The Effectiveness of Physical Therapy in Cervical Dystonia and its Response with Botulinum Toxin: A Case Report
Cervical dystonia is characterised by involuntary cervical muscles contraction leading to inappropriate posture of neck. Numerous causal factor involvements are there. Both pharmacological and physiotherapy need to be incorporated in the treatment. In this case report the patient is a 57 year old male having cervical dystonia and also having frozen shoulder with pain over the contralateral side. Physiotherapy treatment had been started prior to pharmacological intervention for both cervical dystonia and frozen shoulder. Here we tried to reduce the symptoms for cervical dystonia by exercises but due to presence of frozen shoulder the improvement got affected. The cervical dystonia improvement is monitored by Toronto Western Spasmodic Torticollis Rating Scale (TWSTRS).Physiotherapy had been continued after injection of botulinum toxin and the outcome was measured with TWSTRS comparing with the baseline.
Introduction
Cervical dystonia (CD), characterized by involuntary contractions of cervical muscles leading to awkward postures of the head and neck [1] and impaired motor control with concurrent activation of both agonist and antagonist muscles, is the most common form of focal dystonia. Predisposing factors can include peripheral trauma [2] and there is some suggestion of familial links [3]. The pathophysiology of cervical dystonia remains unclear and presented with numerous theories however in some studies they have told regarding disturbances in the basal ganglia, in particular the lent form nucleus [3]. The condition is characterized by abnormal posturing of the head and neck due to involuntary movement that can be tonic or phasic in nature. Combination of postures present in cervical dystonia: rotation (torticollis);
lateral tilting (laterocollis); flexion (anterocollis); extension (retrocollis); and lateral shift. In some cases there is additional involvement of the face, shoulder girdle, upper limbs or trunk [4]. Botulinum toxin (BTX) is the treatment of choice for focal dystonia. However, some authors recommend a multidisciplinary approach to Cervical Dystonia including physical therapy (PT) for better results [4, 5, 6]. There are a few studies on the effects of PT in patients with CD. Rondot, et al. (1991) recommend a combination of anticholinergic drugs, local botulinum toxin injection and rehabilitation to manage dystonia and secondary impairments [7, 8]. Although some authors mention physiotherapy management for cervical dystonia there are no studies looking at type or efficacy [9, 10].
A 57 years old male patient referred to the physiotherapy outpatient department of a Tertiary care center of North East India with diagnosis of cervical dystonia and had been referred for neck exercises. The patient has chief complaint of uncontrolled neck movement towards right side and pain with stiffness of the left shoulder joint. According to the patient he developed involuntary neck movement from last 3 months. Initially 7 months back he developed mild on and off pain over posterior cervical region and eventually he developed pain over left shoulder. Pain over the left shoulder gradually increased and restriction of movement started. Patient could not control his neck movement i.e. rotation towards right side (Torticollis) and tilting towards left side (leterocollis) both in static and dynamic posture. Patient developed frozen shoulder with gross shoulder movement restriction and was plan for intra articular dopemedrol injection. Since patient is a diabetic and is on oral hypoglycaemic drugs intraarticular injection had being delayed until the blood sugar level got stable. Normal findings for MRI cervical spine found with no visible abnormality over the cervical intervertebral disc. There is a history of severe pain over the lower cervical region after excessive writing 7 months back otherwise there was no history of any trauma or fall or any familial history of similar illness. Patient has a hectic schedule comprising of excessive writings and paper work and poor posture habit in workplace and in home.
On physical examination tenderness present over the craniocervical region (grade1), over the right mastoid region (grade 1),over the right splenius capitis muscle(grade1) ,over the left Sternocleidomastoid muscle (grade 1) and over the C6 , C7 and T1 spinous process and paraspinal muscle (grade 1). Spasm present over the cervical paraspinal muscles and bilateral trapezius muscle (cervical portion). The patient has involuntary rotation of the head towards right side and mild tilting of the head towards left side. Sensation is normal over the extremities and without any motor deficit. The left shoulder has limited range of motion with pain over the end range. The external rotation was maximally affected followed by internal rotation, abduction, extension and last the flexion. The resisted isometrics for the left shoulder muscles were weak and painful. There was tenderness over the anterior joint line (grade 1) and acromial region (grade 2) of the left shoulder. No swelling or any deformity present over the left shoulder. The left shoulder has been diagnosed with adhesive capsulitis. The initial assessment for cervical dystonia also included the Toronto Western Spasmodic Torticollis Rating Scale (TWSTRS) which is a clinical tool for assessing and documenting the status of the patient. The baseline total score of TWSTRS for the patient is 33. Intervention and Outcome The physiotherapy management for cervical dystonia has been tailored according to the patient requirement and the standardized physical therapy program. Patient was prescribed with anticholinergic drugs for cervical dystonia. Adhesive capsulitis was managed with regular physiotherapy and NSAIDS. The physiotherapy treatment sessions were kept daily. Passive stretching of the dystonic muscles (i.e. left Sternocleidomastoid muscle, right scalene muscle) were done along with gentle passive movement of the cervical spine in all the planes. PNF stretching (contract relax technique) was used for stretching the dystonic muscles. Activation of cervical antagonist muscle i.e. right Sternocleidomastoid muscle and left scalene muscle in the form of isometric contraction for voluntary control was done. Functional training incorporated along with the activity of daily living. Re-education of the movement is done with the help of feedback given to the patient and in front of the mirror while doing the active movements in all the planes. Craniocervical muscle endurance training given where we concentrate the deep cervical flexor muscles. Application of Ultrasound therapy over the tender area to relief symptoms thereby took chances to reduce any restriction of movement because of pain.
