Post-Operative Patient Preference of Knee in Cruciate Retaining Vs Posterior Stabilized in Bilateral Total Knee Arthroplasty - A Long Term Prospective Follow Up Study
Patient satisfaction after Total Knee Arthroplasty (TKA) is a matter of concern. There is multitude of patient, surgery and implant factors associated to it. Implant design is one of the important factors. Here, we try to assess the correlation between the implant design [Cruciate Retaining (CR) or Posterior Stabilising (PS)] and the patient’s preference of satisfaction in patients undergoing Bilateral Total Knee Arthroplasty for equally affected arthritic knees. 34 patients (68 knees) were followed up for a period of 2 years and Knee Society Knee Scoring (KSKS), preference data were recorded and statistically assessed. Correlation between implant designs were also looked into. At 6 weeks, 3 months, 6 months, 1 year and 2 years follow up, there is significant association of side preference to the side which was operated first irrespective of the implant design. There was no association between the implant design (CR, PS) to the side preference. Patient showed a strong association of pain scoring to side preference. We would like to follow up this finding with more number of samples.
Introduction
Total Knee Arthroplasty (TKA) is one of the most successful surgeries of the decade. The evaluation of the success of the surgery has seen evolution of many implant designs. Most routinely done designs are CR (Cruciate Retaining) and CS (Cruciate Sacrificing) designs. In CR designs, PCL is left institution and in CS designs both ACL and PCL are removed. There have been many studies comparing the functional advantages and disadvantages of both of them [1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15]. Many of them concluded with better functional outcomes with CS designs than the CR designs (1) whereas many have outlined that there was no significant differences between both the designs in functional outcome [2, 16]. Although the discussion of the designs of TKA and retention of PCL has been the subject of argument for decades, the superiority of CR designs over the PS designs has never been established. In many of the studies done earlier for comparing CR VS PS designs, hemilateral TKA was done first and few months later or more ipsilateral TKA was done, where pre operative functional status, post operative pain management, type of anaesthesia and analgesia for rehabilitation were different.
A prospective randomized study of CR Vs CS designs in simultaneous same sitting bilateral TKA which would minimize the patient factors and pain management protocol and rehabilitation would be of higher value to determine whether the CR designs or the PS designs is superior. No clear benefits or drawbacks are apparent for either type of implant designs to the extent that either of them is clearly superior [4]. PS designs have been suggested to offer easier correction of deformity without concern for obtaining appropriate tension on the PCL, a more conforming polyethylene surface that results in polyethylene wear and a more reliable roll back of femur on tibia in flexion [5]. Proponents of PS designs note the more widespread clinical usefulness in that in can be used in knees without PCL [6], as well as the potential benefit of avoiding late posterior instability from PCL rupture which has been reported in osteoarthritic patients and in those with inflammatory arthritis [8, 9].
Proponents of CR [10, 11, 12, 13, 14] have suggested advantages including preservation of an important central stabilizing structure, transfer of stress to a functional ligament rather than a mechanical structure with subsequent reduction in wear and fixation stress, more consistent preservation of the joint line [15], improvement in stair climbing ability [11], and greater conservation of bone. In addition, problems that appeared to be unique with PS designs like patellar clunk, and posterior breakage and wear are absent in CR designs. Finally, the concept of simply resurfacing the joint and maintaining as much as normal structure as possible is the philosophically appealing one. Multiple studies have noted no difference between the two in ultimate range of motion and knee outcome ratings.
In this study, we look into those patients who underwent bilateral TKA-either single sitting or sequential staged one week apart with either of the designs with same type of anesthesia, post operative pain management and physiotherapy protocol. Study was done regarding the patient preference based on pain and functional outcome.
Aims and Objectives
To assess the factors contributing to the patient’s preferences in patients who underwent bilateral total knee arthroplasty either staged or single sitting. To evaluate pain and functional outcome of these patients till a period of 2 years of post operative follow up.
