Occupational Therapy Program for Children with Autism Spectrum Disorder to Improve Trousers-wearing Motion in the Standing Position
The purpose of this study was to investigate whether play-based occupational therapy improves the motions of children with autism spectrum disorder (ASD), who have difficulty putting on trousers in a standing position. The participants included 25 children comprising 16 boys and 9 girls (age range: 5 years and 3 months to 8 years and 2 months; IQ: 82–117) who were diagnosed with ASD (including pervasive developmental disorders and attention-deficit hyperactivity disorder). The intervention was conducted one-on-one between the therapist and the participant for 60 minutes. The participants performed a one-legged stand and trousers-wearing motions before and after the intervention. The analysis parameters for the task were foot pressure and center of pressure (COP) and motion analysis using video data. Each parameter of the one-legged stand showed no intervention effect. In contrast, the maximum excursion and total trajectory of COP in the anterior–posterior direction of the first support leg decreased significantly after the intervention compared to that before the intervention (p=0.049, 0.018). After the intervention, the trouser-wearing motion improved by three points. The participants found it easier to maintain a forward bend of the trunk while standing on one leg. Further, the foot of the first swing leg no longer got caught in the hem of the trousers. In addition, the participants improved their grasp of the waist edge of the trousers during the trouser-wearing motion. These findings suggest that the trousers-wearing motion produced a task-specific effect.
Introduction
Autism spectrum disorder (ASD) refers to developmental disorders characterized by two main symptoms, namely “impairments in social communication and social interaction” and “limited or repetitive behaviors, interests, and activities” [1, 2]. Social impairment is a qualitative impairment in our interaction with others. For example, people with social impairment are unable to make eye contact, gesture, share emotions, or understand; lack interest in their peers; have difficulty playing pretend and with social responses. Such behaviors and interests have limited, repetitive, and stereotypical styles. Examples include repeated hand flapping, resistance to changes in behavior patterns, and insistence on eating the same food and wearing the same clothes every day. They are also hypersensitive to sounds, smells, and touch and may be reluctant to be touched. Further, there are areas where their senses are dull. For example, they may not be bothered by dirt. Children with ASD often show these characteristics from an early age and experience difficulties in their social life.
According to the Diagnostic and Statistical Manual of Mental Disorders (DSM) IV published in 1994, which provides adequate diagnostic criteria and classification categories published by the American Psychiatric Association, the subcategories of pervasive developmental disorder include autistic disorder, Asperger syndrome, and pervasive developmental disorder not otherwise specified. However, in the DSM-5 diagnostic criteria published in 2013, Asperger syndrome and pervasive developmental disorder include a continuum of symptoms that cannot be clearly classified, the diagnosis of ASD is included, and a severity classification for each symptom is added [3, 4]. This criterion is well in line with the decisions made by the DSM-5 in the revised World Health Organization International Statistical Classification of Diseases and Related Health Problems [5]. The incidence of ASD in Japan in boys was 2.2 times that in girls, with a prevalence of 3.22%. The cumulative incidence of ASD at the age of 5 years was 1.31% (95% CI: 1.00–1.62) [6]. However, only 11.5% of these children have ASD alone, whereas the remaining 88.5% have at least one coexisting neurodevelopmental disorder [6].
Studies investigating the relevance of mild neurological dysfunction (MND) in children with ASD reported that the specific dysfunctions frequently found in ASD include dysfunction in posture and muscle tone, impaired fine motor control and coordination, excessive association movements, and motor impairment [7, 8, 9, 10]. In contrast, the central nervous system, which is affected by ASD, is associated with the cerebellum, cerebellar circuits, medial prefrontal cortex, basal ganglia, and brain stem [11, 12, 13, 14, 15, 16]. During the two-year follow-up, the volume of the entire corpus callosum and its substructure was measured, and it was confirmed that the volume of the entire corpus callosum was persistently reduced in autistic children compared to the control group [17]. In addition, the neurobiological wiring of motor function in autism by motor-related potentials may bypass the supplementary motor cortex and primary motor cortex pathways [18]. Behavioral analyses have reported that standing posture in ASD has a significantly smaller center of lateral pressure (COP) shift [19], a repetitive COP pattern, and less complex postural control [20]. Therefore, these functional impairments in ASD have a negative impact on the activities of daily living.
Researchers are often consulted by schoolteachers about children who have difficulty changing their clothes. Dressing behaviors include mistaking the front and back of the upper and lower garments, mistaking the dressing procedure, and taking time to change. Although parents do not consider these behaviors a problem in preschool children, they become a problem in later life. School teachers have difficulty dealing with the highly individualized daily activities of children because they focus on the entire classroom. The dressing behavior of children who are “not good at changing clothes” is also perceived as strange by other children, and they thus become targets of “bullying,” which often leads to their non- attendance at school.
Many children with ASD who use our daycare service for children with disabilities (described below) have difficulty changing their clothes. Of the 446 children with ASD using the service, 161 (36.1%) were perceived to be “unskilled at changing clothes” by their parents or staff. Approximately half of these (n = 92) were preschool-aged children. Both pre- and post-school children showed trunk hypotonia and high trunk sway during changing of clothes. Therefore, children with ASD need more time to change their clothes owing to repetition of the same process, carrying it out sluggishly, or using compensatory movements. In other words, developmental barriers include not only cognitive aspects, such as the front/back/left/right of clothing and movement procedures, but also motor tasks that make it difficult to carry out the dressing activity itself.
Interventions in children with ASD have been reported to improve balance and motor execution [21, 22, 23, 24, 25]. Studies on the activities of daily living have investigated the relationship between sensory processing problems and the number of eating problems in children with ASD [26, 27] and that between self-care and visual performance in young children with ASD [28]. In addition, the occupational therapy practice framework of the American Occupational Therapy Association showed that in the section on Dressing, there is a description of “selecting clothing and accessories according to time of day, weather, and occasion; obtaining clothing from storage; sequential dressing and undressing; tightening and adjusting clothing and shoes; putting on and taking off personal devices, prosthetics, and orthotics; and putting on and taking off personal tools, prosthetics, and splints.” [29]; however, to the best of our knowledge, the movement tasks of children who feel “unskilled at dressing” have not yet been examined. To improve posture, muscle tone, and coordination of the upper and lower limbs necessary for dressing in the standing position, we conducted a play-based occupational therapy (OT) intervention for children with ASD. They were asked to put on their trousers in a standing position, and the effect of the OT program was investigated.
Subjects and Methods
Participants
The participants included 25 children comprising 16 boys and 9 girls, with ages ranging from 5 years and 3 months to 8 years and 2 months and IQs 82–117 who were diagnosed with ASD (including pervasive developmental disorders and attention-deficit hyperactivity disorder) by a pediatrician or a child psychiatrist, and who used child development support and participated in after-school day service programs provided by a specialized facility for day-care support for children with disabilities. Regarding the eligibility criteria, participants needed to be between 5 and 8 years old and able to verbalize. The following were the exclusion criteria: any health issues that could affect balance (including balance disorders, neurological diseases, or a history of seizures), medication changes within the six weeks prior to participation, any significant surgery within the six months prior to testing, or a history of self-injury or injury to others in a routine therapy setting. Because of the focus on the immediate effects of a therapy routine and the pilot nature of this study, any exclusion criteria related to whether or not the participant had past experience with sensory integration (SI) therapy were not set. The role of day-care support facilities for children with disabilities in Japan is to provide children with physical disabilities, intellectual disabilities, or mental disabilities (including those with developmental disabilities) with guidance on basic daily activities; to impart knowledge and skills; to train them to adapt to group life; and to provide other benefits specified by the Ministry of Health, Labor and Welfare Ordinance. The program was launched in April 2012.
Ethical Considerations
The participants and their parents read and understood the instructions for the study and participated voluntarily.
The criteria for participation were that the child had no cognitive or skeletal muscle problems and that the child understood that he/she should wear trousers in a standing position. Ethical approval for this study was granted by the Ethics Committee of the Yamagata Prefectural University of Health Sciences (date of approval: September 27, 2018; approval number: 1809-18).
Test and Measurements
For the clinical profile, the participants’ height, weight, foot length, and foot width were measured. The sensory sensitivity of the participants was examined using the Short Sensory Profile [30, 31].
Tasks and OT Intervention
- OT intervention method: The therapist and the participant had a one-on-one session.
- The OT intervention period was approximately 60 minutes.
- The order of the OT interventions was introduction, play selection, play execution, and reflection.
