Patellofemoral Pain Syndrome: Characteristics and Outcomes of Physical Therapy Episodes of Care
Background: Patellofemoral pain syndrome (PFPS) is a common musculoskeletal condition. Understanding episode of care variables can lead to improved outcomes. Objectives: To explore outcomes of physical therapy (PT) for the management of patients with PFPS. Design: Retrospective cohort. Methods: Data was extracted from the electronic medical record for patients with PFPS treated at a single, academic PT site between July 1, 2016 and May 30, 2019. Episode of care variables, relationship between variables, and odds of improvement were assessed. Results: Fifty-two patients with PFPS, mean (± SD) age of 25.9 (± 14.1) years were referred to PT. Over the course of a single episode of care, significant improvements were seen in pain (P = 0.03) and knee extension strength (P <0.001) with 20-21 complete data sets respectively. After adjusting for age, there was a 13.8% increase in the odds of making clinically meaningful improvements in pain though these findings did not reach statistical significance (Odds ratio [OR] 1.14, 95% CI 0.93-1.39). Positive relationships were identified between weeks (r = 0.57; P = 0.008) and number of visits (r = 0.57; P = 0.007) with improved knee extension strength. Age was negatively correlated with improvements in knee extension strength (r = -0.46; P = 0.04). Conclusion: Each additional visit for patients with PFPS, up to 9 visits, and a younger age are associated with greater odds of making clinically significant improvements in pain. Greater number of weeks and PT visits and a younger age yield higher improvements in knee extension strength.
Introduction
Patellofemoral Pain Syndrome (PFPS) occurs across the lifespan, accounting for 1.5% to 7.3% of all individuals seeking medical care in the United States [1]. PFPS is diagnosed in over 400,000 individuals annually and is a collection of predominately non-traumatic conditions that present as anterior retropatellar or peripatellar knee pain [1, 2]. These symptoms are experienced by approximately 23% of the general population and are most prevalent among adolescent, female athletes [2]. PFPS symptoms are often increased with lower-limb loading including squatting, prolonged sitting, stair negotiation, jumping, and/or running [3, 4]. Therefore, individuals with PFPS experience substantial limitations in activities of daily life, work, and sports [1]. A systematic review on this topic noted that reproduction of retropatellar pain during squatting and a hypomobile patellar tilt test were the most accurate diagnostic tests for PFPS [4]. Symptoms associated with PFPS have the potential to become chronic and more than half of individuals with PFPS report unfavorable recovery 5 to 8 years after symptom onset even without radiographic evidence of osteoarthritis [5]. Despite the prevalence and challenges for recovery in patients with PFPS, physical therapy (PT) interventions demonstrate potential to improve symptoms and function in individuals with PFPS [6, 7, 8]. Randomized controlled trials using targeted hip and knee exercises have demonstrated improvements in pain and patient-reported function; however, reports show no consistency on frequency and duration of exercise making it difficult to prescribe the optimal plan of care [9, 10, 11, 12]. Accordingly, the Academy of Orthopaedic Physical Therapy of the American Physical Therapy Association has published clinical practice guidelines (CPG) for patellofemoral pain to guide evidence-based PT practice and management for patients experiencing PFPS [13]. The CPGs recommend hip and knee targeted exercises and a combined intervention approach including exercise therapy along with foot orthoses, patellar taping, patellar mobilizations, and lower-limb stretching [13]. However, optimal frequency of PT care and total number of PT visits remains unclear. A living systematic review with network meta-analysis found that education in combination with a physical treatment (exercise, orthoses or patellar taping/mobilization) is most effective at 3 months [14]. The study could not recommend a specific type or class or physical treatment over another due to insufficient evidence [14]. Currently, there is no accepted standard program of rehabilitative management [13, 15, 16]. Determining the frequency and duration of care for patients with PFPS can help to standardize effective treatment, inform clinical practice guidelines, improve patient and family engagement, and decrease variance in clinical trials [16, 17]. The purpose of this study was to explore characteristics and outcomes of PT episodes of care for the management of patients with PFPS including analysis of referral timing, frequency and duration, changes in pain, range of motion (ROM), strength, and patient-reported functional outcomes in a single, academic clinic setting.
