular volume measurement was firstly made in a areal way at 1 pixel = 1 mm2 ratio by using Adobe Photoshop CS6 Extended software (Adobe Systems, San Jose, California). Then, change amounts are expressed as volume ratios by converting the areal ratios to volumetric ratio in (√x / √y)3. If it had been considered that the measurements at 1 pixel = 1 mm2 ratio for each patient was made and that it was studied in measurements with PACS system having same solubility for all patients, formation of interpatient statistical error could be prevented. This measurement has been made to determine postoperative muscular volume changes.
Evaluation of Parameters
In the study, parametric values were subjected to evaluation in the statistical sense with SPSS software after being saved in Excel Sheet Format. The criteria included in the evaluation are listed below. Comparing and averaging of GV values of preoperative and postoperative side with palsy and of postoperative side with palsy-healthy side. Comparing and averaging of PHHA values of preoperative and postoperative side with palsy and of postoperative side with palsy-healthy side. Comparing and averaging of EI values of preoperative and postoperative side with palsy and of postoperative side with palsy-healthy side. Comparing and averaging of SS and ER values of preoperative and postoperative side with palsy and of postoperative side with palsy-healthy side.
All MR measurements (angular, proportional and volumetric) were made on the PACS system. Angular and proportional values like GV, EI and PHHA are presented as examples in Figures 1 & 2. 2-dimensional surface area in DICOM section-data was calculated in 1 pixel= 1 mm2 in order to assess the volumetric changes with the help of Adobe Photoshop CS6 Extended software. Calculated surface area measurements were used only for determining the amount of increase or decrease proportionately. For this purpose, the measurements have been realized in the consideration of that all MRI devices at Hacettepe University Department of Radiology didn’t undergo solubility change and that MRIs taken in external center were moved into the system with the same solubility ratio. All MRI scans assessed have section range of 4 mm and section thickness of 0.4 mm. Areal
measurement in mm2 with the method used previously by Waters P, et al. [13] was calculated in pixels in order to the volumetric change rate. In our study, calculated area data was firstly proportioned to each other and after taking the square root, it was cubed to carry volumetric meaning. Namely, mm2 values were converted to mm3 values. Areal measurements assessed in pixels are presented in Figure 3 as example.

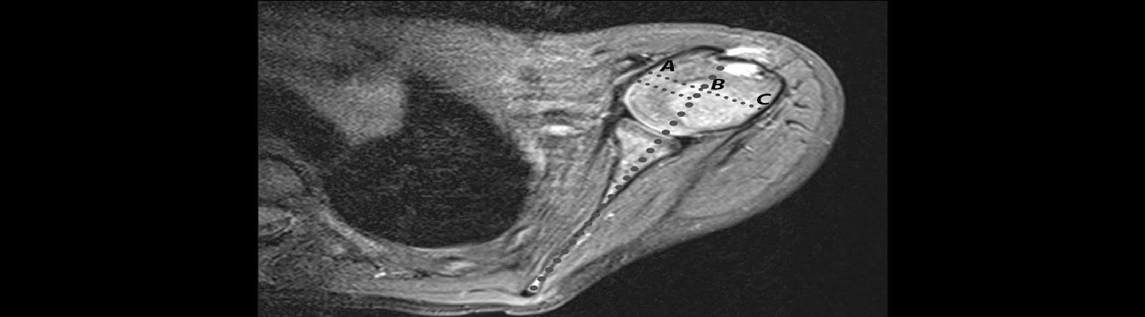
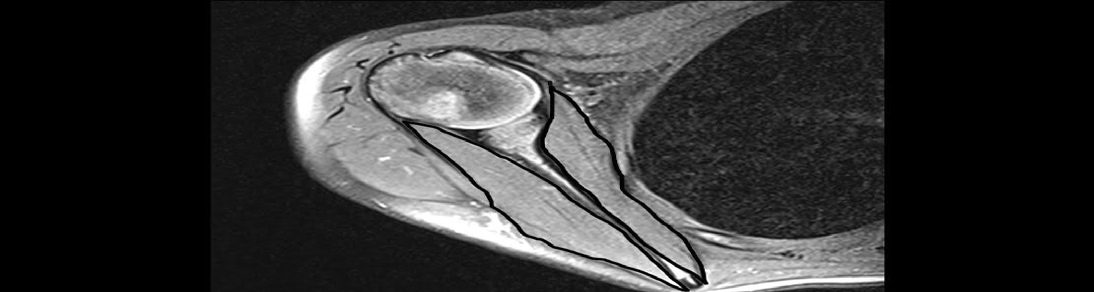
Figure 3: A) Preoperative period, 2-year-old-female patient B) Postoperative period, after 50 months follow-up. Areal measurements are made via T1 sequenced MR transverse sections in which subscapularis (SS) and external rotator muscle groups (infraspinatus and teres minor) (ER) appear in the widest extent. Correlating with the amount of pixels in areal measurement, Adobe Photoshop CS6 Extended program give the intervening area as the number of pixels by marking curvilinear marked lines as pixel. They have been included in comparative evaluation to gain volumetric meaning by being cubed of square roots of proportioning to each other. In the figure it is shown areal measurements for volume changes in muscle in preoperative and postoperative MRI scans of a patient with radiographic follow-up of 50 months.