Inclusion Criteria
Patients with bilateral OA / RA knee with similar Kellgren Lawrence class and pre-operative functional status that underwent bilateral TKA-either staged one week apart or simultaneous in our institution from 2011 May to 2012 September. Those who gave the valid informed consent signed.
Exclusion Criteria
Revision TKA patients and patients who underwent bilateral TKA staged more than one week apart were also excluded. Patient who had any bony deficits in femur or tibia who required any augmentation procedures, who had associated problems of the spine with neurological deficits or any complications which required compromise in the hospital post TKR physiotherapy protocol and those with coronal plane deformities more than 20 degrees. Those patients with any arthritic symptoms in ipsilateral hip or ankle joints which we felt could alter the post operative observation of the study were excluded.
Materials and Methods
34 patients who underwent bilateral TKA-either staged one week apart or simultaneous in our institution was followed up till a period of two years. Follow up pain and functional assessment and their side preference was documented at 6 weeks, 3 months, 6 months, 1 year and 2 years. The entire data is analyzed to assess the factors which contributed to the preference. It’s statistical significance was tested. All the patients were informed of the study, its nature and the purpose. Institute Review Board clearance has been obtained for the study. We used implants from different companies for the patients, but any patient received either CR or PS designs of the same company. In bilateral TKA, all patients underwent TKA with an extramedullary instrumentation for tibial cut and intramedullary instrumentation for femoral cut on one side and the other side with navigation assisted system which was randomized. Ligament balancing in flexion and extension were achieved depending on any medial or lateral side opening [17]. Release of the medial side was done by removal of tibial and femoral osteophytes, releasing the tibial attachment of MCL, releasing of posteromedial capsule and release of attachment of semi membranosus tendon at posteromedial corner. Post operative management was followed uniformly for all patients. All the patients received post operative analgesia either by an epidural catheter or a femoral block and isometric quadriceps exercises, ankle pumps and toe movements were started as soon as the patient could do it actively. Range of movement exercises were begun and full weight bearing with walker was initiated the next day. DVT prophylaxis was initiated for all the patients.
Statistical Analysis
Considering the previous studies and the results, it is statistically acceptable to conduct the study with a sample size of 34 patients and 68 knees. Statistical Analysis will be performed by standard tests – Chi square test; Fischer exact test to assess the association between the variables. Data will be expressed in proportions.
Results
34 patients (68 knees) who underwent bilateral total knee replacement in our Institution, during a time period of 1 year, were followed up for a period of 2 years. At each and every visit, preference of knee was noted as well as Knee Society Knee Scoring. The score and the side preference were compared and statistically analyzed (Figure 1).
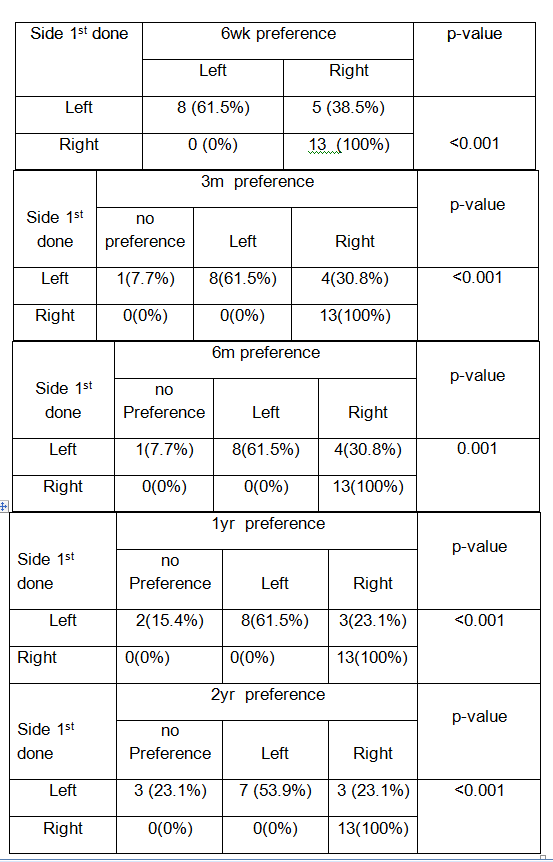
From the chart, on follow up at 6 wks, it is clear that the patients in whom staged bilateral TKA was done preferred the side which was done first; irrespective of the design of the implant. But 5 patients out of 13 patients (38.5%) in whom left side was done first preferred right side. The correlation appears to be statistically significant.