Ergonomic instructions given by postural re-education to limit excessive flexed head positions during occupational, recreational activities and other daily activities. Cry therapy for 15 minutes was given for reducing spasm present over the bilateral upper trapezius and cervical paraspinal muscles. The pulsed ultrasound was given to the left shoulder joint capsule to assist in reducing inflammation. Cryotherapy was given to reduce pain and muscle guarding. Pain free active assisted movement and passive movement at the pain free range was given .Joint mobilization to restricted accessory and joint play motions given. Strengthening exercises given to rotator cuff muscles in the form of isometrics contraction and to the scapular depressors and upward rotators. PNF strengthening exercise contract relax in PNF pattern to the left shoulder given.
Outcome
The patient received treatment for 3 weeks 5 days a week and 1 hour 30mins per session. According to the patient he got relieved from the pain over the cervical region and the trapezius. He was also getting ease of doing the functional activities .The intensity of the involuntary neck movement in static posture has come down but during dynamic posture like during walking the rotatory and tilting movement remain same. The left shoulder mobility deficit does not have much improvement except the rotator cuff muscle power increased. The patient took dopemedrol intraarticular injection after blood sugar got stable. The patient took botulinum toxin injection for dystonic muscles after another 1 week of physiotherapy treatment i.e. after 4 weeks. Patient had been advised by neurologist to resume the physiotherapy treatment immediately after botulinum toxin injection. The TWSTRS score found after 4 weeks of physiotherapy intervention was 11. The follow up visits after intra articular injection and botulinum toxin injection became irregular may be because of occupational busy schedule or may be reluctant of continuing the treatment in the same setting and opting for a higher centre or maybe he felt that he had improved to the point where he required.
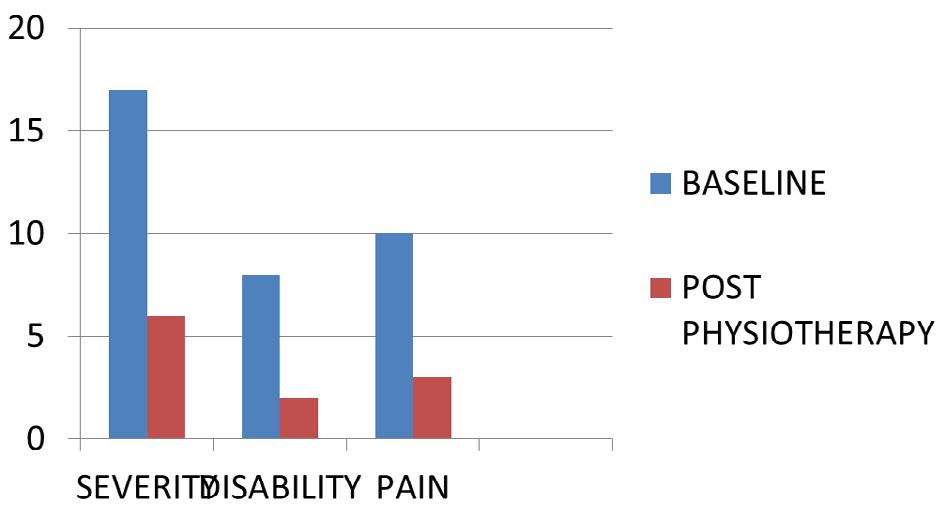
Fgure1: The improvement in the symptoms can be seen with reduce scores in TWSTRS.
Discussion
This Case Report demonstrates an improvement in neck abnormal movement, pain and disability, as measured by the TWSTRS, after a standardized and individual based tailored physiotherapy management for cervical dystonia patient with associated musculoskeletal problems. In this study cervical dystonia in itself a difficult movement disorder where abnormal muscle contraction takes place was worsened by the adhesive capsulitis in the ipsilateral side of dystonic muscle. Though the physiotherapy management was for symptomatic relief it gave improvement in severity, disability and pain scale in TWSTRS.
