Training Rehabilitation Providers in Mental and Behavioral Health A Pilot Study
Background: Mental and behavioral health issues are rising and becoming increasingly prevalent as a comorbid clinical presentation in rehabilitation. Objective: To assess rehabilitation provider’s knowledge and attitudes towards patients with mental and behavioral health issues, following a training session on behavioral health. Design: Pre-immediate post and follow-up survey study Methods: A convenience sample of healthcare providers signed up for an online mental and behavioral class consisting of three 90-minute sessions. Prior to, immediately following and at 3-months following, participants completed a series of survey questions pertaining to beliefs, attitudes and knowledge related to mental and behavioral health. Likert scales were used to determine comfort with treating various mental and behavioral health issues and mental health-related knowledge was measured using the Mental Health Knowledge Schedule (MAKS). Results: Fourteen healthcare providers (92.3% female) completed the training and all measures. All levels of comfort with mental health shifted immediately following training, with only trauma being significant (p = 0.047), but did not remain at 3-month follow-up. Mental health-related knowledge improved significantly immediately following training (p = 0.008), and was still significantly improved 3-months after training (p = 0.011). Conclusion: An online training session is able to shift mental health-related knowledge in rehabilitation providers but not comfort with treating depression, anxiety and trauma. Additional research is needed to extrapolate and expand on the results of this pilot study.
Introduction
According to the National Institute of Health it is estimated approximately one in five people in the United Pilot Study States suffer from a mental, behavioral or emotional disorder and account for an annual spending in excess of $80 billion [1]. Within this data, it is estimated approximately six percent of Americans suffer from major depression [1], with the life-time prevalence of depression estimated at 21.3% in women and 12.7% in males [2]. Unfortunately, depression has been shown to also be a leading cause of suicide, thus showcasing the importance for healthcare providers to screen for depression, treat or refer accordingly [2].
Concerns over mental health, including depression is mounting, especially in light of the corona virus disease of 2019 (COVID-19) [3, 4]. The sudden acute respiratory syndrome that started in 2002 showed significant long-term changes in mental health with up to 65% of survivors developing major depression [5, 6]. Data from the COVID-19 pandemic shows similar potential impacts on mental health [3, 4]. It is well-documented that there’s a significant shortage of mental health providers globally, including for the treatment of depression [7, 8]. Persistent pain and depression often coexist, yet treatment for pain and depression often involve different healthcare providers and disciplines. For example, physical therapy (PT) is not typically seen as an avenue for the treatment of depression, yet it’s estimated that 45-50 million Americans annually seek PT for the care of low back pain, of which approximately 10-15 million suffer with chronic low back pain [9]. Recent studies have shown that approximately one in five patients attending outpatient PT present with moderate to severe depression, yet seeking care for an orthopedic condition [10, 11].
Within this coexistence of pain, disability and mental health is an important clinical mandate for rehabilitation providers such as PTs, PT assistants, occupational therapists, occupational therapy assistants, etc. - the need to know more about mental and behavioral health, including screening and treatment [12, 13, 14, 15, 16]. It has been proposed that PTs use validated tools to screen for depression and either attempt treatments for those on the lower end of the depression scale, or refer patients on the higher end of the scale to a behavioral health provider as needed [17, 18]. Therapeutic treatments may include mindfulness, meditation, exercise, pain neuroscience education, etc [16, 19, 20]. In 2020, amid the COVID-19 pandemic, the American Physical Therapy Association put forth a position statement supporting PT’s ability to evaluate and treat behavioral and mental health disorders, including depression [21]. This mandate aligns with previous calls to PT to embrace a true biopsychosocial model, screen for depression and develop therapeutic interventions for depression [13, 14, 15]. This shift in practice of taking on mental and behavioral health issues is new for PTs and it is unknown how they will respond to this professional and clinical mandate and furthermore, how it may impact their attitudes towards patients with comorbid behavioral health issues. This pilot study aimed to assess rehabilitation provider’s knowledge and attitudes towards patients with mental and behavioral health issues, following a training session on behavioral health.
Methods
Study Design
A private practice PT group in South Dakota and Minnesota gave permission for this training program and research review board approval was obtained from Southwest Baptists University, Bolivar MO. The study was a quality improvement project with pre, immediate-post and 3-month follow-up data collection from a convenience sample of therapist attending the training sessions.