At 3 months follow up, 4 patients in whom left side was done first preferred right side. One patient had no preference and all the right side first patients preferred right side itself.
The correlation appears to be statistically significant (Tables 1-14).
At 6 months follow up, the statistics showed the same trend as at 3 months follow up.
At 1 year follow up, 2 patients in whom left side was done first turned to have no preference to the side and 3 of them preferred right side. All the patients in whom right side was done preferred right side itself.
| Left Side | 6Wk | ||
|---|---|---|---|
| Left | Right | p-value | |
| CR | 3(42.9%) | 4(57.1%) | 0.266 |
| PS | 5(83.3%) | 1(16.7%) |
Table 1: Showing side preference to implant design at 1 year follow up.
- At 6 wks 13 patients who underwent Lt Side first 7 had
- CR and 6 had PS design 8 preferred Lt Side and 5 preferred
- Rt side showing no association between the side preference and implant design.
- Left Side
- 3m p-value
- No Pref
- Left
- Right
- CR
- 1(14.3%)
- 3(42.9%)
- 3(42.9%)
- 0.296
- PS
- 0(0%)
- 5(83.3%)
- 1(16.7%)
Table 2: Showing side preference to implant design at 3 months follow up.
- At 3 months one patient who preferred Rt side with
- CR design at 6 wks has changed to no preference but the remaining patients have shown the same findings indicating
- Left Side
- 6m p-value
- No Pref
- Left
- Right
- CR
- 1(14.3%)
- 3(42.9%)
- 3(42.9%)
- 0.296
- PS
- 0(0%)
- 5(83.3%)
- 1(16.7%)
Table 3: Showing side preference to implant design at 6 months follow up.
- This table also shows no association between the implant design and side preference as earlier.
- Left Side
- 1yr p-value
- No Pref
- Left
- Right
- CR
- 2(28.6%)
- 3(42.9%)
- 2(28.6%%)
- 0.25
- PS
- 0(0%)
- 5(83.3%)
- 1(16.7%)
Table 4: Showing side preference to implant design at 1 year follow up.
In this table one more patient have changed to No preference from Rt side preference with CR design, but still there is no statistical association between the side preference and implant design.
| Pain Score- Lt | Mean | n | Std. Deviation | p-value |
|---|---|---|---|---|
| Pre op | 52.26 | 34 | 17.681 | |
| 6 wks post op | 79.68 | 34 | 13.316 | <0.001 |
| 3m post op | 86.91 | 34 | 10.172 | <0.001 |
| 6m post op | 91.65 | 34 | 6.085 | 0.002 |
| 1 yr post op | 94.44 | 34 | 5.489 | <0.001 |
Table 5: Showing the pain score for Lt side done at 6wks, 3months, 6 months and 1 year.
This table tells us that there has been statistical improvement in the pain score after the procedure.
| pain Score- Rt | Mean | n | Std. Deviation | p-value |
|---|---|---|---|---|
| Pre op | 54.79 | 34 | 16.968 | |
| 6 wks post op | 81.21 | 34 | 12.133 | <0.001 |
| 3m post op | 87.38 | 34 | 9.257 | 0.002 |
| 6m post op | 91.74 | 34 | 5.119 | 0.003 |
| 1 yr post op | 94.65 | 34 | 5.039 | <0.001 |
Table 6: Showing the pain score for Rt side done at 6wks, 3months, 6 months and 1 year.