Results
Osseous and muscular measurement values of shoulder side with palsy of preoperative period, shoulder side with palsy of postoperative period and healthy side of

postoperative period are respectively shown in Tables 2-4, The mean values of the measured parameters, mean values after the change and the statistical significance of the changes are presented in Tables 5 & 6.
| GV | PHHA | Elliptic Index (EI) | Subskapularis (SS) | External Rotator (ER) | |
|---|---|---|---|---|---|
| I | -19 | 0.25 | 1.236 | 12401 | 15038 |
| II | -48 | 0.229 | 1.492 | 17022 | 17578 |
| III | -65 | 0.065 | 1.544 | 8205 | 9529 |
| IV | -47 | 0.201 | 1.333 | 10174 | 18596 |
| V | -13 | 0.378 | 1.635 | 10111 | 18167 |
| VI | -47 | 0.315 | 1.724 | 9810 | 13689 |
| VII | -61 | 0.199 | 1.572 | 4318 | 7194 |
| VIII | -38 | -0.159 | 1.443 | 4587 | 11526 |
| IX | -33 | 0.253 | 1.589 | 7550 | 10322 |
| X | -18 | 0.359 | 1.265 | 7128 | 15855 |
| XI | -14 | 0.36 | 1.377 | 14241 | 20419 |
| XII | -53 | 0.152 | 1.576 | 2280 | 5767 |
| XIII | -39 | 0.24 | 1.481 | 7888 | 15110 |
| XIV | -14 | 0.336 | 1.46 | 16011 | 26848 |
| Mean value -36.4±18.1 | 0.227±0.142 | 1.481±0.141 | 9409±4363 | 1488±5619 |
Table 2: Osseous and muscular measurement values of shoulder side with palsy of preoperative period.
| Patient number | GV | PHHA | Elliptic Index (EI) | Subskapularis (SS) | External Rotator (ER) |
|---|---|---|---|---|---|
| I | -15 | 0,268 | 1.194 | 21007 | 31133 |
| II | -4 | 0,435 | 1.142 | 14106 | 10423 |
| III | -61 | 0,213 | 1.508 | 8196 | 11245 |
| IV | -6 | 0,433 | 1.342 | 13296 | 13180 |
| V | -9 | 0,191 | 1.075 | 11201 | 10703 |
| VI | 0 | 0,451 | 1.243 | 12216 | 14623 |
| VII | 0 | 0,473 | 1.279 | 7182 | 8928 |
| VIII | -6 | 0,373 | 1.515 | 16031 | 22747 |
| IX | -32 | 0,141 | 1.569 | 13601 | 12924 |
| X | -5 | 0,431 | 1.273 | 19922 | 17306 |
| XI | -2 | 0,456 | 1.35 | 18424 | 25412 |
| XII | -7 | 0,367 | 1.125 | 12521 | 23703 |
| XIII | -6 | 0,454 | 1.318 | 10255 | 12090 |
| XIV | -4 | 0,434 | 1.142 | 14292 | 18392 |
| Mean value | -10.813±15.372 | 0.378±0.110 | 1.299±0.146 | 13311.44±4003.42 | 16108.13 ±6435.23 |
| Patient number | GV | PHHA | Elliptic Index (EI) | Subskapularis (SS) | External Rotator (ER) |
| I | -5 | 0,442 | 1.111 | 37124 | 33431 |
| II | -5 | 0,424 | 1.145 | 27494 | 33876 |
| III | -10 | 0,482 | 1.487 | 10634 | 14706 |
| IV | 1 | 0,495 | 1.178 | 16105 | 18765 |
| V | -1 | 0,454 | 1.392 | 12500 | 16267 |
| VI | 1 | 0,451 | 1.278 | 16928 | 24086 |
| VII | -5 | 0,425 | 1.555 | 19658 | 22614 |
| VIII | -5 | 0,477 | 1.33 | 27350 | 31996 |
| IX | -4 | 0,469 | 1.451 | 27234 | 20541 |
| X | -6 | 0,448 | 1.287 | 26178 | 32954 |
| XI | -1 | 0,448 | 1.23 | 18938 | 22285 |
| XII | 0 | 0,470 | 1.359 | 22402 | 25713 |
| XIII | -5 | 0,498 | 1.295 | 19794 | 19542 |
| XIV | -6 | 0,510 | 1.488 | 15129 | 27772 |
| Mean value | -3.625±2.96 | 0.4670±0.27 | 1.352±0.14.ç5 | 20786.75±6827.26 | 23624.06±6644.76 |
Table 3: Osseous and muscular measurement values of shoulder side with palsy of postoperative period.