- The OT intervention content consisted of nine types of play (Table
The OT interventions were based on the needs of each child and included the following ten key therapeutic strategies that a therapist would use when providing SI- based treatment to a child: (1) arranging the room to entice engagement, (2) ensuring physical safety, (3) presenting sensory opportunities, (4) attaining and maintaining optimal arousal levels, (5) tailoring activities to present the just-right challenge, (6) ensuring that activities are successful, (7) guiding the self-regulation of behavior, (8) creating a playful context, (9) collaborating in activity choice, and (10) fostering therapeutic alliances. The 10 areas are encompassed under the following three main areas: (1) providing the child with environmental modifications and sensory opportunities during the treatment session, (2) fostering adaptive responses and providing the just-right challenge, and (3) promoting the therapist–child relationship [33, 34, 35].
| Stage 1 | Stage 2 | Stage 3 | |
|---|---|---|---|
| Spontaneous play | Getting on the swing | Jumping in the big cloth bag | Jumping on a trampoline |
| Spontaneous play | (1) Participants ride while lying on their stomachs or on their backs with their faces up. | (1) Participants enter the large cloth bag, grasp the end of the bag, and stand up. | (1) Participants jump in the same position on the trampoline. |
| Spontaneous play | (2) Participants ride on a straddling seated position. | (2) Participants enter the large cloth bag and jump with the bag | (2) Participants change direction by about 90 degrees while jumping on the trampoline. |
| Spontaneous play | (3) Participants stand and pedal the swing. | Participants move with the large cloth bag by jumping back and forth or in left and right directions. | (3) Participants catch balloons and balls while jumping on the trampoline. |
| Non-competitive game | Climbing up and down a 2-meter high ladder | Climbing up and down a 2-meter high bouldering wall | Climbing up and down a 2-meter high giant cushion |
| Non-competitive game | (1) Participants climb up the ladder. | (1) Participants climb up the bouldering wall. | (1) Participants climb up the giant cushion. |
| Non-competitive game | (2) Participants climb down the ladder. | (2) Participants climb down the bouldering wall. | (2) Participants climb down the giant cushion. |
| Non-competitive game | (3) Participants climb up and down the ladder. | (3) Participants climb up and down the bouldering wall. | (3) Participants climb up and down the giant cushion. |
| Competitive game | 9 m race in a posture of crawling on hands and knees | 9 m race in a high crawling posture position | 9 m race on a scooter board of high crawling |
| Competitive game | (1) Participants compete with the staff. | (1) Participants compete with the staff. | (1) Participants compete with the staff. |
| Competitive game | (2) Participants will compete in a time trial. | (2) Participants will compete in a time trial. | (2) Participants will compete in a time trial. |
Table 1: Concepts of occupational therapy interventions Table 1: Concepts of occupational therapy interventions
Getting on the Swing Play
Swing Getting on the play is a three-step process (Figure 1). The participants held the ropes and rode the swings in each step. In the first step, the participants rode the swing while lying on their stomachs or face up. This process aimed to improve the muscle tone of the participant’s trunk. In the next step, the participants rode in a straddling sitting position, which improves the coordination of the trunk and upper and lower limbs, as well as balance ability in the sitting position while eliciting the external rotation abduction position of the participants’ hip joints. In the final step, the participants rowed the swing in a standing position. This process aimed to elicit smooth movements from the participant’s feet to the knee and hip joints, as well as to elicit coordinated movements of the trunk and upper limbs and to improve the participant’s balance ability in the standing position.

Jumping in the Big Cloth Bag Play
Jumping in the big cloth bag play was a three-step process (Figure 2). In the first step, the participant entered the large cloth bag, grasped the end of the bag, and stood up. This process aimed to allow the participants to adapt to the sack while moving their body, grasp the end of the sack, and maintain the standing position. In the next step, the participant entered a large sack and jumped with the bag. This process aimed to enhance the participant’s ability to maintain a sustained grasp of the object by keeping their body in position with the large bag and not letting go of the bag end. In the final step, the participant moved with the large sack by jumping back and forth or in the left and right directions. This process aimed to maintain the positional relationship between the body and the bag and a sustained grasp of the bag edge while performing dynamic body motions in the large bag.
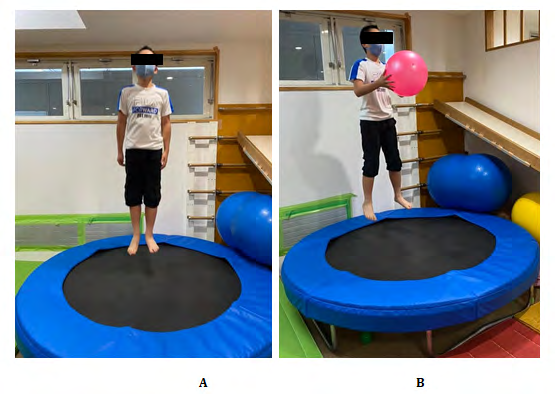
Jumping on the Trampoline Play
Jumping on trampoline play was a three-step process (Figure 3). First, the participant repeatedly jumped in the same position on a trampoline (Powerful Trampoline: T-200, Mirai-Koji Co. Itoshima, Japan). This controlled the trunk and lower limb so that the participants would not lose their posture when jumping their body in the air. Next, the participant turned around by approximately 90° while jumping on the trampoline. The goal of this process was to further improve body control by allowing the participant’s body to perform active motions in the air. Finally, the participant jumped on the trampoline while catching balloons and balls thrown by the therapist, encouraging spatial awareness and eye–hand coordination while maintaining a high level of postural control as the participant jumped and caught balloons or balls flying towards them.

Climbing up and down a2-metter high ladder
The climbing jungle gym game was a three-step process using a fixed jungle gym about two meters high (custom- made: Kanon Co., Hiroshima, Japan; (Figure 4). In the first step, the participant repeatedly climbed up the jungle gym to reach the goal, while descending by another method. This can improve the coordination of the upper and lower limbs and maintain their posture. In the next step, the participant repeatedly climbed down the jungle gym to reach the goal. Climb-up was performed using another method. Similarly, the participant performed again a series of motions to climb up and down the jungle gym, which encouraged spatial cognition and eye–hand coordination while maintaining high postural control as participants ascended and descended the jungle gym.
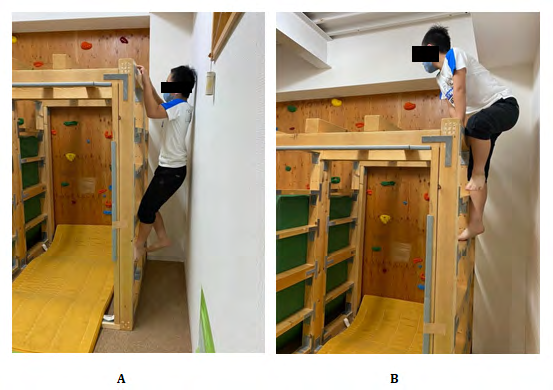
Bouldering Wall-Climbing Game
This was a three-step process using ‘holds’ irregularly fixed on a wall approximately 2 m high and 5 m wide (Figure 5). In the first step, the participant climbed through an irregular array of “holds” toward the goal (Climbing Holds: Atomik climbing holds, Provo, USA) with a different method used for descent. This process improves the coordination of the upper and lower limbs while the participants looked at the goal, grasped the irregular “holds,” and maintained their posture. The participant then descended from the bouldering wall to reach the goal that would improve the coordination of the upper and lower extremities while the participant grasped irregular “holds.” In the final step, the participants performed a series of ascents and descents on the bouldering wall, aiming to encourage spatial awareness and eye-hand coordination while maintaining high postural control as the participant climbed up and down the bouldering wall using irregular “holds.”
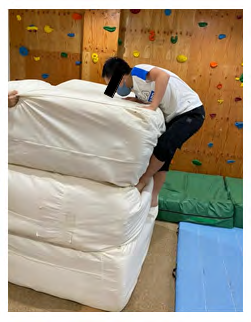
Climbing Giant Cushions Game
Eight giant cushions were used in this game, each approximately 1 m on each side: up and down, left and right, and two in front and behind (Figure 6). Participants ascended and descended the cushions, grasping them at each step of the process. In the first step, the participant climbed to the goal at the top, trying not to lose the cushions. A different method was used for the descent. This aimed to improve the coordination of the upper and lower limbs while the participants focused on the goal, to grasp the arbitrary position of the cushion, and to maintain their posture so that the cushion would not collapse. In the next step, the participant descended to the goal on the floor, trying not to break the cushion pile. This helps participants on how to use gravity to improve the coordination of their trunk and upper and lower limbs. Climbing was performed using a different method. In the final step, the participant climbed up and down a giant cushion. This process aimed to encourage spatial awareness and eye–hand coordination while providing high postural control that uses gravity to prevent the cushion from collapsing.

Crawling on all Fours Race
A 9 m course with mats was used for crawling on all fours’ race (Figure 7). In the first step, the participants crawled forward on all fours to overtake the therapist, which aimed to bring out the participants’ competitive spirit and increase their pace to the therapist’s speed. The therapist then adjusted the speed by observing the participants on all fours. The participants then crawled forward on all fours for 9 m at full speed. This encourages the participants to control their trunk and upper and lower limb motions, so they would not fall.

High Crawling Posture Race
The high crawling posture race involved using both hands and feet to extend the elbows and knees to move across a 9 m floor (Figure 8). In the first step, the participant competed with the therapist. This would bring out the participants’ competitive spirit and increase their pace to the therapist’s speed. The therapist then adjusted the speed by observing the situation of the participant. On a high crawling position, the participant crawled forward for 9 m at full speed. This process encourages the high control of the trunk and upper and lower limb motions.

High Crawling Posture Scooter Board Race
The high crawling posture scooter board race consisted of moving across a 9-m floor surface with elbows and knees extended and hands-on a scooter board (CR000281: Cramer Japan, Inc. Kumagay, Japan; (Figure 9).