While during application of different procedures in adhesive capsulitis the involuntary movements in cervical dystonia worsens due to exertion and stress. By this it appears that any pathology near to the cervical my worsen the symptoms and exacerbate to a new increased level of severity, disability and pain .Although the study lacked the follow up visits and unable to complete the sessions. The post Botulinum toxin injection follow-ups could not be made and TWSTRS score was not measured. Unfortunately a very few studies had been done where physiotherapy intervention in cervical dystonia present .The goal was to achieve full range of motion for the left shoulder with strong muscle contraction and thereby we could have correct the misalignment in cervical more specifically. Both the intervention for adhesive capsulitis and cervical dystonia may affect each other. Some studies had shown an improvement in severity and disability with physiotherapy intervention along with botulinum toxin. One of the studies proposed the application of Functional Electrical Stimulation for the treatment of patients with Cervical Dystonia [11]. Muscle dystonia and abnormal postures impair effective and functional contraction of antagonist muscles, which may lead to muscle hypotonia due to disuse. In addition to muscle contraction of target non-dystonic cervical muscles, the external electrical current used in FES also causes, through reciprocal innervations, relaxation of dystonic muscles that have already been treated with BTX. In future study the recommendation for use of FES along with the standardised physical therapy programme is suggested. Rondot, et al. (1991) recommend a combination of anticholinergic drugs, local botulinum toxin injection and rehabilitation to manage dystonia and secondary impairments [8]. This single case study lacks the extended review period where we could have found the exact effect of botulinum toxin and physiotherapy intervention .A future study is needed comprising of large sample size with homogenous purposive sampling where standardised physiotherapy intervention and botulinum toxin injection to be applied together which may give a better outcome.
Conclusion
This case study has concluded that a tailored based physiotherapy is essential along with the pharmacological intervention to reduce the severity, disability and pain in cervical dystonia and consideration of associated factors like adhesive capsulitis, cervical muscle strain and poor postural habbits in cervical dystonia are required to be evaluated and managed to reduce overall symptoms.
References
-
Camfield L, Ben- ShlomoY, Warner TT (2002) Impact of cervical dystonia in quality of life. Epidemiological Study of Dystonia in Europe Collaborative Group. Mov Disord 17(4): 838-841.
-
Tintner R, Jankovic J (2001) Botulinum toxin for the treatment of cervical dystonia. Expert Opinion in Pharmacotherapy 2(12): 1985-1994.
-
Berardelli A, Rothwell JC, Hallett M, Thompson PD, Manfredi M, et al. (1998) The pathophysiology of primary dystonia. Brain 121(7): 1195-1212.
-
Gita ramdharry (2006) Case Report: Physiotherapy cuts the dose of botulinum toxin. Physiother Res Int 11(2): 117-122.
-
Ramdharry G (2006) Case report: physiotherapy cuts the dose of botulinum toxin. Physiother Res Int 11(2): 117-122.
-
Smania N, Corato E, Tinazzi M, Montagnana B, Fiaschi A, et al. (2003) The effect of two different rehabilitation treatments in cervical dystonia: preliminary results in four patients. Funct Neurol 18(4): 219-225.
-
Tassorelli C, Mancini F, Balloni L, Pacchetti C, Sandrini G, et al. (2006) Botulinum toxin and neuromotor rehabilitation: an integrated approach to idiopathic cervical dystonia. Mov Disord 21(12): 2240-2243.
-
Rondot P, Marchand MP, Dellatolas G (1991) _Spasmodic_ _torticollis_ — review of 220 patients. Canadian Journal of Neurological Science 18(2): 143-151.
-
Van Herwaarden GMFM, Anten HWM, Hoogdin CAL, Niewold JUR, Roos RAC, et al. (1994) Idiopathic spasmodic torticollis: a survey of the clinical syndromes and patients’ experience. Clinical Neurology and Neurosurgery 96(3): 222-225.
-
Bressman S, Greene P (2001) Dystonia. Current Treatment Options in Neurology 2: 275-285.
-
Mariana Araujo Ribeiro Queiroz, ChienHF, Sekeff Sallem FA, Barbosa ER (2012) Physical therapy program for cervical dystonia: a study of 20 cases. Functional Neurology 27(3): 187-192.
- Electrolyte Considerations for Athletes
- Comprehensive Rehabilitation in Adults with Diabetic Peripheral Neuropathy: A Literature Review on Frequency, Intensity, and Duration Parameters
- Exercise Duration and Its Association with ADHD Symptom Severity in Children and Adolescents: A Parent-Reported Survey Study
- Adaptation of the Adult Neurophysiology of Pain Questionnaire for Use in Pediatrics
- A Non-Pharmacological Multidisciplinary Pain Program within a Hospital Wellness Program: A Mixed Methods Study
- The Effect of Frenkel's Exercise with PNF on Functional Reach in Stroke Survivors: A Randomized Control Trial