The Current EBM for Physiotherapy Management of Tetraplegia Hand: Systematic Review of Literature
Introduction: Cervical spinal cord injury patients have loss of hand function, which leads to high dependence degree in everyday activities (ADL). Rehabilitation treatment aimed to hand recovery plays a central role in physiotherapy approach to this medical condition. The aim of this research, if possible, was to find studies establish best EBM practice about conservative treatments of tetraplegic hand. Materials and Methods: A systematic review search was conducted through PubMed, Ebsco, CINAHL Plus with Full Text, Literary Reference Center, MEDLINE. Inclusion criteria were: RCTs published in the last 10 years, regarding physiotherapy management of tetraplegia hand. Results: Eight studies were selected and subdivided into four subgroups: Comparison of conventional therapy with Rejoyce therapy, Comparison of FES therapy with various rehabilitation interventions, Efficacy of tDCS therapy and Study of acute intermittent hypoxia. Discussion: To date it is not possible to establish a gold standard for hand rehabilitation in tetraplegic patients; interventions were different, depending on rehabilitation plan and outcome measured. Several interesting proposal, however, we carried out. Further research is needed to better define a structured and standardized intervention.
Gianluca Ciardi*1 and Marchesi Elia2
Introduction
Spinal Cord Injury (SCI) is a complex medical and life- threatening condition, that causes temporary or permanent changes in the normal motor, sensory and autonomic functions of the spinal cord [1, 2]. The global estimate of SCI incidence is 40-80 new cases/ million inhabitants per year, so every year 250,000 to 500,000 people suffer a spinal cord injury [3]. To get an idea, the 2012 Canadian prevalence study is very interesting; it describes an overall SCI prevalence rate (traumatic and non-traumatic) of 2525 cases per million population or (85,000 people in 2010). Age-related prevalence in Canada indicated that traumatic SCI was prevalent in younger population, while non traumatic- SCI was prevalent in older one [4]. Much of tetraplegic rehabilitation is aimed to motor recovery of hand function; the management varies according to level of injury, and whether it is complete or incomplete, leading to a wide variety of specific physiotherapy management [5]. Loss of hand function is one of the most important disabilities for patients with a cervical spinal cord injury [5]; impairment of motor and sensory functions in the arms and hands results in: loss of joint mobility, grip strength, movement coordination and proprioception. Due to these motor impairments, these patients completely change the way they perform activities of daily living [3]. Several types of interventions are available in literature, such as orthoses, tendon transfers, functional electrostimulation (FES) and creation of a functional hand with a tenodesis [6].
Among conservative approaches performed by physiotherapists, to date, there are several attempts to create a “functional hand”, through a structured shortening of the flexor muscles of fingers and thumb [7]. The prehensile function, in these cases, must be supported by the presence of the radial extensor of the carpus or by an orthosis which, stabilising the wrist, allows the use of the passive functional hand through the activity of biceps [7]. Nevertheless, scientific literature does not recognise an evidence-based guideline for the management of the hand of tetraplegic patients. The aim of this research was, if possible, to find studies in literature to describe treatments actually known.
Aims
The objective of this study was to verify the presence of scientific evidence that can define a gold standard rehabilitation model.
Methods
A systematic review of literature was carried out; formulation of clinical query was carried out through PICO model: P = Population of individuals with traumatic and nontraumatic cervical spinal cord injuries I = Interventions designed for hand rehabilitation C = Inactive control arm/non-specific hand rehabilitation interventions O = Outcome used in studies found Literature search was conducted using the online scientific databases PubMed and Ebsco, CINAHL Plus with Full Text, Literary Reference Center, MEDLINE. All studies included were evaluated by Pedro score, to assess methodology quality.
Inclusion and Exclusion Criteria
The studies selected for this article were only studies randomized controlled trials involving patients with traumatic and non-traumatic cervical spinal cord injury with problems in hand function, written in Italian and English language, last ten years published. Animal studies, publications before 2010 and other than RCTS were excluded.