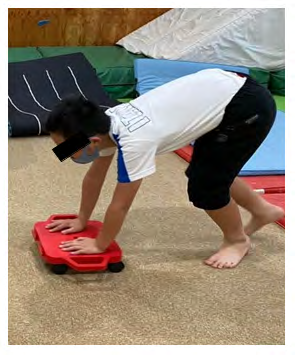
In the first step, participant crawled forward on all fours to overtake the therapist. This process aimed to bring out the participant’s competitive spirit and increase the pace of the therapist’s speed. The therapist then adjusted the speed by observing the crawling of the participant. In the next step, the participant crawled forward on all fours for 9 m at full speed. This process aimed to encourage the participants to control their trunk and upper and lower limb movements, so that they would not fall.
Instrumentation and Data Acquisition
The analysis parameters of the tasks were foot pressure and COP were recorded from the frontal plane and the right sagittal plane using two video cameras (C920; Logitech International SA, Lausanne, Switzerland). The temporal and spatial resolutions of the video camera were 30 Hz and 998,400 pixels (1,280 × 780), respectively. The experimental trousers used for putting on trousers in a standing position were 100% polyester trousers (2285030; Caroline Corp., Nagoya, Japan). Each participant was asked to put on the experimental trousers which measured 100 cm, 110 cm, 120 cm, 130 cm, or 140 cm, depending on the child’s height.
Foot pressure and COP were measured using a foot pressure platform (EM-MP2703; Noraxon USA, Arizona, USA) with a time resolution of 100 Hz and spatial resolution of 16 bits. The 40-cm × 57-cm platform was placed with the short side vertical to the frontal plane of the camera, and the long side was horizontal. The platform was calibrated at the time of the setup. The displacement of the COP was in the anterior–posterior direction of the short side of the platform, and the long side was in the medial–lateral direction. All devices were synchronized using the software (MR3 ver.3.12; Noraxon USA, Arizona, USA). The software was also used for measurement and analysis.
Experimental Tasks
Experimental task All participants performed two tasks before and after the OT intervention. Task 1: Participants were instructed to maintain a standing position with one leg open for a maximum of 10 s. They stood on one foot on the platform of the foot pressure distribution analysis device. The order of the one-legged stand and the position of the upper limb were determined by the participants. Task 2: The participants were instructed to put on the trousers while standing. The speed of the trouser-wearing motion was arbitrary.
Procedure
Tasks 1 and 2 before and after the OT intervention were conducted in a quiet, well-lit room (640 lux, temperature 24°C). The participants entered the room and were briefed on the tasks. The participants then stood upright on the platform. The measurements were performed in the order of task 1 and task 2. In task 1, the participants stood on one foot, either left or right, and were instructed to perform the task while looking at the fixation in front of them. For task 2, the participants took off the trousers that they were already wearing and were asked to put on and remove the trousers intended for the experiment. Finally, the they put on their own trousers to complete the task. The period from the start to the end of the task was approximately 10 min. During the measurement, breaks were taken as needed.
Definitions of Terms
Terms were defined as previously described [36]. Briefly, the first leg (FL) was the leg that first passed through the trousers. The second leg (SL) was the next swing leg after the FL; the SL passed through the trousers later. The first support leg (FSL) was the first support leg while the FL was passing through the trousers. The second support leg (SSL) was the next support leg after the FSL, which had already passed through the trousers.
Motion Phase
Task 2 was divided into five phases based on the video data as previously described [36]. The first phase was from the beginning of the trouser-wearing motion until the FL left the floor. The second phase was from the start of the FL motion until the leg was placed through the trousers. The third phase was from when the FL reached the floor to when SL left the floor. The fourth phase was the period from when the SL left the floor until it passed through the trousers. The fifth phase was the period from when the SL reached the floor until the waistline of the trousers was pulled up to the waist, completing the trouser-wearing motion.
The second and fourth phases were further divided into three smaller phases. The first stage was the period from when the FL or SL motions begin until either was raised to the trousers of the waistline. The second stage was the period from when the participant’s foot began to enter the trousers until the foot was fully inside the trousers. The third stage was the period from the end of the second stage until FL or SL landed on the floor.
Data Analysis
Based on the ON-OFF data of the platform and the moving images, task 1 was measured as the period from when the time one foot of the participant left the platform until the time it was grounded.
Statistical Analysis
The method of putting on and taking off the trousers worn by the participants and the experimental trousers was compared by several examiners to assess the reproducibility of the participants’ motions in task 2. Based on the video, the trouser-wearing motion was divided into five phases [36], and only phases 2 and 4 were analyzed. For tasks 1 and 2, the left and right one-legged standing times and foot pressure distributions were investigated. In addition to the maximum excursion of COP in the anterior–posterior direction (A/P- COP-max) and the maximum excursion of COP in the medial– lateral direction (M/L-COP-max), the COP trajectory length in the anterior–posterior direction (A/P-COP-trajectory) and the COP trajectory length in the medial–lateral direction (M/L-COP-trajectory) were calculated based on the temporal transition of COP.
The SPSS statistical software (version 24.0; SPSS, Chicago, IL, USA) was used for the statistical analysis. In tasks 1 and 2, the Student’s t-test was used to compare the one- legged standing time before and after the OT intervention. Wilcoxon’s signed rank-sum test was used to compare the change in the COP of the supporting leg and the trajectory length before and after the OT intervention. The significance level was set at 5%.
Results
The clinical profiles of each participant are shown in Table 2. Height ranged from 110.0 to 133.0 cm; weight, 14.3– 31.1 kg; foot length, 12.3–19.4 cm; and foot width, 3.2–9.8 cm. The minimum duration of the OT intervention was 5 months and the maximum was 4 years and 11 months.
The sensory profiles of each participant are shown in Table 3. Overall, 21 of 25 participants had a definite difference (above average + 2SD) in at least one of the six sensory sensitivity items. Of the six sensory sensitivity items, visual/auditory sensitivity had the greatest number of definite differences (n = 14).
The results of the COP transition for one-legged standing with eyes open are shown in Table 4. The mean time required to stand on the right was 8.8 s before the OT intervention and 6.9 s after the OT intervention, with a significant difference (p=0.013); that of the left foot was 7.7 s before the OT intervention and 6.8 s after the OT intervention, with no significant difference. Regarding the A/P-COP-max during one-legged standing, the mean values for the right foot before and after the OT intervention were 3.5% and 3.7%, respectively, whereas those for the left foot were 3.8% and
3.1%, respectively. There was no significant difference in A/P-COP-max before and after the OT intervention for both the left and right feet. Regarding the M/L-COP-max during one-legged standing, the mean value for the right foot was 7.0% both before and after the OT intervention, while for the left foot the mean values were 6.5% before and 6.7% after the OT intervention, with no significant difference. Regarding the A/P-COP-trajectory during one-legged standing, the mean value for the right foot was 5.1%/s and 5.8%/s before and after the OT intervention, respectively and for the left foot, 5.2%/s and 5.3%/s, respectively. There was no significant difference in the A/P-COP trajectory before and after the OT intervention for both the left and right sides. Regarding the M/L-COP-trajectory during one-legged standing, the mean values for the right and left legs were 3.3%/s and 3.1%/s before the intervention and 3.4%/s and 3.1%/s after, with no significance differences.
| Participant | Age | Diagnoses | Sex | Height (cm) | Weight (kgf) | Foot length (cm) | Foot width (cm) | During OT intervention |
|---|---|---|---|---|---|---|---|---|
| 01 | 6 years, 4 months | ASD | M | 115 | 16.5 | 13.7 | 3.5 | 2 years |
| 02 | 5 years, 8 months | ASD | F | 113 | 17.2 | 13.2 | 3.2 | 1 year, 4 months |
| 03 | 5 years, 3 months | ASD | M | 110 | 16.0 | 13.3 | 4.1 | 1 year, 3 months |
| 04 | 6 years, 5 months | ASD | M | 110 | 20.6 | 14.2 | 4.1 | 3 years, 2 months |
| 05 | 6 years, 5 months | ASD | M | 125 | 20.4 | 18.4 | 6.1 | 4 years, 11 months |
| 06 | 6 years, 11 months | ASD | M | 120 | 22.2 | 15.2 | 3.6 | 1 year, 4 months |
| 07 | 6 years, 4 months | PDD | M | 115 | 23.1 | 17.9 | 7.4 | 2 years, 5 months |
| 08 | 6 years, 4 months | ASD | F | 113 | 20.7 | 17.6 | 6.9 | 10 months |
| 09 | 8 years, 2 months | ASD | M | 129 | 23.9 | 19.2 | 8.7 | 4 years, 5 months |
| 10 | 5 years, 6 months | ASD | M | 110 | 15.3 | 16.1 | 7.1 | 11 months |
| 11 | 7 years, 6 months | ASD (PDD), ADHD | M | 127 | 27.2 | 18.1 | 7.4 | 5 months |
| 12 | 5 years, 11 months | ASD | F | 113 | 20.3 | 18.5 | 7.4 | 5 months |
| 13 | 8 years, 2 months | ASD | F | 133 | 29.9 | 15.9 | 4.3 | 2 years |
| 14 | 6 years, 5 months | PDD | M | 119 | 19.1 | 17.3 | 7.1 | 2 years, 4 months |
| 15 | 6 years, 8 months | ASD | F | 113 | 19.2 | 13.9 | 3.4 | 2 years |
| 16 | 6 years, 6 months | ASD | M | 117 | 23.0 | 19.0 | 7.0 | 2 years, 3 months |
| 17 | 6 years, 4 months | ASD | F | 110 | 14.3 | 12.3 | 3.9 | 4 years, 4 months |
| 18 | 5 years, 10 months | PDD | M | 115 | 21.4 | 14.3 | 4.1 | 2 years |
| 19 | 6 years | ASD | M | 113 | 18.3 | 12.7 | 3.8 | 1 year, 2 months |
| 20 | 7 years, 11 months | ASD | F | 120 | 21.5 | 13.6 | 4.0 | 2 years, 5 months |
| 21 | 7 years, 10 months | ASD | F | 133 | 30.0 | 19.4 | 9.8 | 1 years, 7 months |
| 22 | 6 years, 5 months | ASD, ADHD | M | 115 | 26.4 | 13.8 | 4.3 | 9 months |
| 23 | 8 years, 1 month | ASD (PDD) | F | 120 | 26.6 | 15.5 | 4.1 | 1 year, 4 months |
| 24 | 7 years, 10 months | ASD | M | 129 | 25.7 | 19.4 | 8.3 | 2 years |
| 25 | 7 years, 11 months | ASD (PDD), ADHD | M | 127 | 31.1 | 16.6 | 4.3 | 10 months |
| Max | 133.0 | 31.1 | 19.4 | 9.8 | ||||
| Min | 110.0 | 14.3 | 12.3 | 3.2 | ||||
| Mean | 118.6 | 22.0 | 16.0 | 5.5 | ||||
| SD | 7.4 | 4.7 | 2.4 | 2.0 |
Table 2: Clinical Profile.