Methods
Procedures
A retrospective electronic medical records review was performed identifying patients with PFPS who were treated at a single academic physical therapy location. Data from the medical records were manually extracted including age, diagnosis, referral timing, frequency, duration, number of PT visits, and outcome measures. This study was approved by University of Maryland, Baltimore’s Institutional Review Board. This study did not require any interaction with the research subjects and all information was deidentified for extraction and analysis to maintain confidentiality. Each rehabilitation examination included objective and subjective measures of pain, ROM, strength, and patient-reported functional outcomes. Pain was measured using a 10-cm Visual Analogue Scale (VAS) where 0 represents “no pain” and 10 represents “the worst pain”. The VAS is reliable and valid in assessing treatment outcomes in persons with PFPS [18]. The minimal clinically important difference (MCID) is important to consider as it provides clinicians the necessary information to determine if a meaningful change has been made to the patient [18]. It has been reported that the MCID for the VAS in those experiencing PFPS is a change of 1.5 to 2.0 cm (15%–20%) to detect improvement [18].
ROM is a measure, in degrees, of the arc of motion a joint has in a space, which is routinely measured with a goniometer [19]. Strength, as defined by Dutton [20], as an assessment of power where musculotendinous units act across a bone-joint lever-arm system to actively generate motion or passively resist movement against gravity and resistance, was measured with manual muscle testing (MMT) [20, 21]. In the clinical setting, MMT was commonly used to assess strength [20, 21]. Patient-reported functional outcomes were used to assess a patient’s current level of function and quality of life. The Lower Extremity Functional Scale (LEFS) questionnaire was used to minimize bias, maintain validity, document progress, and help to determine and advance treatment approaches [22]. The LEFS is a reliable and validated questionnaire that measures functional limitations in individuals with lower extremity dysfunctions such as PFPS [23, 24]. The LEFS has been found to be reliable and responsive to clinical change in individuals with anterior knee pain [24].
International Classification of Diseases, Tenth Revision (ICD-10) codes (Table 1) were assessed in EPIC (Epic Systems Co., Verona, WI) to identify electronic medical records of patients seen between July 1, 2016 and May 30, 2019 for physical therapy services. Episodes of care were included if the patient had a diagnosis of PFPS and were 6 years of age or older at the time of rendered services. Episodes of care were excluded for patients with known active osteoarthritis or chondromalacia in the rehabilitating knee, or if the physical therapy episodes of care were not addressing the PFPS diagnosis. Baseline data were extracted from documentation of the initial evaluation or the subsequent PT encounter, and end-of-episode data were extracted from the final PT encounter. If no objective data were documented in the final PT encounter, data were extracted from documentation within three encounters, but no more than 30 days, from the final PT encounter.
| M22.2x9 | Patellofemoral Disorders, Unspecified Knee |
| M22.2x1 | Patellofemoral Disorders, Right Knee |
| M22.2x2 | Patellofemoral Disorders, Left Knee |
| M22.40 | Chondromalacia Patella, Unspecified Knee |
| S83.006A | Unspecified Dislocation of Unspecified Patella, Initial Encounter |
| M25.569 | Pain in Unspecified Knee |
| M25.561 | Pain in Right Knee |
| M25.562 | Pain in Left Knee |
Table 1: ICD-10 Codes Abbreviation: ICD-10, International Classification of Diseases, 10th Revision
Data Analysis
Statistical analysis was performed using SPSS version 22.0 (IBM Inc., Chicago, IL, USA) to calculate descriptive statistics including mean, standard deviation (SD), median, range, and percentages. MMT scores were converted to a 0–10 scale for analysis [25]. Pearson’s product correlations (r) were used to explore relationships between variables. Paired t-tests were used to assess changes from baseline to end-of- episode outcomes. All comparisons were made at the ≤0.05 level of significance. We used logistic regression to calculate log-odds of making a clinically significant improvement in pain intensity, using visit count as the primary predictor of interest. We exponentiated the log-odds to get an odds ratio, interpreted as the relative difference in likelihood of improvement for each additional visit of PT received.