This table tells us that there has been statistical improvement in the pain score after the procedure.
| Function score - Lt | Mean | n | Std. Deviation | p-value |
|---|---|---|---|---|
| Pre op | 40.88 | 34 | 16.259 | |
| 6 wks post op | 48.97 | 34 | 22.455 | 0.001 |
| 3m post op | 71.47 | 34 | 15.449 | <0.001 |
| 6m post op | 84.56 | 34 | 12.635 | <0.001 |
| 1 yr post op | 92.35 | 34 | 11.026 | <0.001 |
Table 7: Showing the function score for Lt side done at 6wks, 3months, 6 months and 1 year.
This table tells us that there has been statistical improvement in the function score after the procedure.
| Function score - Rt | Mean | n | SD | p-value |
|---|---|---|---|---|
| Pre op | 40.88 | 34 | 16.26 | |
| 6 wks post op | 51.18 | 34 | 21.88 | 0.006 |
| 3m post op | 70.74 | 34 | 15.58 | <0.001 |
| 6m post op | 84.56 | 34 | 12.64 | <0.001 |
| 1 yr post op | 92.35 | 34 | 11.03 | <0.001 |
Table 8: Showing the function score for Rt side done at 6wks, 3months, 6 months and 1 year.
This table tells us that there has been statistical improvement in the function score after the procedure except for scoring at 6 wks.
| KSKS - Lt | Mean | N | Std. Deviation | p-value |
|---|---|---|---|---|
| Pre op | 10.12 | 34 | 3.073 | |
| 6 wks post op | 21.94 | 34 | 3.733 | <0.001 |
| 3m post op | 28.41 | 34 | 2.904 | <0.001 |
| 6m post op | 34.88 | 34 | 2.705 | <0.001 |
| 1 yr post op | 37.71 | 34 | 2.097 | <0.001 |
| KSKS - Rt | Mean | N | Std. Deviation | p-value |
| Pre op | 10.12 | 34 | 3.073 | |
| 6 wks post op | 21.94 | 34 | 3.733 | <0.001 |
| 3m post op | 28.41 | 34 | 2.904 | <0.001 |
| 6m post op | 34.88 | 34 | 2.705 | <0.001 |
| 1 yr post op | 37.71 | 34 | 2.097 | <0.001 |
Table 9: Showing the KSKS for Lt Side done at 6wks, 3months, 6 months and 1 year.
This table tells us that there has been statistical improvement in the KSKS after the procedure.
- This table tells us that there has been statistical improvement in the KSKS after the procedure.
- 6 wks post op
- Mean n
- Sd p-value pain score - Lt
- 83.92
- 12
- 7.17
- 0.174 pain score - Rt
- 82.33
- 12
- 7.33 function score - Lt
- 56.67
- 12
- 22.7
- 0.339 function score - Rt
- 53.33
- 12
- 23.48
- KSKS - Lt
- 22.67
- 12
- 4.12
- 1
- KSKS - Rt
- 22.67
- 12
- 4.12
- Left preferred pain score - Lt
- 77.36
- 22
- 15.36
- Right preferred pain score - Rt
- 80.59
- 22
- 14.21 function score - Lt
- 44.77
- 22
- 21.68
- 0.264 function score - Rt
- 50
- 22
- 21.44
- KSKS - Lt
- 21.55
- 22
- 3.54
- 1
- KSKS - Rt
- 21.55
- 22
- 3.54
Table 10: Showing relation between side preferences to Pain score, Function score and KSKS at 6 wks post up.
- Here there is no statistical association between these scorings and the side preference, except for Rt side preference at 6wks to the pain score.