| Participant | Sensory Sensitivity | |||||
|---|---|---|---|---|---|---|
| Participant | Tactile Sensitivity | Movement Sensitivity | Underresponsive/Seeks Sensation | Auditory Filtering | Low Energy/Weak | Visual/Auditory Sensitivity |
| 01 | ||||||
| 02 | ||||||
| 03 | ||||||
| 04 | ||||||
| 05 | ||||||
| 06 | ||||||
| 07 | ||||||
| 08 | ||||||
| 09 | ||||||
| 10 | ||||||
| 11 | ||||||
| 12 | ||||||
| 13 | ||||||
| 14 | ||||||
| 15 | ||||||
| 16 | ||||||
| 17 | ||||||
| 18 | ||||||
| 19 | ||||||
| 20 | ||||||
| 21 | ||||||
| 22 | ||||||
| 23 | ||||||
| 24 | ||||||
| 25 | ||||||
| c | Typical performance:Average value+1SDor less |
| Probable difference:Average value+1SD and lower range than average value+2SD | |
| Definite difference:Above average +2SD |
Table 4: Sensory sensitivity for each participant.
| Participant | One-legged standing time (s) | A/P-COP-max (%) | M/L-COP-max (%) | A/P-COP-trajectory (%/s) | M/L-COP-trajectory (%/s) | ||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Before OT | After OT | Before OT | After OT | Before OT | After OT | Before OT | After OT | Before OT | After OT | ||||||||||||||||||||
| R | L | R | L | R | L | R | L | R | L | R | L | R | L | R | L | R | L | R | L | ||||||||||
| 01 | 4.6 | 10.0 | 9.6 | 6.7 | 4.1 | 3.3 | 4.0 | 4.6 | 8.7 | 7.8 | 12.2 | 12.0 | 5.7 | 5.1 | 5.6 | 7.8 | 4.0 | 3.4 | 5.6 | 2.9 | |||||||||
| 02 | 7.9 | 6.4 | 6.5 | 4.6 | 4.2 | 4.8 | 2.7 | 2.5 | 10.3 | 8.5 | 9.2 | 5.3 | 5.3 | 5.5 | 4.7 | 4.1 | 4.7 | 3.1 | 2.9 | 2.4 | |||||||||
| 03 | 10.0 | 8.0 | 6.1 | 3.5 | 3.3 | 3.4 | 7.3 | 5.1 | 8.9 | 10.5 | 6.8 | 8.9 | 1.5 | 3.2 | 5.6 | 8.8 | 2.2 | 2.7 | 2.3 | 4.0 | |||||||||
| 04 | 4.0 | 3.2 | ー | ー | 3.4 | 3.5 | ー | ー | 7.0 | 5.4 | ー | ー | 5.1 | 5.8 | ー | ー | 3.5 | 4.4 | ー | ー | |||||||||
| 05 | 10.0 | 10.0 | 10.0 | 10.0 | 3.1 | 2.0 | 6.2 | 6.2 | 5.6 | 6.2 | 8.2 | 11.5 | 4.9 | 4.5 | 7.2 | 9.1 | 4.1 | 4.4 | 4.0 | 6.3 | |||||||||
| 06 | 6.9 | 10.0 | 2.6 | 6.1 | 7.6 | 7.4 | 8.0 | 6.4 | 15.6 | 16.4 | 10.5 | 12.3 | 9.9 | 7.3 | 8.8 | 8.6 | 4.5 | 3.0 | 5.6 | 3.3 | |||||||||
| 07 | 10.0 | 4.0 | 2.7 | 2.3 | 3.4 | 3.1 | 2.2 | 1.7 | 5.0 | 3.3 | 5.7 | 2.7 | 6.6 | 4.6 | 3.8 | 3.8 | 3.5 | 3.1 | 4.4 | 2.4 | |||||||||
| 08 | ー | ー | 10.0 | 10.0 | ー | ー | 2.1 | 2.7 | ー | ー | 3.9 | 4.3 | ー | ー | 4.6 | 4.8 | ー | ー | 2.1 | 1.9 | |||||||||
| 09 | 10.0 | 10.0 | 10.0 | 10.0 | 3.6 | 2.1 | 2.8 | 2.5 | 4.8 | 2.5 | 5.0 | 3.1 | 5.1 | 4.3 | 4.5 | 3.8 | 4.2 | 2.4 | 3.0 | 2.0 | |||||||||
| 10 | 10.0 | 5.4 | 2.8 | 2.3 | 3.6 | 2.7 | 3.5 | 1.5 | 4.6 | 6.1 | 3.5 | 3.1 | 7.1 | 2.3 | 6.0 | 5.0 | 3.9 | 2.3 | 3.4 | 3.4 | |||||||||
| 11 | 10.0 | 10.0 | 10.0 | 10.0 | 2.2 | 2.7 | 2.4 | 2.5 | 4.5 | 3.5 | 4.7 | 4.8 | 4.2 | 4.3 | 5.2 | 5.1 | 3.6 | 3.2 | 3.6 | 3.8 | |||||||||
| 12 | 7.0 | 10.0 | 10.0 | 10.0 | 2.1 | 1.5 | 1.5 | 2.2 | 9.3 | 2.3 | 3.0 | 3.5 | 5.3 | 4.2 | 3.8 | 4.8 | 3.9 | 1.9 | 2.1 | 3.1 | |||||||||
| 13 | 10.0 | 10.0 | 10.0 | 10.0 | 2.4 | 2.6 | 2.5 | 4.2 | 5.8 | 4.5 | 6.6 | 6.5 | 3.6 | 2.7 | 3.9 | 4.2 | 2.2 | 1.6 | 2.8 | 2.5 | |||||||||
| 14 | 9.2 | 3.0 | 6.6 | 5.2 | 2.8 | 5.0 | 6.7 | 4.1 | 4.3 | 6.7 | 12.5 | 7.4 | 4.1 | 13.3 | 10.5 | 5.4 | 2.5 | 6.4 | 4.2 | 4.2 | |||||||||
| 15 | 10.0 | 3.5 | 9.1 | 10.0 | 4.9 | 8.3 | 4.5 | 3.4 | 9.9 | 9.4 | 14.3 | 7.6 | 6.6 | 8.6 | 7.1 | 4.9 | 3.2 | 3.6 | 4.4 | 2.9 | |||||||||
| 16 | 10.0 | 3.2 | 6.6 | 5.7 | 1.9 | 1.9 | 2.8 | 1.8 | 4.6 | 2.2 | 4.1 | 3.4 | 4.2 | 4.5 | 3.6 | 4.7 | 2.6 | 1.6 | 3.2 | 4.1 | |||||||||
| 17 | 8.2 | 10.0 | 4.5 | 6.5 | 6.7 | 4.1 | 4.9 | 4.4 | 7.5 | 6.8 | 6.1 | 10.2 | 7.3 | 5.7 | 7.1 | 5.6 | 3.3 | 3.3 | 2.6 | 3.0 | |||||||||
| 18 | 10.0 | 9.2 | 4.8 | 7.7 | 4.2 | 8.6 | 3.6 | 2.1 | 7.4 | 9.4 | 8.2 | 6.9 | 6.6 | 6.7 | 8.2 | 5.0 | 3.5 | 3.5 | 3.5 | 3.4 | |||||||||
| 19 | 9.6 | ー | 4.9 | 4.7 | 5.2 | ー | 3.2 | 2.4 | 8.5 | ー | 9.2 | 8.5 | 5.5 | ー | 5.3 | 5.4 | 3.9 | ー | 2.8 | 2.5 | |||||||||
| 20 | 9.0 | 10.0 | 10.0 | 10.0 | 2.4 | 2.6 | 3.4 | 3.2 | 7.1 | 7.4 | 8.0 | 8.1 | 4.7 | 4.3 | 3.8 | 3.9 | 3.5 | 2.6 | 2.5 | 2.4 | |||||||||
| 21 | 10.0 | 7.7 | 9.3 | 4.6 | 1.6 | 2.5 | 2.0 | 2.2 | 3.2 | 2.4 | 4.0 | 2.3 | 3.5 | 3.5 | 3.4 | 4.7 | 2.3 | 2.2 | 2.5 | 2.6 | |||||||||
| 22 | 6.9 | 8.7 | 2.3 | 3.0 | 1.6 | 6.4 | 5.2 | 2.0 | 5.0 | 11.2 | 8.0 | 5.6 | 4.0 | 5.7 | 11.2 | 4.2 | 3.0 | 3.2 | 4.3 | 3.3 | |||||||||
| 23 | 7.0 | 6.2 | 3.3 | 9.6 | 4.8 | 4.3 | 3.5 | 4.6 | 10.9 | 10.4 | 6.4 | 11.0 | 5.2 | 6.3 | 7.5 | 4.9 | 3.2 | 4.3 | 4.5 | 2.9 | |||||||||
| 24 | 10.0 | 10.0 | 10.0 | 10.0 | 2.1 | 1.8 | 2.7 | 1.6 | 2.8 | 2.3 | 2.8 | 3.4 | 3.1 | 2.7 | 3.3 | 2.8 | 2.0 | 1.7 | 2.0 | 2.0 | |||||||||
| 25 | 10.0 | 7.6 | 4.3 | 1.6 | 1.8 | 1.4 | 2.2 | 1.6 | 7.2 | 4.1 | 5.9 | 7.1 | 4.0 | 3.9 | 4.9 | 5.8 | 3.1 | 2.7 | 2.8 | 3.3 | |||||||||
| Max | 10.0 | 10.0 | 10.0 | 10.0 | 7.6 | 8.6 | 8.0 | 6.4 | 15.6 | 16.4 | 14.3 | 12.3 | 9.9 | 13.3 | 11.2 | 9.1 | 4.7 | 6.4 | 5.6 | 6.3 | |||||||||
| Min | 4.0 | 3.0 | 2.3 | 1.6 | 1.6 | 1.4 | 1.5 | 1.5 | 2.8 | 2.2 | 2.8 | 2.3 | 1.5 | 2.3 | 3.3 | 2.8 | 2.0 | 1.6 | 2.0 | 1.9 | |||||||||
| Mean | 8.8 | 7.7 | 6.9 | 6.8 | 3.5 | 3.8 | 3.7 | 3.1 | 7.0 | 6.5 | 7.0 | 6.7 | 5.1 | 5.2 | 5.8 | 5.3 | 3.3 | 3.1 | 3.4 | 3.1 | |||||||||
| SD | 2.5 | 3.3 | 3.2 | 3.3 | 1.7 | 2.3 | 1.9 | 1.6 | 3.2 | 3.9 | 3.4 | 3.4 | 1.9 | 2.7 | 2.5 | 1.9 | 1.0 | 1.4 | 1.2 | 1.1 | |||||||||