Results
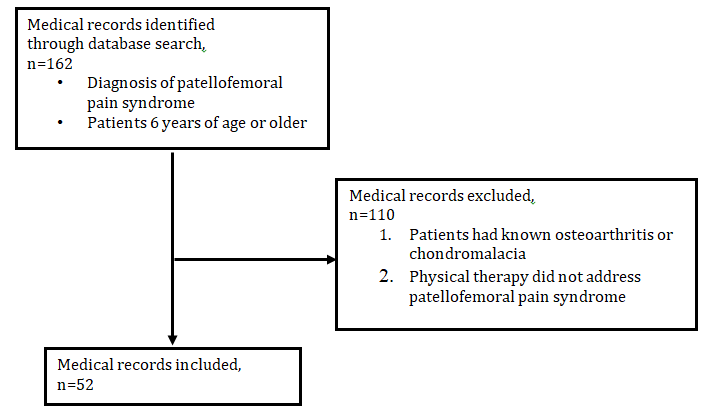
A total of 162 electronic medical records were screened. Of the initial search, 110 electronic medical records were excluded because these records did not meet the inclusion criteria. The remaining 52 electronic medical records underwent data extraction and analysis (Figure 1). The mean (± SD) age of the cohort was 25.9 (± 14.1) years at the time of the initial examination. The median time of referral to PT from the onset of symptoms was 34 weeks (interquartile range [IQR], 6.5–97.5). Frequency of PT was prescribed for 2 to 3 times per week for 71% of episodes of care; however, 71% of the patients attended PT 1 to 2 times per week. Episode of care duration was a median of 3.5 weeks (IQR, 1–9). The number of visits was a median of 3 visits (IQR, 1–7) (Figure 1, Table 2).
| Mean (SD) | Range | |
|---|---|---|
| Age, years | 25.85 (14.14) | 7-55 |
| Episode of Care (n = 52) | Median | IQR |
| Visits, count | 3 | 1-7 |
| Week, count | 3.5 | 1-9 |
| Initiation of Care Since Diagnosis, weeks (n = 42) | 34 | 6.5-97.5 |
Table 2: Episode of Care Characteristics. Abbreviations: SD, standard deviation; IQR, interquartile range Due to missing data for
Table 2: Episode of Care Characteristics. Abbreviations: SD, standard deviation; IQR, interquartile range Due to missing data for the majority of the participants on either the initial evaluation or the end of episode of care documentation, 20-22 complete data sets were able to be analyzed for pain, knee extension and flexion ROM, and knee extension strength and 11 complete data sets for the LEFS functional outcome. Over the course of a single episode of care, patients demonstrated significant improvements in pain (n = 20; P = 0.03), knee extension ROM (n = 21; P = 0.05), knee flexion ROM (n = 22; P = 0.001), and knee extension strength (n = 21; P <0.001). Patient reported functional outcomes were reported in 85% of episodes of care on initial visit, and the LEFS was used for all patients who completed a functional outcome questionnaire. Improvements were found in LEFS scores; however, these scores were not statistically significant (n = 11; P = 0.38). Mean change in variables over the course of care are presented in Table 3.
| Mean Change (SD) | Mean Range | |
|---|---|---|
| MMT Flexion (0–10) | 0.48 (1.21) | 8.27 to 9.10 |
| MMT Extension (0–10) | 0.95 (0.86) | 8.27 to 9.24 |
| ROM Flexion (degrees) | 6.73 (8.60) | 9.24 to 124.09 |
| ROM Extension (degrees) | 1.71 (3.74) | -0.20 to 1.43 |
| Functional Change on LEFS (0–80) | 8.27 (29.86) | 46.83 to 48.17 |
| Pain Change (0–10 VAS) | -1.70 (3.11) | 5.67 to 2.90 |
Table 4: Mean Change in Variables Over Course of Care Abbreviations: SD, standard deviation; MMT, manual muscle test; ROM, range
Table 3: Mean Change in Variables Over Course of Care Abbreviations: SD, standard deviation; MMT, manual muscle test; ROM, range of motion; LEFS, Lower Extremity Functional Scale; VAS, Visual Analogue Scale Each additional visit of physical therapy for patients with PFPS, up to 9 visits, is associated with a 12.1% increase in the odds of making clinically significant improvements in pain intensity over the course of therapy, but this difference was not statistically significant (Odds ratio [OR] 1.12, 95% CI 0.94-1.34). After adjusting for age, each additional visit was associated with a 13.8% increase in the odds of making clinically significant improvements in pain intensity over the course of therapy, but this difference was not statistically significant (Odds ratio [OR] 1.14, 95% CI 0.93-1.39).