- 3m post op
- Mean n
- SD p-value pain score - Lt
- 90.82
- 11
- 5.21
- 0.001 pain score - Rt
- 87.45
- 11
- 5.57 function score - Lt
- 72.73a
- 11
- 17.37
- 1 function score - Rt
- 72.73a
- 11
- 17.37
- KSKS - Lt
- 28.18a
- 11
- 2.75
- 1
- KSKS - Rt
- 28.18a
- 11
- 2.75
- Left preferred pain score - Lt
- 84.33
- 21
- 11.75
- <0.001 pain score - Rt
- 86.76
- 21
- 11.02 function score - Lt
- 69.52
- 21
- 14.74
- 0.424 function score - Rt
- 68.33
- 21
- 14.78
- KSKS - Lt
- 28.19a
- 21
- 2.96
- 1
- KSKS - Rt
- 28.19a
- 21
- 2.96
- Right preferred
- This table shows us that there is no association between the side preference to the scoring done except for Rt side preference at 6 wks to pain score on the Rt side.
- 6m post op
- Mean n
- SD p-value pain score - Lt
- 92.91
- 11
- 3.36
- 0.006 pain score - Rt
- 90.64
- 11
- 3.2 function score - Lt
- 84.09
- 11
- 13.19
- 1 function score - Rt
- 84.09
- 11
- 13.19
- KSKS - Lt
- 34.55
- 11
- 3.11
- 1
- KSKS - Rt
- 34.55
- 11
- 3.11
- Left preferred pain score - Lt
- 90.48
- 21
- 7.03
- 0.017 pain score - Rt
- 91.81
- 21
- 5.81 function score - Lt
- 83.81
- 21
- 12.74
- 1 function score - Rt
- 83.81
- 21
- 12.74
- KSKS - Lt
- 34.95
- 21
- 2.58
- 1
- KSKS - Rt
- 34.95
- 21
- 2.58
- Right preferred
Table 11: Showing the association between side preference to Pain score, Function score and KSKS.
- This table shows us that there is no association between the side preference to the scoring done at 6 months follow up.
- 1 yr post op
- Mean n
- SD p-value pain score - Lt
- 94.45
- 11
- 2.54
- 0.015 pain score - Rt
- 92.91
- 11
- 3.05 function score - Lt
- 90.91
- 11
- 11.36
- 1 function score - Rt
- 90.91
- 11
- 11.36
- KSKS - Lt
- 37.82
- 11
- 2.27
- 1
- KSKS - Rt
- 37.82
- 11
- 2.27
- Left preferred pain score - Lt
- 93.8
- 20
- 6.75
- 0.064 pain score - Rt
- 95
- 20
- 5.88 function score - Lt
- 92
- 20
- 11.52
- 1 function score - Rt
- 92
- 20
- 11.52
- KSKS - Lt
- 37.6
- 20
- 2.21
- 1
- KSKS - Rt
- 37.6
- 20
- 2.21
- Right preferred
Table 12: Showing the association between side preference to Pain score, Function score and KSKS.
This table shows us that there is no association between the side preference to the scoring done at 1 year follow up.
Conclusion
In this study, we could conclude that at 6 weeks, 3 months, 6 months, 1 year and 2 years follow up, there is significant association of side preference to the side which was operated first irrespective of the implant design, with a p value of < 0.001.
61.5 % of patients preferred left side when the left knee was operated first. 100% of patients preferred right side when the right knee was operated first. There was no association between the implant design (CR, PS) to the side preference. The p value was > 0.05 at 6 weeks, 3 months, 6 months and 1 year.
Patient showed a strong association of pain scoring to side preference except for scoring at 6 weeks follows up, where patients preferred the left side but there was no difference in pain score between the left and right sides.
There is no significant association between side preference to implant design in cases where we have done bilateral same sitting using either designs in knees in the same patient. In our observation, we found that patients preferred the side with CR designs, but as the sample size is too small, no association was found statistically significant. We would like to follow up this finding with more number of samples.