| Mean value | Difference | S value | P value | ||
|---|---|---|---|---|---|
| GV | Preoperative | -36,357 | +25,143 | 18,126 | 0.000* |
| GV | Postoperative | -11,214 | +25,143 | 16,427 | 0.000* |
| PHHA | Preoperative | 0,250 | +0,116 | 0,092 | 0.007* |
| PHHA | Postoperative | 0,366 | +0,116 | 0,113 | 0.007* |
| EI | Preoperative | 0,481 | -0,190 | 0,141 | |
| EI | Postoperative | 0,291 | -0,190 | 0,155 | 0.005* |
| SS | Preoperative | 98,19,03,164 | +67,64,01,230 | 64,38,68,438 | 0.014* |
| SS | Postoperative | 1,65,83,04,394 | +67,64,01,230 | 72,50,76,719 | 0.014* |
| ER | Preoperative | 1,87,11,34,085 | +39,19,08,088 | 1,04,40,08,390 | 0.667 |
| ER | Postoperative | 2,26,30,42,177 | +39,19,08,088 | 1,39,26,47,954 | 0.667 |
| Mean value | Difference | S value | P value | ||
| GV | Side with palsy postoperative | -11,214 | -7,571 | 16,428 | 0,104 |
| GV | Healthy side postoperative | -3,643 | -7,571 | 3,178 | 0,104 |
| PHHA | Side with palsy postoperative | 0,366 | -0,098 | 0,113 | 0,004* |
| PHHA | Healthy side postoperative | 0,464 | -0,098 | 0,026 | 0,004* |
| EI | Side with palsy postoperative | 0,292 | -0,036 | 0,291 | 0,482 |
| EI | Healthy side postoperative | 0,328 | -0,036 | 0,328 | 0,482 |
| SS | Side with palsy postoperative | 1658304 | -1560706 | 725076 | 0,004* |
| SS | Healthy side postoperative | 3219011 | -1560706 | 1629269 | 0,004* |
| ER | Side with palsy postoperative | 2263042 | -692266 | 1392647 | 0,004* |
| ER | Healthy side postoperative | 3955308 | -692266 | 1544393 | 0,004* |
Table 4: The mean values of the measured parameters of affected side shoulders, mean values after the change of postoperative fol
According to the results, It is understood that significant (p <0.05) changes in GV and EI values has occurred at the similar rate to values of the healthy shoulder side at the end of postoperative follow-up period (Tables 5 & 6).
Discussion
According to the study results, it has been found that significant osseous remodelling has occurred in accordance with early secondary shoulder surgical procedures performed on the cases with OBPP accompanied by shoulder problems and in accordance with the literature on long-term follow-up [3, 6, 13, 16]. This is particularly obtained in EI values and GV values assessed by Friedman method which express remodelling of the humeral head and glenoid [17].
According to these results, it has been obtained in follow- up that the humeral head is more oval and the glenoid is in more anteverted position. Even if significant reduction in the amount of GH subluxation had been obtained, this reduction could not be achieved in exactly similar amount with the healthy side. SS volumetric changes have been likewise determined in the direction of statistically significant increase; these values have lagged behind by not exactly matching with the current values of the healthy side. Any gain in ER changes couldn’t be mentioned. Namely, while a significant change in volumetric external rotator muscle group is not observed at the post-surgical follow-up, it can be said that subscapularis muscle volume increase has occurred but it has not been as healthy side.
Several previous studies have stated that shoulder side interventions on patients with OBPP are important in terms of prevention of posterior glenoid dysplasia and dislocation for joint integrity [7, 13, 16]. In this sense, we think that our study will make a significant contribution to the literature in terms of showing that remodelling has been achieved as both glenoid and humeral head origin. In addition, we believe on the occasion of our study that MR as stated in previous studies has an important place in assessment of shoulder problems of the patients with OBPP and of response to treatment.
Limiting the number of patients in order to ensure adequate follow-up in the study can be considered as a negative aspect of the study. However, we believe that this study is valuable because it allows multidimensional assessments and contains the long follow-up period. Also we think that our study will make a significant contribution to the literature because it represents comparatively the results of healthy side and side with palsy in postoperative period.