Participants
Internal communication in the PT group was sent out, recruiting clinicians interested in mental and behavioral health to sign up and participate for free in a training session on mental and behavioral health. The sessions were open to all licensed healthcare providers including PT, PT assistants, occupational therapists, occupational therapy assistants, athletic trainers, speech-language pathologists as well as graduate students in these disciplines doing clinical rotations. All participants had to be willing and able to complete three survey packets before, immediately after and at 3-month follow-up. Additionally, they had to commit to attending both training sessions. Participants had to be fluent in writing and reading the English language.
Educational Session
The sessions were designed based on current best- evidence for mental and behavioral health in rehabilitation [14, 22, 23, 24, 25, 26, 27, 28]. The content included three 90-minute educational sessions (Table 1) for a total of 4.5 hours.
The presentations were developed by an interdisciplinary expert cohort consisting of a PT, occupational therapist and clinical psychologist. The content used in this presentation, with permission, was an abbreviated version of an 8-month post-graduate certification on mental and behavioral health (www.evidenceinmotion.com). The presenter was a PT with 24 years of clinical experience, a pain specialists and pain fellow and advanced, post-graduate training in mental and behavioral health. The original plan was for in-person training, but in lieu of COVID-19, the three sessions were be delivered online via Zoom™.
| Session 1 | Session 2 | Session 3 |
|---|---|---|
| Introduction | Depression | Creative therapies |
| Welcome | Anxiety | ¾ Writing |
| Trauma definition | Post-traumatic stress disorder | ¾ Art / craft |
| Pain neuroscience education | Adverse childhood events | ¾ Music |
| Words that heal / harm | Acute versus chronic brain | ¾ Dance |
| Therapeutic alliance | Psychology treatment | Nutrition |
| Goal setting | ¾ Talk therapy | Mindfulness |
| Sleep | ¾ Somatic experience | Meditation |
| ¾ Eye movement desensitization and reprocessing | Breathing | |
| ¾ Brain spotting | Movement therapies | |
| ¾ Neurofeedback | ¾ Yoga | |
| ¾ Prolonged exposure | ¾ Pilates | |
| ¾ Feldenkrais | ||
| ¾ Tai-chi | ||
| Additional resources |
Table 1: Content of the educational sessions.
Outcome measures
At initial intake, attendees completed a demographic survey. Internally, employee identification numbers were be used to match pre, post and follow-up responses. The presenter only had access to the employee identification numbers, not names, thus blinding her to the attendee’s identity. Demographic data collected included discipline (PT, PTA, OT, COTA, ATC, SLP and student), years of clinical experience, highest earned degree, level of pain science education, age and gender. Additionally, and specific to this study, attendees also had to report on:
- Have you previously taken any courses related to depression?
- Have you previously taken any courses related to behavioral health/mental health?
- Have you previously taken any courses related to anxiety?
- Percent of your daily practice in which you are treating patients with chronic pain?
- Are you currently experiencing any chronic pain?
- Have you previously experienced any chronic pain?
- Do you have a history of any mental health issue?
- Do you routinely screen for mental health conditions?
Three questions were be asked prior to the initial session, immediately following the final session and at 3-month follow-up. These questions pertain to mental and behavioral health and pain science, using a Likert Scale anchored with “very comfortable” on the one end (scored at a maximum of
5) and “very uncomfortable” on the other end (scored as 0):
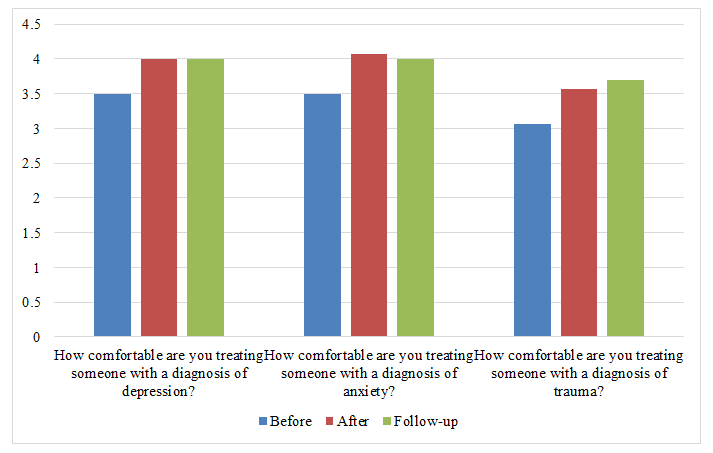
- How comfortable are you treating someone with a diagnosis of depression?