Results
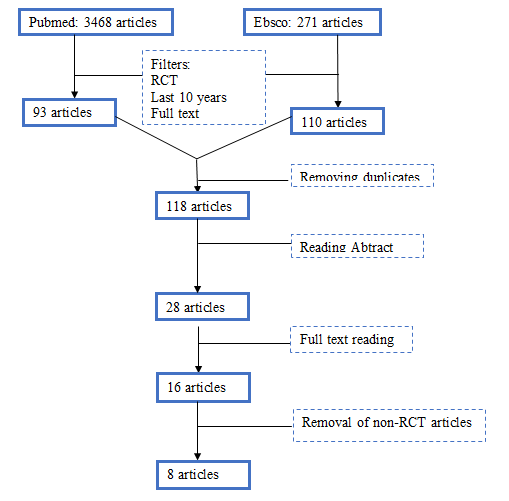
Following search strategy a total of 3739 articles were found. An initial selection was possible thanks to the automatic filters contained in both the PubMed and Ebsco databases, set in accordance with the inclusion and exclusion criteria, which made it possible to select 93 articles from PubMed and 110 articles from Ebsco. After removal of duplicates, 118 articles were excluded, and after reading the title and abstract 28 articles were selected, which later became 16 by full text reading. Of these 9 papers were removed, because they were not RCTs, so to conclude the search yielded 8 articles.
All included studies had Pedro score from 6/10 to 8/10, except Hofmann (10) paper (3/10).
Comparison of conventional therapy with Rejoyce therapy one of included study [8] was performed on a population of 13 individuals with C5-C7 tetraplegia for at least 9 months, divided into 2 groups by randomization.
The characteristics of the intervention were as follow:
- Group 1 performed 6 weeks (5 hrs/wk) of an exercise programme followed by a 1-month washout period and 6 weeks of exercise therapy using the ReJoyce (Rehabilitation Joystick for Computerized Exercise).
- Control group received 6 weeks of ReJoyce exercise, 1 month washout and then 6 weeks of exercise. Difficulty of exercises was tailored to the ability of each participant each sessions was divided into three 20-minute segments, one for strength training, the second for accuracy training and third one for TES (therapeutic electrical stimulation).
Rejoyce Exercise Programme
During ReJoyce sessions, participants played computer games on workstation, with a target difficulty depending on patient’s ability.
The main outcome used was the ARAT (Action Research Arm Test) and as a second one the ReJoyce Automated Manual Function Test (RAHFT) was examined; it evaluates functional range of motion, functional activities and limb positioning activities.
The study showed that ReJoyce workstation + FES was more effective than the exercise programme + TES, in fact, after week 6, improvements in ARAT were 4.0% ± 9.6% (group 1 with exercise programme) and 13.0% ± 9.8% (group 2 ReJoyce therapy). Corresponding improvements in RAHFT were 3.3% ± 10.2% (Group 1 exercise programme) and 16.9% ± 8.6% (Group 2 ReJoyce Therapy).
Comparison of FES therapy with various rehabilitation interventions Harvey’s [9] and Popovic’s (11) studied SCI patients in the first 6 months by diagnosis; Harvey studied 70 patients, with complete or incomplete C2-T1 spinal injury, Popovic 22 ones. In contrast, Hoffman’s study [10] observed a sample of 24 patients, with spinal injury C7 or higher for at least one year. In the first study [9] one group performed occupational therapy sessions aimed to hand recovery, while experimental group added FES treatment. Study [10] was a cross over RCT, which performed 4 types of intervention at different times: FES use + unimanual training, FES use + bimanual training, SS (somatosensory stimulation) use + unimanual training, SS use + bimanual training. Follow up was different: studies [9] and [11] evaluated patients at 8 weeks, while study [10] at three weeks after intervention. Popovic’s [11] and Hoffman’s [10] studies indicate that the use of FES led to improvements in the outcomes measured while Harvey’s study [9] found no differences between the control group and the intervention group.
Effectiveness of tDCS therapy (Transcranial direct current stimulation) RCTs [12, 13, 14] involved a sample of 8 and 24 patients respectively, diagnosed with cervical SCI, treated with TDCS. Yozbatiran [12] and Potter-Baker [13] treated both groups with a rehabilitation protocol and tDCS, applied in the control group in sham mode; in the study of [12], in addition, intervention was carried out R-AAT (robot-assisted arm training). In study [14] patients are divided into three groups: tDCS, TENS and vibration.
Follow up was even at the end of treatment [12, 13, 14]. All studies show a greater but statistically insignificant improvement in outcomes in the groups treated with tDCS.
Acute intermittent hypoxia
Trumbower [15] tested the effects of acute intermittent hypoxia (AIH) combined exercises to improve dexterity, function and maximal hand opening in people with chronic incomplete cervical spinal cord injury.