| p-value | a: | 0.0133 | v: | 0.3326 | b: | 0.280 | w: | 0.126 | c: | 0.497 | x: | 0.439 | d: | 0.114 | y: | 0.413 | e: | 0.469 | z: | 0.452 |
Table 5: Center of Presure (COP) transition under one-legged standing with eyes open.
Table 4: Center of Presure (COP) transition under one-legged standing with eyes open. A-P indicated anterior to posterior side. A-P direction of COP amplitude (%/s) was normalized by dividing the COP amplitude by the foot length. L-M indicated lateral to medial side. L-M direction of COP amplitude (%/s) was normalized by dividing the COP amplitude by the foot width. OT indicates occupational therapy.
| Participant | One-legged standing time during wearing torsors (s) | A/P-COP-max (%) | M/L-COP-max (%) | A/P-COP-trajectory (%/s) | M/L-COP-trajectory (%/s) | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Before OT | After OT | Before OT | After OT | Before OT | After OT | Before OT | After OT | Before OT | After OT | |||||||||||||
| Side of FSL | FSL | SSL | Side of FSL | FSL | SSL | FSL | SSL | FSL | SSL | FSL | SSL | FSL | SSL | FSL | SSL | FSL | SSL | FSL | SSL | FSL | SSL | |
| 01 | R | 2.9 | 3.3 | R | 3.6 | 4.4 | 3.3 | 5.7 | 3.1 | 20.6 | 9.4 | 5.3 | 10.3 | 23.5 | 6.4 | 7.5 | 5.1 | 10.5 | 3.9 | 2.0 | 7.3 | 16.9 |
| 02 | R | 1.2 | 4.4 | R | 1.6 | 4.1 | 7.3 | 9.2 | 5.8 | 11.3 | 12.7 | 9.6 | 8.0 | 34.8 | 13.3 | 5.4 | 9.9 | 13.2 | 7.4 | 2.2 | 2.8 | 13.4 |
| 03 | L | 3.9 | 1.9 | L | 3.0 | 1.4 | 6.6 | 4.0 | 4.9 | 4.4 | 8.9 | 6.5 | 9.7 | 8.1 | 9.8 | 12.9 | 8.6 | 13.1 | 6.9 | 5.6 | 5.9 | 6.1 |
| 04 | L | 2.8 | 1.9 | L | 1.4 | 2.0 | 4.7 | 5.9 | 4.4 | 8.5 | 7.6 | 9.8 | 7.6 | 6.9 | 7.9 | 14.6 | 13.0 | 15.0 | 4.3 | 4.8 | 3.9 | 3.5 |
| 05 | L | 1.5 | 1.6 | L | 4.3 | 1.1 | 6.7 | 6.1 | 6.1 | 4.7 | 4.9 | 18.6 | 8.8 | 14.5 | 28.9 | 20.8 | 9.9 | 21.0 | 5.0 | 16.2 | 6.6 | 11.5 |
| 06 | L | 2.2 | 2.6 | L | 1.4 | 1.9 | 4.9 | 5.1 | 4.2 | 3.7 | 11.5 | 8.6 | 4.1 | 13.1 | 7.8 | 8.1 | 7.8 | 9.1 | 4.3 | 3.9 | 3.6 | 6.3 |
| 07 | R | 1.8 | 1.3 | R | 1.6 | 1.2 | 5.2 | 2.3 | 2.4 | 2.1 | 0.9 | 1.8 | 1.8 | 3.6 | 13.6 | 8.9 | 6.6 | 9.5 | 1.3 | 3.8 | 3.7 | 7.8 |
| 08 | L | 2.8 | 1.5 | L | 2.0 | 2.1 | 2.1 | 3.8 | 2.8 | 2.3 | 5.9 | 4.2 | 7.9 | 4.7 | 6.3 | 7.0 | 6.5 | 7.8 | 5.6 | 4.7 | 4.2 | 4.6 |
| 09 | L | 1.3 | 1.0 | L | 1.8 | 1.0 | 5.9 | 4.0 | 2.5 | 1.9 | 5.1 | 5.5 | 3.4 | 4.3 | 17.9 | 13.5 | 7.4 | 6.8 | 5.4 | 10.1 | 4.5 | 8.1 |
| 10 | R | 2.2 | 1.5 | R | 1.6 | 1.4 | 4.7 | 5.7 | 1.4 | 3.1 | 3.7 | 16.9 | 7.0 | 3.3 | 10.3 | 23.5 | 5.6 | 12.8 | 4.5 | 10.8 | 8.0 | 4.5 |
| 11 | L | 1.8 | 1.0 | L | 1.5 | 1.4 | 5.0 | 2.1 | 1.8 | 4.9 | 6.0 | 4.7 | 2.4 | 5.3 | 13.4 | 8.3 | 5.2 | 11.0 | 7.0 | 5.7 | 4.5 | 6.1 |
| 12 | R | 1.8 | 1.1 | R | 1.6 | 1.2 | 2.2 | 3.7 | 2.2 | 4.6 | 3.6 | 3.2 | 2.0 | 3.9 | 8.1 | 10.4 | 7.6 | 10.8 | 5.1 | 6.4 | 4.2 | 8.0 |
| 13 | R | 1.7 | 1.7 | R | 3.5 | 1.2 | 3.5 | 3.0 | 6.6 | 2.0 | 5.9 | 6.4 | 8.3 | 2.5 | 6.1 | 5.4 | 9.2 | 5.0 | 5.4 | 3.0 | 4.3 | 1.7 |
| 14 | R | 1.3 | 1.5 | L | 3.4 | 1.5 | 5.2 | 4.5 | 6.0 | 4.9 | 5.5 | 3.6 | 17.4 | 16.7 | 17.0 | 14.1 | 16.0 | 9.1 | 5.7 | 5.1 | 10.5 | 16.7 |
| 15 | L | 4.3 | 1.2 | L | 2.5 | 3.1 | 8.7 | 4.9 | 6.8 | 9.7 | 29.3 | 12.6 | 6.7 | 46.9 | 11.3 | 15.1 | 9.8 | 23.0 | 7.0 | 7.4 | 3.0 | 12.4 |
| 16 | L | 1.9 | 1.1 | L | 1.6 | 0.9 | 3.5 | 4.3 | 2.5 | 2.6 | 3.7 | 10.1 | 2.7 | 5.0 | 21.1 | 21.4 | 6.9 | 13.7 | 11.1 | 8.3 | 4.5 | 8.6 |
| 17 | L | 2.1 | 1.8 | L | 1.7 | 1.8 | 4.4 | 3.2 | 3.1 | 5.5 | 9.4 | 8.8 | 11.3 | 11.7 | 8.1 | 6.1 | 5.8 | 8.8 | 4.7 | 4.5 | 6.0 | 4.4 |
| 18 | R | 1.6 | 1.6 | R | 1.7 | 2.0 | 5.5 | 2.3 | 5.3 | 3.8 | 5.6 | 9.1 | 18.5 | 12.1 | 11.4 | 8.3 | 12.4 | 8.5 | 3.9 | 8.4 | 4.0 | 5.6 |
| 19 | L | 1.3 | 1.0 | L | 1.6 | 1.8 | 5.2 | 2.0 | 4.5 | 6.3 | 8.6 | 4.5 | 9.2 | 7.0 | 8.7 | 7.5 | 7.3 | 6.5 | 4.6 | 3.8 | 5.6 | 2.6 |
| 20 | L | 2.1 | 1.2 | L | 2.1 | 1.0 | 2.3 | 8.0 | 2.9 | 7.6 | 6.2 | 15.7 | 6.7 | 21.1 | 5.4 | 18.3 | 7.4 | 22.5 | 3.4 | 11.0 | 3.5 | 13.1 |
| 21 | R | 2.4 | 1.1 | R | 1.8 | 1.5 | 3.3 | 3.0 | 4.4 | 3.3 | 3.3 | 1.7 | 2.3 | 2.2 | 7.4 | 7.9 | 10.7 | 9.8 | 4.3 | 3.0 | 4.6 | 4.5 |
| 22 | L | 2.1 | 1.0 | L | 1.3 | 1.2 | 4.3 | 8.0 | 2.5 | 9.0 | 5.4 | 12.6 | 8.3 | 15.4 | 7.4 | 21.0 | 8.3 | 16.7 | 3.5 | 8.4 | 5.9 | 8.2 |
| 23 | L | 1.1 | 1.2 | L | 1.5 | 1.4 | 5.8 | 4.6 | 4.6 | 3.9 | 4.4 | 10.6 | 5.6 | 4.3 | 19.1 | 16.7 | 9.3 | 9.4 | 3.0 | 9.7 | 4.5 | 2.8 |
| 24 | R | 1.3 | 0.8 | R | 1.6 | 1.0 | 3.2 | 5.0 | 2.8 | 1.8 | 3.8 | 1.9 | 3.5 | 3.0 | 7.7 | 18.5 | 6.6 | 6.2 | 3.9 | 1.8 | 3.3 | 4.8 |
| 25 | L | 0.9 | 0.9 | L | 1.5 | 1.0 | 3.6 | 2.4 | 4.6 | 4.1 | 4.3 | 2.8 | 5.7 | 5.4 | 8.3 | 7.6 | 7.7 | 10.4 | 2.3 | 2.1 | 2.8 | 3.5 |
| Max | 4.3 | 4.4 | 4.3 | 4.4 | 8.7 | 9.2 | 6.8 | 20.6 | 29.3 | 18.6 | 18.5 | 46.9 | 28.9 | 23.5 | 16.0 | 23.0 | 11.1 | 16.2 | 10.5 | 16.9 | ||
| Min | 0.9 | 0.8 | 1.3 | 0.9 | 2.1 | 2.0 | 1.4 | 1.8 | 0.9 | 1.7 | 1.8 | 2.2 | 5.4 | 5.4 | 5.1 | 5.0 | 1.3 | 1.8 | 2.8 | 1.7 | ||
| Mean | 2.0 | 1.6 | 2.0 | 1.7 | 4.7 | 4.5 | 3.9 | 5.5 | 7.0 | 7.8 | 7.2 | 11.2 | 11.3 | 12.4 | 8.4 | 11.6 | 4.9 | 6.1 | 4.9 | 7.4 | ||
| SD | 0.8 | 0.8 | 0.8 | 0.9 | 1.6 | 1.9 | 1.6 | 4.1 | 5.4 | 4.8 | 4.3 | 10.9 | 5.7 | 5.7 | 2.6 | 4.9 | 1.9 | 3.5 | 1.8 | 4.3 | ||