References
-
Michael J, Bercik (2013) Posterior cruciate retaining Vs posterior stabilized total knee arthroplasty – A met analysis; Journal of Arthroplasty (28): 439-444.
-
Lozano Calderon SA, Shen J Doumato, Greene DA, Zelicof SB (2013) Cruciate retaining Vs posterior substituting inserts in total knee arthroplasty: functional outcome comparison. Journal of arthroplasty 28(2): 234-242.
-
Kazuyoshi Yagishita (2012) High flex posterior cruciate retaining Vs posterior cruciate stabilizing designs in simultaneous bilateral TKA; Journal of arthroplasty 27(3): 368-374.
-
Insall and Scott Surgery of the Knee, 5th (Edn.), Chapter 109, pp: 1125-1131.
-
Scott RD (1993) 12 years’ experience with Posterior cruciate retaining TKA; CORR (205): 100-107.
-
Ginsel BL, Banks S, Verdonschot N (2009) Improving maximum flexion with posterior cruciate retaining TKA, A fluoroscopic study; Acta Ortho Belgium 75(6): 801- 807.
-
O’ Rourke MR, Claghan JJ (2002) Osteolysis associated with cemented modular posterior cruciate substituting total knee design; 5-8 year follow up. JBJS Am (84): 1362-1371.
-
Komislek RD, Mahfouz MK, Bertin KC (2008) In vivo determination of TKA kinematics, the Nexgen Prosthesis with and without a PCL – A multicentre analysis. Journal of Arthroplasty 23(1): 41-50.
-
Mestha P, Shenava Y (2000) Fracture of polyethylene tibial post in Posterior stabilized (IB 2) TKA; Journal of Arthroplasty 15: 814-815.
-
Andriachi TP, Gulante JO (1988) Retention of PCL in TKA. Journal of Arthroplasty 3: S13-S19.
-
Andriachi TP, Gulante JO, Fermier RW (1982) The influence of total knee replacements designs in walking and stair climbing, JBJS Am Vol: 64(9): 1328-1335.
-
Barrington JW, Sah A, Malchan H (2009) Contemporary Cruciate Retaining TKA with a pegged tibial base plate, Results at a minimum of 10 years; JBJS AM 91: 874-878.
-
Bozic KJ, Kinder J, Menegini M (2005) Implant survivorship and complication rates after Total Knee Arthroplasty with a 3rd generation cemented system 5-8 years follow up. CORR 430: 117-124.
-
Dorr LD, Oschner JL (1998) Functional Comparison of Posterior cruciate Vs Cruciate sacrificied TKA. CORR 236: 34-36.
-
Emodi GJ, Callaghan JJ, Pedersen DR (1999) Posterior cruciate ligament function following TKA. The effect of joint line elevation. IOWA Orthop journal 19: 82-92.
-
Kim YH, Choi Y, Kwon OR, Kim JS (2009) Functional outcome and range of motion of high flexion posterior cruciate retaining and high flexion posterior substituting total knee prosthesis-A prospective randomized study. JBJS Am 91(4): 753-760.
-
Yagishita K, Muneta (2003) Step by step measurements of soft tissue balancing during total knee arthroplasty for patients with varus knee. Journal of arthroplasty 18: 313.
- Electrolyte Considerations for Athletes
- Comprehensive Rehabilitation in Adults with Diabetic Peripheral Neuropathy: A Literature Review on Frequency, Intensity, and Duration Parameters
- Exercise Duration and Its Association with ADHD Symptom Severity in Children and Adolescents: A Parent-Reported Survey Study
- Adaptation of the Adult Neurophysiology of Pain Questionnaire for Use in Pediatrics
- A Non-Pharmacological Multidisciplinary Pain Program within a Hospital Wellness Program: A Mixed Methods Study
- The Effect of Frenkel's Exercise with PNF on Functional Reach in Stroke Survivors: A Randomized Control Trial