Relationships between variables were explored, and moderate positive relationships were identified between the weeks (r = 0.57; P = 0.008) and number of visits (r = 0.57; P = 0.007) with improved knee extension strength. Age demonstrated a moderate negative relationship with improvements in knee extension strength (r = -0.46; P = 0.04), thus favouring increased magnitude of strength improvements among younger patients in this cohort (Table 4).
| R | P | |
|---|---|---|
| Weeks | 0.57 | 0.008** |
| Number of Visits | 0.57 | 0.007** |
| Age | -0.46 | 0.038* |
Table 3: Association Between Knee Extension Strength And Frequency And Duration And Age Variables r = Pearson’s product correlati
Table 4: Association Between Knee Extension Strength And Frequency And Duration And Age Variables r = Pearson’s product correlations; * = P<0.05; ** = P<0.01 Relationships between body function impairments and patient reported functional outcome scores were also explored. A significant negative relationship existed between the amount of improvement in pain and LEFS scores (r = 0.82; P = 0.01).
Discussion
This study explored the characteristics, outcomes, and relationships of PT episodes of care variables for the management of patients with PFPS. Over the course of a single episode of care, improvements were identified in pain, knee extension ROM, knee flexion ROM, and knee extension strength. Positive relationships were identified between the number of weeks and visits a patient received PT and the improvements in knee extension strength. Age- related relationships demonstrated increased improvement among younger patients. A significant relationship between improvement in pain and higher LEFS scores was also observed. Each additional visit of PT for patients with PFPS, up to 9 visits, and younger age are associated with an increase in the odds of making a clinically significant improvement in pain intensity over the course of PT. These findings support the greater use of PT, up to 9 visits for decreasing pain in younger patients with PFPS.
Understanding the frequency and duration of PT care for patients with PFPS can help to standardize effective treatment. Winters, et al. [14] found that education in combination with a physical treatment (exercise, orthoses or patellar taping/mobilization) is most effective at 3 months. The researchers performed a living systematic review with network meta-analysis to determine which treatment(s)/treatment category is most effective for PFPS. Twenty-two randomized controlled trials evaluating any treatment for individuals having PFPS for more than 6 weeks were included. Any improvement defined by any degree of recovery or improvement on a Global Rating of Change (GROC) Scale and pain intensity on scale of 0 to 10 or 0 to 100 by ‘worst in the past week’ on a VAS or Numerical Rating Pain Scale (NRS) were used as outcome measures. Education alone was comparable to education combined with a physical treatment at 12 months [14]. The study could not recommend a specific type or class or physical treatment over another due to insufficient evidence [14]. They found that all treatments were superior to a wait and see approach for any improvement on the GROC scale at 3 months [14]. However, no treatment was found superior to wait and see approach for the secondary outcome of pain intensity during the previous week [14]. This study supports that early patient education and potentially exercise and patellar taping/mobilizations may be of benefit in the first 3 months of symptom onset. The current study reported a median time of referral to PT from the onset of symptoms at 34 weeks (interquartile range [IQR], 6.5–97.5) or 7.8 months, which is significantly longer from what is recommended in the Winters, et al. [14] study. Reasons for delayed referral to PT in this study are unknown and would benefit from further exploration in future studies.
Specific exercise prescription related to improved outcomes of pain and function is yet to be determined in patients with PFPS [13, 16]. In the current study, patients were seen for a median of 3 visits (IQR, 1–7) over 3.5 weeks (IQR, 1–9) which is lower than previously published efficacious intervention trials that vary from 4 to 8 weeks [9, 10, 11, 12]. Young, Rhon, Cleland, and Snodgrass [16] performed a systematic review to identify specific doses of exercise related to improved outcomes of pain and function in individuals with knee osteoarthritis, patellar tendinopathy, and PFPS. A variety of outcome measures were used across the studies included. They reported 24 total therapeutic exercise sessions and 8 to 12-week durations of exercise therapy were most associated with large effect sizes for patients with knee osteoarthritis. The authors concluded that no trends were seen with exercise dosing for individuals with patellar tendinopathy or PFPS [16]. The most common intervention duration for PFPS was 8 weeks ranging from 3 to 16 weeks [16]. Dolak, et al. [9] randomized 33 females with PFPS into either initial hip strengthening or initial quadriceps strengthening for 4 weeks, before a 4-week program of functional weight-bearing exercises. This study used the VAS and LEFS, the same patient-reported outcome measures used in the present study, following exercise therapy 3 days a week for 8 weeks for a total of 24 visits to assess patient improvement [9]. The authors revealed that the hip group had significantly less pain than the quadriceps group at week
4. Pain scores at 4 and 8 weeks were significantly lower than baseline scores in the hip group. However, in the quadriceps group, pain scores were significantly lower than baseline at 8 weeks but not at 4 weeks. Both groups demonstrated a statistically significant mean decrease in VAS scores with a mean change ranging from 1.6 cm – 2.2cm. The current study found the mean change in pain to be 1.7 cm which is comparable to what Dolak, et al. [9] reported.