| p-value | a: | 0.84158 | v: | 0.604 | b: | 0.049 | w: | 0.150 | c: | 0.454 | x: | 0.081 | d: | 0.013 | y: | 0.310 | e: | 0.458 | z: | 0.122 |
Table 6: The COP transition during trouser-wearing with eyes open was assessed before and after the OT intervention Table 5: The
The COP transition during trouser-wearing with eyes open was assessed before and after the OT intervention (Table 5). The mean single-leg standing time for the FSL (2.0 s) did not change before and after the intervention. That for the SSL was 1.6 s before and 1.7 s after the OT intervention, with no significant difference. Regarding the A/P-COP-max during the trouser-wearing motion, the mean values of the FSL were 4.7% and 3.9% before and after the intervention, respectively, whereas those of the SSL were 4.5% and 5.5%, respectively. The A/P-COP-max in the FSL decreased significantly after the OT intervention compared to before the intervention (p=0.049). However, there was no significant difference in the A/P-COP-max in the SSL. Regarding the M/L- COP-max, the mean values of the FSL were 7.0% and 7.2% before and after the OT intervention, respectively and those of the SSL were 7.8% and 11.2%, respectively. There were no significant differences in the M/L-COP-max between the FSL and SSL before and after the intervention. Regarding the A/P- COP-trajectory, the mean values of the FSL were 11.3%/s and 8.4%/s before and after the intervention, respectively and those of the SSL were 12.4%/s and 11.6%/s, respectively. The A/P-COP-trajectory of the FSL decreased significantly after the OT intervention compared with that before the intervention (p=0.018). However, there was no significant difference in the A/P-COP trajectory of the SSL. Regarding the M/L-COP-trajectory, the mean value of the FSL before and after the OT intervention did not change (4.9%/s); those of the SSL were 6.1%/s and 7.4%/s before and after the OT intervention, respectively. There was no significant difference in the M/L-COP-trajectory between the FSL and SSL before and after the intervention.
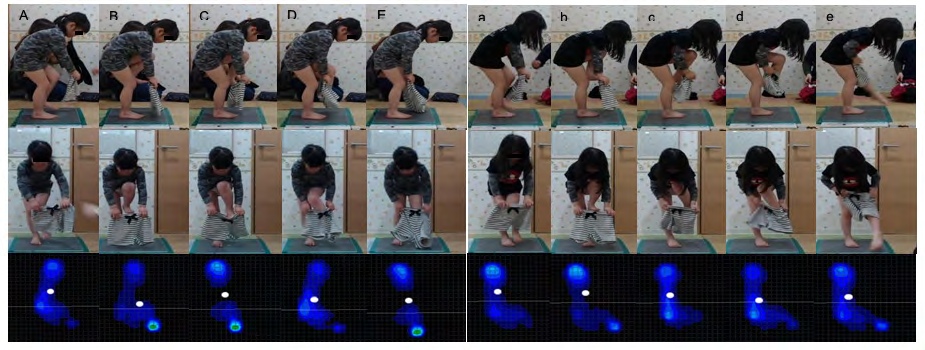
Figure 10: Photographic playback during trouser-wearing motion before and after OT intervention (participant L). The left side indicates the foot of first leg ( from takeoff to landing before OT intervention, and the right side indicates it after OT intervention Top indicates photos from the sagittal plane, middle indicates photos from the frontal plane The bottom indicates the foot pressure distribution and the center of pressure ( of the first support leg ( Dark blue indicates weak pressure, green indicates strong pressure White circles indicate COP ..” and “ indicate when the FL begins to move ..” and “ indicate when the foot of the FL has risen to the waistline of the trousers ..“ and “ indicate the moment when the foot of the FL was inserted into the waist of the trousers ..” and “ indicate the moment when the FL’s foot passes through the hem of the trousers ..“ and “ indicate the moment when the foot of the FL was set on the floor The photographic playback of the trouser-wearing motion of participant L before and after the OT intervention is shown in Figure 10. Comparing “A” and “a” before and after the OT intervention, the characteristics of the motion images were similar. Foot pressure distribution was similar in the COP position, although the pressure at the heel was higher after the intervention. Comparing “B” and “b,” there was greater forward flexion of the trunk after the intervention. Before the intervention, the foot pressure increased in the thumb, and the COP shifted forward. On the other hand, there was less thumb pressure and little COP shift after the intervention compared with before. Comparing “C” and “c,” trunk forward flexion was greater after the OT intervention. Before the intervention, the foot pressure increased at the heel, in addition to that of the thumb, and the COP moved backward. After the intervention, the thumb pressure decreased, and the COP moved slightly forward. In the comparison between “D” and “d,” before the intervention, the trunk was becoming vertically extended, whereas there was no change after the intervention. Before the intervention, the position of the trousers was fixed, and the FL passed through the hem. The foot pressure at this point increased on the fifth midfoot side, and the COP moved forward again. After the OT intervention, the participant pulled up the trousers with both upper limbs while passing the FL through the trousers. In this case, the foot pressure increased on the 5th metatarsal side, and the COP moved forward similarly before the intervention. In the comparison between “E” and “e,” the FL foot did not pass through the trousers before the intervention, and the FL foot was on the floor. The foot pressure of the FSL was high at the toe and the heel, and no ground contact was observed on the fifth metatarsal side. However, after the intervention, the FL passed through the trouser leg opening, while the trousers were pulled up to the waist, the foot pressure of the FSL weakened on the 5th metatarsal side, and the COP moved backward.