Six participants completed the study by receiving 5 consecutive days of AIH episodes (15 per day) or sham hypoxic episodes, followed by 20 repetitions of hand opening training. Outcome measured was Box and Block Test and Jebsen-Taylor hand function test. The comparison of the outcomes showed that patients treated with AIH had an overall improvement in both the Box and Block Test and the Jebsen-Taylor hand function test, compared to patients treated with sham AIH episodes, as well as an increase in hand opening.
Discussion
To date, scientific literature shows a severe lack of good quality articles about hand rehabilitation in tetraplegic patients. Rehabilitation interventions tested are very different, and are therefore difficult to compare. In addition, as pointed out by Trumbower [15] Yozbatiran [12] another problem encountered, due to the fragility of these patients, was the lost during study period, leading to a massive decrease in the study sample as is also pointed out by Popovic [11].
Strengths and Weaknesses of this Review
The strengths of this article were: examination of RCTs, extremely significant in the literature, very recent (last ten years), with extensive profiling, an high general value of the PEDro scale and reviewing development according to PRISMA method. Weak points, on the other hand, were small sample size, and different outcome used, even in studies that carried out rehabilitation with the same treatment, making comparison imppssible.
Comparison of Conventional Therapy with Rejoyce Therapy
Rehabilitation with the Rejoyce workstation appears to be a valid therapy for improving dexterity of the upper extremity and hand, as described in Kowalczewski’s study [8], and in agreement with Prochazka’s previous study [16]; the latter conducted an RCT comparing rejoyce with an exercise program. At the sixth week of intervention the improvements in ARAT scores were 4.0% ± 9.6% (group 1 with exercise programme) and 13.0% ± 9.8% (group 2 ReJoyce therapy) while the corresponding improvements in RAHFT were 3.3% ± 10.2% (group 1 - exercise) and 16.9% ± 8.6% (group 2 ReJoyce). However, device cost is critical to perform this rehabilitation intervention.
FES Therapy
Rehabilitation by FES was already present in literature, but no accordance to express the improvements was reached; Harvey’s study [9] concluded that addition of FES therapy to an intensive rehabilitation programme on patient’s hand did not induce significant improvements compared to the physiotherapy alone; in fact intervention group which went from m-ARAT value of 24.8 to one of 38.7, while the control group from a 21, 2 to 33.4; Popovic [11] and Hoffman [10] instead, indicated that FES led to significant statistical improvements in the functionality of hand, with a consequent improvement in the patient’s autonomy. Popovic [11] showed an improvement in the FIM from 8 to 17.8 points in the control group and from 8.1 to 28.2 in the intervention group, SCIM scale went from 3.3 to 6.4 in the control group and a from 1.9 to 12.1 in the intervention group. Various articles supports advantages of this therapy, but in relation to a therapy with BCI (brain computer interface) as in the studies of Osuagwu [17] and Colachis [18], also in the study of Kowalczewski [8] rejoyce rehabilitation was integrated with an FES therapy.
This leads to the assumption that the results of this therapy are greater in conjunction with other therapies and not as only rehabilitation treatment.
Efficacy tDCS Therapy
About tDCS therapy, studies agreed that it had a positive effect when used in conjunction with targeted training of the patient’s hand in comparison to a basic treatment, with major improvements in increasing patient’s hand dexterity.
Improvements occurred in outcome that measured the speed of execution of a particular task as the JTHFT and the NHPT, unfortunately, as highlighted by Yozbatiran [12] these improvements were statistically insignificant, and that future studies with a larger sample population will be needed to better investigate this therapy. Also intervention was always in correlation with physiotherapy and occupational treatment. In literature, no study supports the argument that tDCS has positive effects on hand’s motor skills, such established by Reis 2009 study [19]. Various studies also indicated that tDCS has a targeted effect on modulation of motor cortex excitability, which leads to an improvement in muscle activation and coordination [20, 21, 22].
Effects of Acute Intermittent Hypoxia
Acute intermittent hypoxia therapy [15] seems to give positive results with regard to hand rehabilitation, this intervention is of recent introduction and there is no EBM evidence to support it; studies by Hayes [23] and Navarrete- Opazo [24] which focus on gait rehabilitation in chronic spinal injuries, agreed with improvements in terms of speed and resistance to effort. This is undoubtedly a very promising therapy, and it’s needed to study in depth in the coming years, because results of low literature present and small number of examined patients do not grant it a definitive validation (Table 1).