The MCID is important to consider as it provides clinicians the necessary information to determine if a meaningful change has been made to the patient [18]. It has been reported that the MCID for the VAS in those experiencing PFPS is a change of 1.5 to 2.0 cm (15%–20%) to detect improvement [9, 18]. A mean change of 1.7 cm on the VAS does reach the MCID of 1.5 to 2.0 which means a meaningful change has been made to the patient. The current study found that with each additional visit of physical therapy for patients with PFPS, up to 9 visits, there is a 12.1% increase in the odds of making clinically significant improvements in pain intensity of the course of therapy. Even though these findings are not statistically significant (Odds ratio [OR] 1.12, 95% CI 0.94-1.34), a 12.1% increase in the odds of making clinically significant improvement in pain is compelling and supports the greater use of therapy, up to 9 visits.
Dolak, et al. [9] reported a mean improvement of 12 points on the LEFS following 8 weeks of rehabilitation, whereas the current study results showed a mean improvement of 8.3 points over a median of 3.5 weeks. This comparison supports the findings of the current study that a higher number of visits over a longer duration yields greater improvement on the LEFS. It is important for clinicians to consider the minimal detectable change (MDC) which conveys the number of points a questionnaire must change to be confident that a true change in the patient’s functional status has occurred [24, 26]. A MDC of 8 points has been reported in patients experiencing anterior knee pain, the most common symptom of PFPS [24]. Despite that improvements in LEFS scores in the present study were not statistically significant (n = 12; P = 0.38), the patients in this study did demonstrate improvements greater than the previously reported MDC. Future longitudinal studies are needed to further investigate the relationships between body function impairments such as strength and functional outcomes in patients with PFPS.
Despite the most commonly prescribed frequency of 2 to 3 times per week for 71% of the patients, the patients in this single academic site study attended fewer number of visits (median of 3 visits) over a shorter period of time (median of 3.5 weeks). Most episodes of care ended because of a combination of self-discharge and insurance issues (85.6%). The exact reason for patients' self-discharge from PT care and cause of insurance issues is unknown. However, it is important to note that all patients included in the current study were seen in an urban single academic clinical setting.
No-show rates have been shown to range from 15% to 30% in adult general medicine clinics and urban community centers [27, 28, 29]. Ofei-dodoo, et al. [29] interviewed 25 patients over the phone at two urban, university affiliated family medicine residency outpatient clinics who missed three or more scheduled appointments during a 5-year span. The authors found five consistent themes for why these patients missed their scheduled outpatient appointments: forgetfulness; transportation issues; personal health issues; family and employer obligations; and other issues, such as anticipated long clinic wait times, bad weather, and financial problems. The reasons for patients in the current study no longer attending PT is unknown but warrants further exploration in future studies.
Knee extension strength has been identified as a target for PT intervention [13]. The results of the current study suggest that patients who had a higher number of visits and who were treated for a longer duration in weeks, demonstrated greater improvements in knee extension strength. Van Tiggelen, et al. [30] identified decreased knee extension strength as a predisposing factor in the development of PFPS in male military recruits. In a case-control study comparing asymptomatic women to women with PFPS, females with PFPS demonstrated a 20% deficit in knee extensor strength compared with the asymptomatic women [31]. The findings of the current study suggest that a higher number of PT visits over a longer duration can influence improvements in knee extension strength, thus highlighting the potential role of episode of care dosage on knee extension impairment.
Guney, Yuksel, Kaya, and Doral [32] investigated the relationship between concentric and eccentric quadriceps strengths with functional outcomes using the self-reported Kujala patellofemoral scores in female patients with unilateral PFPS. The authors reported that quadriceps eccentric and concentric strengths were significantly correlated with the Kujala score using Spearman’s correlation coefficient test. Piva, et al. [33] explored relationships between physical impairments of muscle strength, soft tissue length, movement control, postural and biomechanical alterations, and psychological factors with self-reported physical function and pain in patients with PFPS. The authors reported that factors related to these physical impairments did not associate to self-reported function or pain. Powers, Perry, Hsu, and Hislop [34] assessed functional limitations by using the functional assessment questionnaire and reported no correlation between function and quadriceps strength in patients with PFPS which differs from the current study’s findings. Research using strength as outcome measures is limited. Future research on specific exercise protocols involving strength outcomes is warranted.