Discussion
The one-legged standing time was significantly shorter for the right leg after than before the intervention, but there was no significant difference for the left leg. The participants with the shortest one-legged standing time were N (left leg, 3.0 s) before the intervention and Y (left leg, 1.6 s) after the intervention. In addition, two participants refused to stand on one leg before the intervention, and another one refused after the intervention. There was no significant difference in the COP maximum amplitude and the total trajectory length during one-legged standing before and after the OT intervention. A previous study found that muscle tone in the trunk axis during static standing is sensitive and requires dynamic coordination [37]. Thirty-two children with ASD without intellectual disability (IQ ≥ 70) and 32 healthy controls were compared; a standardized age-specific neurological examination according to Touwen was used to detect the presence of MNDs. A study on children with ASD found that 26 (81.3%) had simple MND and 5 (15.6%) had complex MND. MNDs included posture and muscle tone, 4 (12.5%); coordination and balance, 11 (34.4%); fine motor dysfunction, 9 (28.1%); associated movements, 19 (59.4%); and sensory deficits 7 (21.9%) [7]. In another study, simple MND was found in 24 (21%) children, complex MND in 83 (74%) children, mild dysfunction in posture and muscle tone regulation in 87%, mild coordination problems in mild fine manipulative disability in 75%, excess of associated movements in 45%, and mild sensory dysfunction in 15% [8]. Although there are differences in the prevalence of MNDs among the studies, the postural and muscle tone problems associated with ASD are evident.
Another study examining passive muscle tone in the upper and lower extremities and body axis using dangling and extensibility found a discordant tonic typology, with a tonic component in the trunk muscles and proximal muscles of the lower extremities and a relaxed component in the proximal and distal muscles of the ankle and upper extremities (wrist and shoulder) [38]. Furthermore, hypotonia was reported as an early marker for ASD diagnosis [39]. Upon standing on one leg, many children with ASD lost their balance starting from the lower trunk and pelvic area. Although the tonic and lax components of the trunk and the lower limb muscles of the participants in this study were not clear, the presence of postural and muscle tone problems was evident. Another report investigated the relationship between balance control and the diagnostic and symptom severity indices of ASD in children with ASD and their peers with typical development (TD) [40]. They found that balance deficits in ASD were not associated with symptom severity, and that in TDs, the duration of one-legged standing increased with increasing age [40]. The anterior–posterior and lateral components of COP during one-legged standing were smaller in participants aged 8–12 years than in those aged 4–7 years [41].
The sensory processing results differed between children with ASD and those with TD [30, 31]. Deficits in the regulation of incoming sensory input have been widely reported as features of autism [42, 43, 44, 45, 46, 47]. The results of this study similarly showed that many participants had a definite difference in each item of sensory sensitivity, with the majority showing a difference in visual/auditory sensitivity. A study examining the maintenance of upright posture in children with ASD and TD found that the sway area of COP was significantly greater in all test conditions in which the afferent input of ASD children varied [48]. This report suggested that children with ASD have deficits in the integration of visual, vestibular, and somatosensory inputs to maintain posture. Another study noted a delay in the development of postural stability in ASD compared with TD [49]. They suggested that it is difficult for children with ASD to maintain posture under conditions that require multiple sensory systems, including somatosensory systems. In a study on young adults with ASD, postural impairment under conditions where only visual information was inaccurate was not observed; however, there was impairment under conditions where both visual and intrinsic sensory information were inaccurate [50]. Thus, ASD impairs the integration of multiple sensory species, making it difficult to maintain posture in a standing position. A resting-standing study compared the effects of SI therapy in children with ASD and TD and found an immediate effect of SI therapy, with a decrease in COP after the intervention [51]. One-legged standing, the subject of our study, is more challenging than resting standing. Therefore, we speculate that the 60-minute OT intervention could not adjust sensory processing sufficiently to improve the participants’ one- legged standing time.
Furthermore, all participants performed the trouser- wearing motion in the standing position before and after the OT intervention. The mean times to stand on one leg during the trouser-wearing operation were 2.0 s for the FSL and 1.6 and 1.7 s for the SSL, respectively, with no significant difference. This finding suggested that the reason for the difficulty in the trouser-wearing motion was not due to the time spent standing on one leg. In contrast, the A/P-COP-max and the total trajectory length of the FSL while the FL was put through the trousers significantly decreased after the OT intervention. However, there was no significant difference in the A/P-COP- max and the total trajectory length of the SSL while the SL was put through the trousers. These results suggest that the OT intervention improved the unilateral balance ability of the SL until the FL was put through the trousers. Several factors contributed to this improvement. First, the participants found it easier to maintain a forward bend of the trunk while standing on one leg. Next, the foot of the FL no longer got caught in the hem of the trousers. In addition, the participants improved their grasp of the waist edge of the trousers during the trouser -wearing motion.
Figure 2 shows that the forward-trunk bending became easier after the OT intervention. The participant maintained the forward-trunk bending until the FL was lifted to the waistline of the trousers. The participant was also able to hold the forward-trunk flexion when passing the legs through the trousers. During this time, the legs were placed through the trousers by extending the FL while pulling the trousers with both hands. The participant could firmly grasp the waist end of the trousers with both hands. Although these observations are qualitative in nature and cannot be expressed numerically, our findings suggest that the OT intervention could improve posture, muscle tone, and the upper and lower limb coordination [24, 25]. We speculated that the result was manifested as a decrease in the A/P- COP-max and A/P-COP-tra of the FSL until the FL passed through the trousers. In other words, these observations can be attributed to the task specificity caused by the trouser- wearing behavior, and there is a possibility that the effects of the OT intervention for ASD can be applied to specific daily life activities.
Limitations of the Study
Since this was a cross-sectional study, the participants’ proficiency in standing trouser-wearing motions was not assessed. Thus, although an immediate effect was observed following the OT intervention, it may not be an ongoing effect. Therefore, it is necessary to evaluate the proficiency of trouser-wearing motions of children with ASD in long- term studies. However, owing to our small sample size, comparisons between ages could not be made.
Conclusion
The current study was to investigate whether play-based occupational therapy improves the motions of children with autism spectrum disorder (ASD), who have difficulty putting on trousers in a standing position. The results suggest that the maximum excursion and total trajectory of COP in the anterior–posterior direction of the first support leg decreased significantly after the intervention compared to that before the intervention. These findings are attributed to the task-specificity of the trouser-wearing behavior and are speculated to be the effects of OT intervention for ASD on activities of daily living.
Acknowledgements
The authors thank Dr. Reiko Tsuchida, President the Japanese Academy of Sensory Integration for her valuable suggestions to this study. We also thank the staff of the Kanon Co. and the parents of the participants for their excellent assistance. Parts of this paper were presented at the 29th Tohoku Occupational Therapy Conference & Expo in Yamagata, Japan, the 53rd Japanese Occupational Therapy Conference & Expo in Fukuoka, Japan.
References
-
Lord C, Elsabbagh M, Baird G, Veenstra Vanderweele J (2018) Autism spectrum disorder. Lancet 392(10146): 508-520.
-
Denda K (2017) Understanding individualities in autism spectrum disorder. Jpn J Psychosom Med 57: 19-26.
-
American Psychiatric Association (2013) Diagnostic and statistical manual of mental disorders (DSM- 5). 5th (Edn.), Washington, DC, American Psychiatric Association Publishing, pp: 429-457.
-
Miyakawa J (2014) DMS-5, revised diagnostic criteria by American Psychiatric Association: neurodevelopmental disorders, intellectual disabilities, and autism spectrum disorder. J Sch Educ Sugiyama Jogakuen Univ 7: 65-78.
-
Stein DJ, Szatmari P, Gaebel W, Berk M, Vieta E, et, al. (2020) Mental, behavioral and neurodevelopmental disorders in the ICD-11: an international perspective on key changes and controversies. BMC Med 18(1): 21.
-
Saito M, Hirota T, Sakamoto Y, Adachi M, Takahashi M, et, al. (2020) Prevalence and cumulative incidence of autism spectrum disorders and the patterns of co-occurring neurodevelopmental disorders in a total population sample of 5 year old children. Mol Autism 11(1): 35.
-
Tripi G, Roux S, Carotenuto M, Bonnet Brilhault F, Roccella M (2018) Minor neurological dysfunctions (MNDs) in autistic children without intellectual disability. J Clin Med 7(4): 79.
-
De Jong M, Punt M, De Groot E, Minderaa RB, Hadders Algra M (2011) Minor neurological dysfunction in children with autism spectrum disorder. Dev Med Child Neurol 53(7): 641-646.
-
Ament K, Mejia A, Buhlman R, Erklin S, Caffo B, et al. (2015) Evidence for specificity of motor impairments in catching and balance in children with autism. J Autism Dev Disord 45(3): 742-751.