- How comfortable are you treating someone with a diagnosis of anxiety?
- How comfortable are you treating someone with a diagnosis of trauma?
Mental health-related knowledge was measured with the Mental Health Knowledge Schedule (MAKS) [29]. Part A comprise six items covering stigma-related mental health knowledge areas (help- seeking, recognition, support, employment, treatment and recovery) and Part B consist of six items that enquire about classification of various conditions as mental illnesses [30]. Overall test–retest reliability of the MAKS is 0.71 (Lin’s concordance statistic) and the overall internal consistency among items is 0.65 (Cronbach’s alpha). The total score is calculated so that higher MAKS scores indicate greater knowledge. Questions 1-6: Instructions: For each of statements 1– 6 below, respond by ticking one box only (ranging from agree strongly to don’t know)
- Most people with mental health problems want to have paid employment.
- If a friend had a mental health problem, I know what advice to give them to get professional help.
- Medication can be an effective treatment for people with mental health problems.
- Psychotherapy (e.g., talking therapy or counseling) can be an effective treatment for people with mental health problems.
- People with severe mental health problems can fully recover.
- Most people with mental health problems go to a health care professional to get help. Instructions: For items 7-12, say whether you think each condition is a type of mental illness by ticking one box only (ranging from agree strongly to don’t know).
- Depression
- Stress
- Schizophrenia
- Bipolar disorder (manic depression)
- Drug/substance addiction
- Grief
Statistical analysis
Microsoft Excel™ was used to enter data into spreadsheets. All observations were kept from the sample, with no modifications to the original data. Excel was used to explore descriptive statistics of the sample such as mean and standard deviation of demographics variables. RStudio Cloud version 1.4 of RStudio IDE was used to calculate the means of Personal Comfort variables, as well as the means of MAKS responses. Two-sided, paired sample t-tests in R were used to evaluate any differences between MAKS responses before, immediately after, and in follow-up.
Results
Participants
Overall, 14 participants attended all the sessions and completed the required forms before, immediately after and 3-months later (Table 2).
| Subjects (n = 14) | |
|---|---|
| Female | 13 (92.9%) |
| Age group: | |
| 20-25 | 2 (14.2%) |
| 26-35 | 7 (50%) |
| 36-45 | 2 (14.2%) |
| 46-55 | 2 (14.2%) |
| 56-65 | 1 (7.4%) |
| Discipline: | |
| Physical therapist | 6 (42.9%) |
| Physical therapist assistant | 5 (35.8%) |
| Occupational therapist | 1 (7.1%) |
| Occupational therapist assistant | 1 (7.1%) |
| Student | 1 (7.1%) |
| Clinical experience: | |
| 0-2 years | 3 (26.2%) |
| 2-5 years | 1 (7.1%) |
| 5-10 years | 3 (26.2%) |
| 10-15 years | 2 (14.3%) |
| 15-20 years | 3 (26.2%) |
| >20 years | 2 (14.2%) |
| Highest degree: | |
| Student | 1 (7.1%) |
| Associates | 2 (14.2%) |
| Bachelors | 5 (35.8%) |
| Masters | 1 (7.1%) |
| Doctorate | 5 (35.8%) |
| Have you previously taken any courses related to depression? | Yes = 2 (14.2%) |
| Have you previously taken any courses related to behavioral health/mental health? | Yes = 3 (21.4%) |
| Have you previously taken any courses related to anxiety? | Yes = 2 (14.2%) |
| Percent of your daily practice in which you are treating patients with chronic pain? | |
| 0-25% | 7 (50%) |
| 26-50% | 5 (35.8%) |
| 51-75% | 0 (0%) |
| 76-100% | 2 (14.2%) |
| Are you currently experiencing any chronic pain? | Yes = 0 (0%) |
| Have you previously experienced any chronic pain? | Yes = 0 (0%) |
| Do you have a history of any mental health issue? | Yes = 4 (28.6%) |
| Do you routinely screen for mental health conditions? | Yes = 3 (21.4%) |
Table 2: Demographic information for the participants.
Clinical comfort
Figure 1 show the three clinical questions pertaining to a clinician’s comfort in treating various diagnoses associated with mental and behavioral health. Immediately following the educational session, all diagnoses shifted to a higher level of comfort, but trauma was the only one reaching significance (p = 0.047), compared to depression (p = 0.068) and anxiety (0.055). At 3-month follow-up, none of the diagnoses shifted significantly from prior to the educational sessions (depression p = 0.068, anxiety p = 0.151 and trauma p = 0.057) (Figure 1).