Age might play a role in prescription of appropriate frequency and duration for patients with PFPS. PFPS occurs across the lifespan with a prevalence of 1 in 14 adolescents [35, 36]. In the current study, younger patients demonstrated greater improvements in knee extension strength and demonstrated increased odds of recovery. Rathleff, Roos, Olesen, and Rasmussen [37] studied adolescents, 15 to 19 years of age, who were cluster randomized to patient education with home exercises or patient education combined with exercise therapy 3 times a week for 3 months. Self-reported recovery was the primary outcome measure and was measured on a seven-point Likert scale ranging from “completely recovered” to “worse than ever”. This study assessed exercise adherence through weekly text messages and PT attendance, and found that a higher total number of weekly exercise sessions increased the odds of recovery which is in agreement with the findings of the current study [37]. However, van Middelkoop, van der Heijden, and Bierma-Zeinstra [38] found no difference in patient reported pain and function by questionnaire between adolescents and adults with PFPS. Rathleff, et al. [39] also reported lower success rates of treatment in adolescent patients with PFPS compared to adults who performed similar exercises and had comparable adherence when looking at the patient reported symptom duration in months through questionnaire. Further research that focuses on comparing strength and odds of recovery between younger and older individuals with PFPS is needed.
Limitations
The limitations of the current study include a small sample of patients with PFPS with a wide range of length of episode of care. All patients were seen in a single urban academic clinic under the care of a select group of physicians and physical therapists which limits generalizability. Pain scores using the VAS were only collected on 20 out of the 52 patients (38%) and functional outcome scores using the LEFS were only collected on 11 of the 52 patients (21%) at discharge, thus, limiting the ability to report change in patient-reported functional outcomes. However, despite the low power, we observed clinically important magnitudes of improvements that will be explored in future studies.
Conclusion
The current study describes episode of care variables and outcomes for management of PFPS at a single academic urban site. The results suggest that patients with a younger age and higher frequency and duration of PT visits demonstrated greater improvements in knee extension strength and odds of improvement. Over the course of a single episode of care, significant improvements can be made in reducing pain, increasing knee flexion and extension ROM, and improving knee extension strength. Each additional visit for patients with PFPS, up to 9 visits, and a younger age is associated with greater odds of making clinically significant improvements in pain intensity. Greater improvements in pain are associated with positive change in LEFS scores. Additional research is needed to fully elucidate therapy episodes of care for the management of patients with PFPS including analysis of timing, and frequency and duration in a larger setting.
Acknowledgements: The authors would like to thank Jason Falvey, PT, DPT, PhD for his assistance and contributions to this research study.
References
-
Glaviano NR, Kew M, Hart JM, Saliba S (2015) Demographic and epidemiological trends in patellofemoral pain. The International Journal of Sports Physical Therapy 10(3): 281-290.
-
Smith B, Smith BE, Selfe J, Thacker D, Hendrick P, et al. (2018) Incidence and prevalence of patellofemoral pain: A systematic review and meta-analysis. PLoS One 13(1): e0190892.
-
Collins NJ, Vicenzino B, van der Heijden RA, van Middelkoop M (2016) Pain during prolonged sitting is a common problem in persons with patellofemoral pain. Journal of Orthopaedic & Sports Physical Therapy 46(8): 658-663.
-
Papadopoulos K, Stasinopoulos D, Ganchev D (2015) A systematic review of reviews in patellofemoral pain syndrome. Exploring the risk factors, diagnostic tests, outcome measurements and exercise treatment. The Open Sports Medicine Journal 9: 7-17.
-
Lankhorst NE, van Middelkoop M, Crossley KM, Bierma-Zeinstra SM, Oei EH, et al. (2016) Factors that predict a poor outcome 5–8 years after the diagnosis of patellofemoral pain: a multicentre observational analysis. British Journal of Sports Medicine 50(14): 881- 886.
-
Clijsen R, Fuchs J, Taeymans J (2014) Effectiveness of exercise therapy in treatment of patients with patellofemoral pain syndrome: systematic review and meta-analysis. Physical Therapy 94(12): 1697-1708.