Consequently, it will be true to say that osseous remodelling in GHJ has been significantly achieved on the cases with OBPP through early secondary shoulder surgical procedures and that this achieved remodelling has been both glenoid and humeral head origin. However in case that the muscle volume change is viewed, it is a little difficult to talk about the same situation. Even though slight increase in the volume of the subscapularis muscle was recorded, it is obvious that this situation couldn’t achieve success in osseous remodelling.
References
-
Jellicoe P, Parsons JS (2008) Brachial plexus birth palsy. Current orthopaedics 22(4): 289-194.
-
Kozin SH, Boardman MJ, Chafetz RS, Williams GR, Hanlon A (2010) Arthroscopic treatment of internal rotation contracture and glenohumeral dysplasia in children with brachial plexus birth palsy. J Shoulder Elbow Surg 19(1): 102-110.
-
Kozin SH, Chafetz RS, Barus D, Filipone L (2006) Magnetic resonance imaging and clinical findings before and after tendon transfers about the shoulder in children with residual brachial plexus birth palsy J Shoulder Elbow Surg 15(5): 554-561.
-
Leblebicioğlu AG (2005) Brakiyal Pleksus Yaralanmaları. Türk Nöroşirürji Dergisi 15(3): 227-249.
-
Moukoko D, Ezaki M, Wilkes D, Carter P (2004) Posterior shoulder dislocation in infants with neonatal brachial plexus palsy. J Bone Joint Surg 86(4): 787-793.
-
Pearl ML (2003) Arthroscopic release of shoulder contracture secondary to birth palsy: An early report on findings and surgical technique. Arthroscopy 19(6): 577-582.
-
Pearl ML, Edgerton BW, Kazimiroff PA, Burchette RJ, Wong K (2006) Arthroscopic release and latissimus dorsi transfer for shoulder internal rotation contractures and glenohumeral deformity secondary to brachial plexus birth palsy. J Bone Joint Surg 88(3): 564-574.
-
Van der Sluijs JA, Van der Meij M, Verbeke J, Manoliu RA, Wuisman PI (2003) Measuring secondary deformities of the shoulder in children with obstetric brachial plexus lesion: reliability of three methods. J Pediatr Orthop 12(3): 211-214.
-
Waters PM (1997) Obstetric brachial plexus injuries: evaluation and management. J Am Acad Orthop Surg 5: 205-214.
-
Hoffer MM, Phipps GJ (1998) Closed reduction and tendon transfer for treatment of dislocation of the glenohumeral joint secondary to brachial plexus birth palsy. J Bone Joint Surg 80(7): 997-1001.
-
Hogendoorn S, Van Overvest KL, Watt I, Duijsens AH, Nelissen RG (2010) Structural changes in muscle and glenohumeral joint deformity in neonatal brachial plexus palsy. J Bone Joint Surg Am 92(4): 935-942.
-
Waters PM, Bae DS (2006) The effect derotational humeral osteotomy on global shoulder function in brachial plexus birth palsy. J Bone J Surg Am 88(5): 1035-1042.
-
Waters PM, Monica JT, Earp BE, Zurakowski D, Bae DS (2009) Correlation of radiographic muscle cross- sectional area with glenohumeral deformity in children with brachial plexus birth palsy. J Bone Joint Surg 91(10): 2367-2375.
-
Yücetürk A (2001) Palliative surgery: tendon transfers to the shoulder in children. Edited by Gilbert A. Martin Dunitz Ltd. London 25: 249-259.
-
Hoeksma AF, Ter Steeg AM, Dijkstra P, Nelissen RGH, Beelen A, et al. (2003) Shoulder contracture and osseous deformity in obstetrical brachial plexus injuries. J Bone Joint Surg Am 85(2): 316-322.
-
Hui JH, Torode IP (2003) Changing glenoid version after open reduction of shoulders in children with obstetric brachial plexus palsy. J Pediatr Orthop 23(1): 109-113.
-
Friedman RJ, Hawthorne KB, Genez BM (1992) The use of computerized tomography in the measurement of glenoid version. J Bone Joint Surg Am 74(7): 1032-1037.
- Electrolyte Considerations for Athletes
- Comprehensive Rehabilitation in Adults with Diabetic Peripheral Neuropathy: A Literature Review on Frequency, Intensity, and Duration Parameters
- Exercise Duration and Its Association with ADHD Symptom Severity in Children and Adolescents: A Parent-Reported Survey Study
- Adaptation of the Adult Neurophysiology of Pain Questionnaire for Use in Pediatrics
- A Non-Pharmacological Multidisciplinary Pain Program within a Hospital Wellness Program: A Mixed Methods Study
- The Effect of Frenkel's Exercise with PNF on Functional Reach in Stroke Survivors: A Randomized Control Trial