Intervention Author, year and title of articles Comparison of conventional therapy with Rejoyce therapy 2011, J. Kowalczewski et al., In-Home Tele-Rehabilitation Improves Tetraplegic Hand Function (8) Comparison of FES therapy with various rehabilitation interventions
- 2016, L. Harvey et al., Early intensive hand rehabilitation is not more effective than usual care plus one-to-one hand therapy in people with sub-acute spinal cord injury (‘Hands On’): a randomised trial (9)
- 2013, L. Hoffman et al., Effects of Practice Combined with Somatosensory or Motor Stimulation on Hand Function in Persons with Spinal Cord Injury (10)
- 2011, M. Popovic et al., Functional Electrical Stimulation Therapy of Voluntary Grasping Versus Only Conventional Rehabilitation for Patients With Subacute Incomplete Tetraplegia: A Randomized Clinical Trial (11)
- 2016, N. Yozbatiran et al., Transcranial direct current stimulation (tDCS) of the primary motor cortex and robot-assisted arm training in chronic incomplete cervical spinal cord injury: A proof of concept sham-randomized clinical study (12)
- 2018, K. Potter-Baker et al., Transcranial direct current stimulation (tDCS) Paired with massed practice training to promote adaptive plasticity and motor recovery in chronic incomplete tetraplegia: a pilot study (13)
- 2015, J. Gomes-Osman et al., Cortical vs. afferent stimulation as an adjunct to functional task practice training: A randomized, comparative pilot study in people with cervical spinal cord injury (14)
- Efficacy tDCS therapy (Transcranial direct current stimulation)
- Acute intermittent hypoxia study
- •
- 2017, R. Trumbower et al., Effects of acute intermittent hypoxia on hand use after spinal cord trauma (15)
Table 1: synopsis and reference of included articles.
Conclusions
Hand rehabilitation for tetraplegia patients has not a gold standard in literature, due to the difficulty in finding patients with this condition and the variety of clinical pictures. Various therapeutic proposals seem to give positive results, as in the case of therapy with Rejoice, and it will certainly be important to continue to study this technique in order to increase the literature on the subject. Acute intermittent hypoxia was a promising treatment, but it is necessary to study this technique in more depth, and increase the literature to understand its effectiveness in long-term rehabilitation projects. Regarding FES therapy conflicting evidence has emerged, but it is clear that improvements in the patient’s hand function were greater when FES and exercises were combined. As for tDCS, the present study shows a positive finding, but it needs more standardization for outcome measures, in order to obtain more significant results.
References
-
Fakhoury M (2015) Spinal cord injury: Overview of experimental approaches used to restore locomotor activity. Rev Neurosci 26(4): 397-405.
-
Ferro S, Cecconi L, Bonavita J, Pagliacci MC, Biggeri A, et al. (2017) Incidence of traumatic spinal cord injury in Italy during 2013-2014: A population based study. Spinal Cord (55): 1103-1107.
-
WHO (2013) International perspectives on spinal cord injury.
-
Noonan VK, Fingas M, Farry A, Baxter D, Singh A, et al. (2012)Incidence and prevalence of spinal cord injury in Canada: A national perspective. Neuroepidemiology 38(4): 219-226.
-
Lamb DW, Chan KM (1983) Surgical reconstruction of the upper limb in traumatic tetraplegia. A review of 41 patients. J Bone Jt Surg Ser B 65(3): 291-298.
-
Land NE, Odding E, Duivenvoorden HJ, Bergen MP, Stam HJ (2004) Tetraplegia Hand Activity Questionnaire (THAQ): The development, assessment of arm-hand function related activities in tetraplegic patients with a spinal cord injury. Spinal Cord 42(5): 294-301.
-
Valsecchi L, Ruth J, Cassinis A (2000) Upper limb positioning and functional hand. A CNOPUS guideline 1-13.
-
Kowalczewski J, Chong SL, Galea M, Prochazka A (2011) In home tele rehabilitation improves tetraplegic hand function. Neurorehabil Neural Repair 25(5): 412-422.
-
Harvey LA, Dunlop SA, Churilov L, Galea MP, Hurley M, et al. (2016) Early intensive hand rehabilitation is not more effective than usual care plus one to one hand therapy in people with subacute spinal cord injury (‘Hands On’): A randomised trial. J Physiother 62(2): 88-95.
-
Hoffman L, Field Fote E (2013) Effects of practice combined with somatosensory or motor stimulation on hand function in persons with spinal Cord Injury. Top Spinal Cord Inj Rehabil 19(4): 288-299.