-
Mari M, Castiello U, Marks D, Marraffa C, Prior M (2003) The reach-to-grasp movement in children with autism spectrum disorder. Philos Trans R Soc Lond B Biol Sci 358(1430): 393-403.
-
Nayate A, Bradshaw JL, Rinehart NJ (2005) Autism and Asperger’s disorder: are they movement disorders involving the cerebellum and/or basal ganglia? Brain Res Bull 67(4): 327-334.
-
Whitney ER, Kemper TL, Rosene DL, Bauman ML, Blatt GJ (2009) Density of cerebellar basket and stellate cells in autism: evidence for a late developmental loss of Purkinje cells. J Neurosci Res 87(10): 2245-2254.
-
D Mello AM, Stoodley CJ (2015) Cerebro-cerebellar circuits in autism spectrum disorder. Front Neurosci 9: 408.
-
Kelly E, Meng F, Fujita H, Morgado F, Kazemi Y, et al. (2020) Regulation of autism relevant behaviors by cerebellar prefrontal cortical circuits. Nat Neurosci 23(9): 1102-1110.
-
Dadalko O, Travers BG (2018) Evidence for brainstem contributions to autism spectrum disorders. Front Integr Neurosci 12: 47.
-
Hanaie R, Mohri I, Kagitani Shimono K, Tachibana M, Matsuzaki J, et al. (2016) White matter volume in the brainstem and inferior parietal lobule is related to motor performance in children with autism spectrum disorder: A voxel-based morphometry study. Autism Res 9(9): 981-992.
-
Frazier TW, Keshavan MS, Minshew NJ, Hardan AY (2012) A two-year longitudinal MRI study of the corpus callosum in autism. J Autism Dev Disord 42(11): 2312- 2322.
-
Rinehart NJ, Tonge BJ, Bradshaw JL, Iansek R, Enticott PG, et al. (2006) Movement-related potentials in high- functioning autism and Asperger’s disorder. Dev Med Child Neurol 48(4): 272-277.
-
Fournier KA, Kimberg CI, Radonovich KJ, Tillman MD, Chow JW, et al. (2010) Decreased static and dynamic postural control in children with autism spectrum disorders. Gait Posture 32(1): 6-9.
-
Fournier KA , Shinichi Amano, Radonovich KJ, Bleser TM, Hass CJ (2014) Decreased dynamical complexity during quiet stance in children with autism spectrum disorders. Gait Posture 39(1): 420-3.
-
Minshew NJ, Sung KB, Jones BL, Furman JM (2004) Underdevelopment of the postural control system in autism. Neurology 63(11): 2056-2061.
-
Cheldavi H, Shakerian S, Boshehri NS, Zarghami M (2014) The effects of balance training intervention on postural control of children with autism spectrum disorder: Role of sensory information. Res Autism Spectr Disord 8(1): 8-14.
-
Casey AF, Quenneville Himbeault G, Normore A, Davis H, Martell SG (2015) A therapeutic skating intervention for children with autism spectrum disorder. Pediatr Phys Ther 27(2): 170-177.
-
Nuntanee S, Daranee S (2019) Effect of motorized elephant-assisted therapy program on balance control of children with autism spectrum disorder. Occup Ther Int 2019: 5914807.
-
Hassani F, Shahrbanian S, Shahidi SH, Sheikh M (2020) Playing games can improve physical performance in children with autism. Int J Dev Disabil 11: 1-8.
-
Provost B, Crowe TK, Osbourn PL, McClain C, Skipper BJ (2010) Mealtime behaviors of preschool children: comparison of children with autism spectrum disorder and children with typical development. Phys Occup Ther Pediatr 30(3): 220-233.
-
Nadon G, Feldman DE, Dunn W, Gisel E (2011) Association of sensory processing and eating problems in children with autism spectrum disorders. Autism Res Treat 2011: 541926.
-
Chi IJ, Lin LY (2020) Exploring the performance of self- care and visual perception in preschool children with autism spectrum disorder (ASD). Am J Occup Ther 74 (4S1): 7411505164p1-7411505164p1.
-
Boop C, Cahill SM, Davis C, Dorsey J, Gibbs V, et al. (2020) Occupational therapy practice framework: Domain and process fourth edition. Am J Occup Ther 74(S2): 1-85.
-
Tomchek SD, Dunn W (2007) Sensory processing in children with and without autism: a comparative study using the short sensory profile. Am J Occup Ther 61(2): 190-200.
-
Tani I, Ito H, Hirashima T, Iwanaga R, Hagiwara T, et al. (2015) Standardization of the Japanese Version of the Short Sensory Profile: reliability and validity. Clin Psychiatry 57(6): 419-429.
-
Fidler GS, Velde BP (1999) Activities: reality and symbol. 1st (Edn.), Slack Incorporated, West Deptford, New Jersey, USA, pp: 61-79.
-
Tickle Degnen L, Coster W (1995) Therapeutic interaction and the management of challenge during the beginning minutes of sensory integration treatment. OTJR Occup Particip Health 15(2): 122-141.
-
Dunkerley E, Tickle Degnen L, Coster WJ (1997) Therapist-child interaction in the middle minutes of sensory integration treatment. Am J Occup Ther 51(10): 799-805.
-
Pfeiffer BA, Koenig K, Kinnealey M, Sheppard M, Henderson L (2011) Effectiveness of sensory integration interventions in children with autism spectrum disorders: a pilot study. Am J Occup Ther 65(1): 76-85.
-
Matsuda N, Kato K, Ito K, Morikawa A, Suzuki K, et al. (2021) Differences in the motion of typically developing children aged 4-6 years, putting on trousers in a standing position. Yamagata J Health Sci. 25. On-Line First December 24 2021.
-
Gurfinkel V, Cacciatore TW, Cordo P, Horak F, Nutt J, et al. (2006) Postural muscle tone in the body axis of healthy humans. J Neurophysiol 96(5): 2678-2687.
-
Paquet Aude, Olliac B, Golse B, Vaivre Douret L (2017) Evaluation of neuromuscular tone phenotypes in children with autism spectrum disorder: an exploratory study. Neurophysiol Clin 47(4): 261-268.
-
Serdarevic F, Ghassabian A, van Batenburg-Eddes T, White T, Blanken LME, et al. (2017) Infant muscle tone and childhood autistic traits: A longitudinal study in the general population. Autism Res 10(5): 757-768.
-
Graham SA, Abbott AE, Nair A, Lincoln AJ, Müller RA, et al. (2015) The influence of task difficulty and participant age on balance control in ASD. J Autism Dev Disord 45(5): 1419-1427.
-
Zumbrunn T, MacWilliams BA, Johnson BA (2011) Evaluation of a single leg stance balance test in children. Gait Posture 34(2): 174-177.
-
Ayres AJ (1980) Southern California sensory integration tests manual. Los Angeles, Western Psychological Services.
-
Adrien JL, Lenoir P, Martineau J, Perrot A, Hameury L, et al. (1993) Blind ratings of early symptoms of autism based upon family home movies. J Am Acad Child Adolesc Psychiatry 32(3): 617-626.
-
Adrien JL, Ornitz E, Barthelemy C, Sauvage D, Lelord G (1987) The presence or absence of certain behaviors associated with infantile autism in severely retarded autistic and nonautistic retarded children and very young normal children. J Autism Dev Disord 17(3): 407- 416.
-
Baranek GT (1999) Autism during infancy: a retrospective video analysis of sensory-motor and social behaviors at 9-12 months of age. J Autism Dev Disord 29(3): 213-224.
-
Kientz MA, Dunn W (1997) A comparison of the performance of children with and without autism on the Sensory Profile. Am J Occup Ther 51(7): 530-537.
-
Ornitz EM, Lane SJ, Sugiyama T, de Traversay J (1993) Startle modulation studies in autism. J Autism Dev Disord 23(4): 619-637.
-
Osterling J, Dawson G (1994) Early recognition of children with autism: a study of first birthday home videotapes. J Autism Dev Disord 24(3): 247-257.
-
Molloy CA, Dietrich KN, Bhattacharya A (2003) Postural stability in children with autism spectrum disorder. J Autism Dev Disord 33(6): 643-652.
-
Gabis LV, Shaham M, Leon Attia O, Shefer S, Rosenan R, et al. (2021) The Weak Link: Hypotonia in Infancy and Autism Early Identification. Front Neurol 12: 612674.
-
Smoot Reinert SS, Jackson K, Bigelow K (2015) Using posturography to examine the immediate effects of vestibular therapy for children with autism spectrum disorders: A feasibility study. Phys Occup Ther Pediatr 35(4): 365-380.
- Electrolyte Considerations for Athletes
- Comprehensive Rehabilitation in Adults with Diabetic Peripheral Neuropathy: A Literature Review on Frequency, Intensity, and Duration Parameters
- Exercise Duration and Its Association with ADHD Symptom Severity in Children and Adolescents: A Parent-Reported Survey Study
- Adaptation of the Adult Neurophysiology of Pain Questionnaire for Use in Pediatrics
- A Non-Pharmacological Multidisciplinary Pain Program within a Hospital Wellness Program: A Mixed Methods Study
- The Effect of Frenkel's Exercise with PNF on Functional Reach in Stroke Survivors: A Randomized Control Trial