-
Hamstra-Wright KL, Aydemir B, Earl-Boehm J, Bolgla L, Emery C, et al. (2015) Lasting improvement of patient- reported outcomes 6 months after patellofemoral pain rehabilitation. Journal of Sport Rehabilitation 26(4): 223-233.
-
van der Heijden RA, Lankhorst NE, van Linschoten R, Bierma-Zeinstra SM, Van Middelkoop M (2016) Exercise for treating patellofemoral pain syndrome: an abridged version of Cochrane systematic review. European Journal of Physical and Rehabilitation Medicine 52(1): 110-133.
-
Dolak KL, Silkman C, Medina McKeon J, Hosey RG, Lattermann C, et al. (2011) Hip strengthening prior to functional exercises reduces pain sooner than quadriceps strengthening in females with patellofemoral pain syndrome: a randomized clinical trial. Journal of Orthopaedic & Sports Physical Therapy 41(8): 560-570.
-
Fukuda TY, Melo WP, Zaffalon BM, Rossetto FM, Magalhães E, et al. (2012) Hip posterolateral musculature strengthening in sedentary women with patellofemoral pain syndrome: a randomized controlled clinical trial with 1-year follow-up. Journal of Orthopaedic & Sports Physical Therapy 42(10): 823-830.
-
Herrington L, Al-Sherhi A (2017) A controlled trial of weight-bearing versus non–weight-bearing exercises for patellofemoral pain. Journal of Orthopaedic & Sports Physical Therapy 37(4): 155-160.
-
Witvrouw E, Lysens R, Bellemans J, Peers K, Vanderstraeten G (2000) Open versus closed kinetic chain exercises for patellofemoral pain. A prospective, randomized study. American Journal of Sports Medicine 28(5): 687-694.
-
Willy RW, Hoglund LT, Barton CJ, Bolgla LA, Scalzitti DA, et al. (2019) Patellofemoral pain: clinical practice guidelines linked to the International Classification of Functioning; Disability, and Health from the Orthopaedic Section of the American Physical Therapy Association. Journal of Orthopaedic & Sports Physical Therapy 49(9): CPG1-CPG95.
-
Winters M, Holden S, Lura CB, Welton NJ, Caldwell DM, et al. (2020) Comparative effectiveness of treatments for patellofemoral pain: a living systematic review with network meta-analysis. British Journal of Sports Medicine.
-
Holden S, Rathleff MS, Jensen MB, Barton CJ (2018) How can we implement exercise therapy for patellofemoral pain if we don’t know what was prescribed? A systematic review. British Journal of Sports Medicine 52(6): 385.
-
Young JL, Rhon DI, Cleland JA, Snodgrass SJ (2018) The influence of exercise dosing on outcomes in patients with knee disorders: a systematic review. Journal of Orthopaedic & Sports Physical Therapy 483(3): 146-
-
Carmen KL, Dardess P, Maurer M, Sofaer S, Adams K, et al. (2013) Patient and family engagement: a framework for understanding the elements and developing interventions and policies. Health Affairs 32(2): 223- 231.
-
Crossley KM, Bennell KL, Cowan SM, Green S (2004) Analysis of outcome measures for persons with patellofemoral pain: which are reliable and valid? Archives of Physical Medicine and Rehabilitation 85(5): 815-822.
-
Norkin CC, White DJ (2016) Measurement of joint motion: A guide to goniometry. 5th (Edn.). Philadelphia, PA: F.A. Davis Company.
-
Dutton M (2004) Dutton’s Orthopaedic Examination, Evaluation, and Intervention. New York, NY: McGraw Hill Medical.
-
Avers D, Brown M, Daniels, Worthinghams (2019) Muscle Testing: Techniques of Manual Examination and Performance Testing. St. Louis, MO: Elsevier.
-
Nelson EC, Berwick DM (1989) The Measurement of Health Status in Clinical Practice. Medical Care 27: S77-S90.
-
Binkley JM, Stratford PW, Lott SA, Riddle DL (1999) The Lower Extremity Functional Scale (LEFS): scale development, measurement properties, and clinical application. North American Orthopaedic Rehabilitation Research Network. Physical Therapy 79(4): 371-383.
-
Watson CJ, Propps M, Ratner J, Zeigler D, Horton P, et al. (2005) Reliability and responsiveness of the lower extremity functional scale and the anterior knee pain scale in patients with anterior knee pain. Journal of Orthopaedic & Sports Physical Therapy 35(3): 128-193.