Mental Health Knowledge Schedule
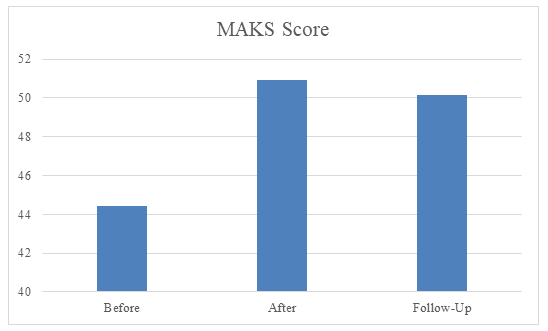
Figure 2 shows the overall, combined scores of the MAKS before, immediately after and at follow-up. Immediately following the training, the MAKS score improved significantly (p = 0.008), whereas a comparison of pre- and follow-up scores at 3-months showed a significant shift (p = 0.011) (Figure 2).
Discussion
This exploratory study is the first known study to deliberately try and alter rehabilitation provider’s comfort with treating and knowledge about behavioral and mental health. An online, abbreviate training session on behavioral and mental health for rehabilitation providers is able to increase knowledge of mental health, but not clinical comfort with various behavioral and mental health issues.
Mental and behavioral health issues are ever-increasing and not confined to only mental and behavioral health providers [1, 2]. Traditionally, psychiatrists, psychologists, licensed counsellors, etc., typically evaluate and treat mental and behavioral health issues. With increased prevalence of mental and behavioral issues such as depression, anxiety, adverse childhood events, trauma, etc., providers such as family physicians, emergency room physicians, surgeons and now rehabilitation providers find themselves with an increased need to understand mental and behavioral health [10, 24]. This implies that healthcare providers, including rehabilitation providers have a fundamental knowledge of these disorders. The results from this study show that knowledge can be positively impacted immediately following the training session and still be intact 3 months following training. Increased knowledge is a good first step, as it often leads to a variety of potential positive shifts over time as research and education in this area expands. For example, in lieu of the pain and opioid epidemic, it was established that PTs have a fundamental lack of knowledge related to modern pain science [31, 32]. Original studies, in line with the current paper’s design, showed that pain neuroscience education delivered to rehabilitation providers similarly increased knowledge of pain [32, 33], which has since been tied to positive shifts in attitudes and beliefs regarding persistent pain, self-reported clinical practice patterns and even superior clinical outcomes (Louw, et. al 2022 – submitted for publication) [34, 35]. The results from this study, albeit a small heterogenous sample, is an important first step in helping rehabilitation providers fulfill their place in the screening and management of a subgroup of patients with mental and behavioral health issues. Additionally, it should be recognized that this training was done via online delivery of the education, which may be meaningful as it’s positive effects could be replicated at scale versus in-person training alone [36].
The study failed to show any long-term meaningful shifts in self-reported comfort with treating patients presenting with depression, anxiety or trauma. This result is contrary to what has been seen in pain science where increased knowledge has been shown to change beliefs and attitudes regarding patients experiencing chronic pain [33, 34]. It can be argued that the shift in pain was positive given the fact that pain is such a prevalent issue in rehabilitation. Even without formal training in modern pain science, all therapist is trained in fundamentals of pain, including evaluation, screening and management, and that updating their current beliefs and attitudes were easier since they already had a baseline knowledge [37]. In contrast, entry- level occupational therapy curriculum provides significant exposure to behavioral medicine, but not PT. In fact, the current International Association of the Study of Pain’s new PT school guidelines, which is to take effect for entry-level PT programs in 2022, only now calls for inclusion of behavioral and mental health issues. This argument is underscored by the fact that only three of the participants (21%) prior to this presentation have taken a continuing education course on behavioral and mental health and even fewer have taken courses on depression (14%) or anxiety (14%). It is thus argued that increased knowledge, exposure clinically and changes to entry-level education may over time allow for increased clinical comfort in assessing and treating patients with mental or behavioral health issues.
The study contains numerous limitations. First, there is no control group to compare the participants who were trained or not trained. This pre- and post-study design, however, is often used in exploratory studies to test viability of larger scaled projects. Second, the sample size is very small and confined to a regional clinical group. Larger, more elaborate studies should be undertaken to extrapolated these findings., including a larger geographical, socioeconomic and cultural footprint.