-
Popovic MR, Kapadia N, Zivanovic V, Furlan JC, Craven BC (2011) McGillivray C. Functional electrical stimulation therapy of voluntary grasping versus only conventional rehabilitation for patients with subacute incomplete tetraplegia: A randomized clinical trial. Neurorehabil Neural Repair 25(5): 433-442.
-
Yozbatiran N, Keser Z, Davis M, Stampas A, O Malley MK, et al. (2016) Transcranial direct current stimulation (tDCS) of the primary motor cortex and robot assisted arm training in chronic incomplete cervical spinal cord injury: A proof of concept sham-randomized clinical study. NeuroRehabilitation 39(3): 401411.
-
Potter Baker KA, Janini DP, Lin YL, Sankarasubramanian V, Cunningham DA, et al. (2018) Transcranial direct current stimulation (tDCS) paired with massed practice training to promote adaptive plasticity and motor recovery in chronic incomplete tetraplegia: A pilot study. J Spinal Cord Med [Internet 41(5): 503-517.
-
Gomes-Osman J, Field Fote EC (2015) Cortical vs. afferent stimulation as an adjunct to functional task practice training: A randomized, comparative pilot study in people with cervical spinal cord injury. Clin Rehabil 29(8): 771-782.
-
Trumbower RD, Hayes HB, Mitchell GS, Wolf SL, Stahl VA (2017) Effects of acute intermittent hypoxia on hand use after spinal cord trauma: A preliminary study. Neurology 89(18): 1904-1907.
-
Prochazka A, Kowalczewski J (2015) A fully automated, quantitative test of upper limb function. J Mot Behav 47(1): 19-28.
-
Osuagwu BCA, Wallace L, Fraser M, Vuckovic A (2016) Rehabilitation of hand in subacute tetraplegic patients based on brain computer interface and functional electrical stimulation: A randomised pilot study. J Neural Eng 13(6): 0650002.
-
Colachis SC, Bockbrader MA, Zhang M, Friedenberg DA, Annetta NV, et al. (2018) Dexterous control of seven functional hand movements using cortically controlled transcutaneous muscle stimulation in a person with tetraplegia. Front Neurosci 12: 1-14.
-
Reis J, Schambra HM, Cohen LG, Buch ER, Fritsch B, et al. (2009) Noninvasive cortical stimulation enhances motor skill acquisition over multiple days through an effect on consolidation. Proc Natl Acad Sci U S A 106(5): 1590- 1595.
-
Bastani A, Jaberzadeh S (2012) Does anodal transcranial direct current stimulation enhance excitability of the motor cortex and motor function in healthy individuals and subjects with stroke: A systematic review and meta- analysis. Clin Neurophysiol [Internet] 123(4): 644-657.
-
Nitsche MA, Liebetanz D, Antal A, Lang N, Tergau F, et al. (2003) Transcranial Magnetic Stimulation and Transcranial Direct Current Stimulation. In: Transcranial Magnetic Stimulation and Transcranial Direct Current Stimulation (Supplements to Clinical Neurophysiology) 255-276.
-
Nitsche MA, Paulus W (2001) Sustained excitability elevations induced by transcranial DC motor cortex stimulation in humans. Neurology 57(10): 1899-1901.
-
Hayes HB, Jayaraman A, Herrmann M, Mitchell GS, Rymer WZ (2014) Trumbower RD. Daily intermittent hypoxia enhances walking after chronic spinal cord injury A randomized trial. Neurology 82(2): 104-113.
-
Navarrete Opazo A, Alcayaga J, Sepulveda O, Rojas E, Astudillo C (2017) Repetitive Intermittent Hypoxia and Locomotor Training Enhances Walking Function in Incomplete Spinal Cord Injury Subjects: A Randomized, Triple Blind, Placebo Controlled Clinical Trial. J Neurotrauma 34(9): 1803-1812.
- Electrolyte Considerations for Athletes
- Comprehensive Rehabilitation in Adults with Diabetic Peripheral Neuropathy: A Literature Review on Frequency, Intensity, and Duration Parameters
- Exercise Duration and Its Association with ADHD Symptom Severity in Children and Adolescents: A Parent-Reported Survey Study
- Adaptation of the Adult Neurophysiology of Pain Questionnaire for Use in Pediatrics
- A Non-Pharmacological Multidisciplinary Pain Program within a Hospital Wellness Program: A Mixed Methods Study
- The Effect of Frenkel's Exercise with PNF on Functional Reach in Stroke Survivors: A Randomized Control Trial