-
Kendall FP, McCreary EK, Provance PG (1993) Muscles, Testing and Function. (4th Edn.), Baltimore, MD: Lippincott, Williams & Wilkins.
-
Binkley FM (1999) Measurement of functional status, progress and outcome in orthopedic clinical practice. Orthopaedic Division Review.
-
Davies ML, Goffman RM, May JH, Monte RJ, Rodriguez KL, et al. (2016) Large-scale no-show patterns and distributions for clinic operational research. Healthcare 4(1): 15.
-
Goldman L, Freidin R, Cook EF, Eigner J, Grich P (1982) A multivariate approach to the prediction of no-show behavior in a primary care center. Archives of Internal Medicine 142(3): 563-567.
-
Ofei-Dodoo S, Kellerman R, Hartpence C, Mills K, Manlove E (2019) Why patients miss scheduled outpatient appointments at urban academic residency clinics: a qualitative evaluation. Kansas Journal of Medicine 12(3): 57-61.
-
Van Tiggelen D, Witvrouw E, Coorevits P, Croisier JL, Roget P (2004) Analysis of isokinetic parameters in the development of anterior knee pain syndrome: a prospective study in a military setting. Isokinetics and Exercise Science 12(4): 223-228.
-
de Moura Campos Carvalho-E-Silva AP, Peixoto Leão Almeida G, Oliveira Magalhães M, Renovato França FJ, Vidal Ramos LA, et al. (2016) Dynamic postural stability and muscle strength in patellofemoral pain: is there a correlation? Knee 23(4): 616-621.
-
Guney H, Yuksel I, Kaya D, Doral MN (2016) The relationship between quadriceps strength and joint position sense, functional outcome and painful activates in patellofemoral pain syndrome. Knee Surgery Sports Traumatology Arthroscopy 24(9): 2966-2972.
-
Piva SR, Fitzgerald GK, Irrgang JJ, Fritz JM, Wisniewski S, et al. (2009) Associates of physical function and pain in patients with patellofemoral pain syndrome. Archives of Physical Medicine and Rehabilitation 90(2): 285-295.
-
Powers CM, Perry J, Hsu A, Hislop JH (1997) Are patellofemoral pain and quadriceps femoris muscle torque associated with locomotor function? Physical Therapy 77(10): 1063-1075.
-
Callaghan MJ, Selfe J (2007) Has the incidence or prevalence of patellofemoral pain in the general population in the United Kingdom been properly evaluated? Physical Therapy in Sport 8: 837-843.
-
Witvrouw E, Callaghan MJ, Stefanik JJ, Noehren B, Bazett- Jones DM, et al. (2014) Patellofemoral pain: consensus statement from the 3rd International Patellofemoral Pain Research Retreat held in Vancouver, September 2013. British Journal of Sports Medicine 48(4): 411-414.
-
Rathleff MS, Roos EM, Olesen JL, Rasmussen S (2015) Exercise during school hours when added to patient education improves outcome for 2 years in adolescent patellofemoral pain: a cluster randomized trial. British Journal of Sports Medicine 49(6): 406-412.
-
van Middelkoop M, van der Heijden RA, Bierma- Zeinstra SMA (2017) Characteristics and outcome of patellofemoral pain in adolescents: Do they differ from adults? Journal of Orthopaedic & Sports Physical Therapy 47(10): 801-805.
-
Rathleff MS, Vicenzino B, Middelkoop M, Graven-Nielsen T, van Linschoten R, et al. (2015) Patellofemoral pain in adolescence and adulthood: same same, but different? Sports Medicine 45(11): 1489-1495.
- Electrolyte Considerations for Athletes
- Comprehensive Rehabilitation in Adults with Diabetic Peripheral Neuropathy: A Literature Review on Frequency, Intensity, and Duration Parameters
- Exercise Duration and Its Association with ADHD Symptom Severity in Children and Adolescents: A Parent-Reported Survey Study
- Adaptation of the Adult Neurophysiology of Pain Questionnaire for Use in Pediatrics
- A Non-Pharmacological Multidisciplinary Pain Program within a Hospital Wellness Program: A Mixed Methods Study
- The Effect of Frenkel's Exercise with PNF on Functional Reach in Stroke Survivors: A Randomized Control Trial