Conclusion
An online training session is able to shift mental health-related knowledge in rehabilitation providers but not comfort with treating depression, anxiety and trauma. Additional research is needed to extrapolate and expand on the results of this pilot study.
References
-
Health (2015) N.I.o. Prevalence data for any mental illness and major depression prevalnce in the US. Available from: http://www.nimh.nih.gov/health/ statistics/prevalence/any-mental-illness-ami-among- us-adults.shtml
-
Kessler RC, Borges G, Walters EE (1999) Prevalence of and risk factors for lifetime suicide attempts in the National Comorbidity Survey. Arch Gen Psychiatry 56(7): 617-626.
-
Stein MB (2020) EDITORIAL: COVID-19 and Anxiety and Depression in 2020. Depress Anxiety 37(4): 302.
-
Rajkumar RP (2020) COVID-19 and mental health: A review of the existing literature. Asian J Psychiatr 52: 102066.
-
Mak IW, Chu CM, Pey CPan C, Chung Yiu MG, Chan VL (2009) Long-term psychiatric morbidities among SARS survivors. Gen Hosp Psychiatry 31(4): 318-326.
-
Lee AM, Wong JGWS, McAlonan GM, Cheung V, Cheung C, et al. (2077) Stress and psychological distress among SARS survivors 1 year after the outbreak. Can J Psychiatry 52(4): 233-240.
-
Andrilla CHA, Patterson DG, Garberson LA, Coulthard C, Larson EH, et al. (2018) Geographic Variation in the Supply of Selected Behavioral Health Providers. Am J Prev Med 54(6 Suppl 3): S199-S207.
-
Chaiyachati KH, Livesey C, Liao JM (2020) Going Beyond Cost-Sharing Parity to Improve Behavioral Health Access. JAMA Netw Open 3(10): e2020232.
-
Zheng P, Kao MC, Karayannis NV, Smuck M(2017) Stagnant Physical Therapy Referral Rates Alongside Rising Opioid Prescription Rates in Patients With Low Back Pain in the United States 1997-2010. Observational study 42(9): 670-674.
-
Louw A, Ashlyn R; Mendoza G, Kassal F, Brennan J, et al. (2021) Depression and patients attending outpatient physical therapy with musculoskeletal pain and disability. MOJ Orthop Rheumatol 13(6): 126-129.
-
Matheson LN, Verna J, Enright DS, Gherscovici E, Kemp B, et al. (2020) Development and validation of a method to screen for co-morbid depression by non-behavioral health practitioners treating musculoskeletal pain. Work 67(1): 55-65.
-
Boissonnault WG, Bass C (1991) Medical screening examination: not optional for physical therapists. J orthop sports phys ther 14(6): 241-242.
-
Foster NE, Delitto A (2011) Embedding psychosocial perspectives within clinical management of low back pain: integration of psychosocially informed management principles into physical therapist practice challenges and opportunities. Phys Ther 91(5): 790-803.
-
Keefe FJ, CJ Main CJ, George SZ (2018) Advancing Psychologically Informed Practice for Patients With Persistent Musculoskeletal Pain: Promise, Pitfalls, and Solutions. Phys Ther 98(5): 398-407.
-
Haggman S, Maher CG, Refshauge KM (2004) Screening for symptoms of depression by physical therapists managing low back pain. Phys Ther 84(12): 1157-1166.
-
Uckun AC, Donmez BK, Yurdakul FG, Garip Y, Bodur H (2020) the Role of Pain Catastrophizing and Depression in the Outcomes of Physical Therapy in a Prospective Osteoarthritis Cohort. Pain Physician 23(2): 209-218.
-
Pincus T, Burton AK, Vogel S, Field AP (2002) A systematic review of psychological factors as predictors of chronicity/disability in prospective cohorts of low back pain. Spine (Phila Pa 1976) 27(5): 109-120.
-
Delitto A, George SZ, Dillen LV, Whitman JM, Sowa G, et al. (2012) Low back pain. J orthop sports phys ther 42(4): A1-57.
-
Louw A, Elen W, Hawk D, Sturdevant N, Louw H, et al. (2021) Pain Neuroscience Education for Depression: A Pilot Study. Psychological Disorders and Research 42(2): 1-7.
-
Farah WH, Alsawas M, Mainou M, Alahdab F, Farah MH, et al. (2016) Non-pharmacological treatment of depression: a systematic review and evidence map. Evid Based Med 21(6): 214-221.
-
APTA (2020) Role of the Physical Therapist and APTA in Behavioral and Mental Health.
-
Nijs J, Wijma AJ, Willaert W, Huysmans E, Mintken P, et al. (2020) Integrating Motivational Interviewing in Pain Neuroscience Education for People With Chronic Pain: A Practical Guide for Clinicians. Phys Ther 100(5): 846- 859.
-
Dejesus RS, Vickers KS, Melin GJ,Williams MD (2007) A system-based approach to depression management in primary care using the Patient Health Questionnaire-9. Mayo Clin Proc 82(11): 1395-402.
-
Gallagher KC, Taylor CE (2021) Gatekeeper Training and the Medical Community’s Fight Against Depression and Suicide-A Shared Burden. JAMA Surg 156(3): 215-216.
-
Lowe B, Unutzer J, Callahan CM, Perkins AJ, Kroenke K (2004) Monitoring depression treatment outcomes with the patient health questionnaire-9. Med Care 42(12): 1194-1201.
-
Sterling M, Chadwick BJ (2010) Psychologic processes in daily life with chronic whiplash: relations of posttraumatic stress symptoms and fear-of-pain to hourly pain and uptime. Clin J Pain 26(7): 573-582.
-
Coronado RA, Brintz CE, McKernan LC, Master H, Motzny N, et al. (2020) Psychologically informed physical therapy for musculoskeletal pain: current approaches, implications, and future directions from recent randomized trials. Pain Rep 5(5): e847.
-
Main CJ, George SZ (2011) Psychologically informed practice for management of low back pain: future directions in practice and research. Physical therapy 91(5): 820-824.
-
Evans Lack S, Little K, Meltzer H, Rose D, Rhydderch D, et al. (2010) Development and psychometric properties of the Mental Health Knowledge Schedule. Can J Psychiatry 55(7): 440-448.
-
Evans Lacko S, Henderson C, Thornicrof G (2013) Public knowledge, attitudes and behaviour regarding people with mental illness in England 2009-2012. Br J Psychiatry Suppl 55: 51-57.
-
Moseley GL (2007) Reconceptualising pain acording to modern pain sciences. Physical Therapy Reviews 12: 169-178.
-
Moseley GL (2003) Unravelling the barriers to reconceptualisation of the problem in chronic pain: the actual and perceived ability of patients and health professionals to understand the neurophysiology J Pain 4(4): 184-189.
-
Cox T, Puentedura E, Louw A (2017) An Abbreviated Therapeutic Neuroscience Education Session Improves Pain Knowledge in First Year Physical Therapy Students But Does Not Change Attitudes or Beliefs. J Man Manip Ther 25(1): 11-21.
-
Louw A, Vogsland R, Marth L, Marshall P, Cox T, et al. (2019) Interdisciplinary Pain Neuroscience Continuing Education in the Veteran’s Affairs: Live Training and Live-Stream with 1-year Follow-up. Clin J Pain 35(11): 901-907.
-
Louw A, Sluka KA, Nijs J, Courtney CA, Zimney K (2020) Revisiting the Provision of Pain Neuroscience Education: An Adjunct Intervention for Patients, but a Primary Focus for Clinician Education. J Orthop Sports Phys Ther 51(2): 57-59.
-
Podolak J, Louw A, Benz P, Kruse A, Louw C, et al. (2019) A Randomized Trial of Live versus Video Delivery of Pain Neuroscience Education for Middle School Children. Psychological Disorders and Distress 2(2): 1-10.
-
Hoeger Bement MK, Sluka KA (2015) The current state of physical therapy pain curricula in the United States: a faculty survey. The journal of pain : official journal of the American Pain Society 16(2): 144-152.
- Electrolyte Considerations for Athletes
- Comprehensive Rehabilitation in Adults with Diabetic Peripheral Neuropathy: A Literature Review on Frequency, Intensity, and Duration Parameters
- Exercise Duration and Its Association with ADHD Symptom Severity in Children and Adolescents: A Parent-Reported Survey Study
- Adaptation of the Adult Neurophysiology of Pain Questionnaire for Use in Pediatrics
- A Non-Pharmacological Multidisciplinary Pain Program within a Hospital Wellness Program: A Mixed Methods Study
- The Effect of Frenkel's Exercise with PNF on Functional Reach in Stroke Survivors: A Randomized Control Trial