The Role of Exercise in the Management of Forwarding Head Posture A.K.A. Upper Crossed Syndrome. A Critically Appraised Topic
Introduction: Forward head posture is a common condition that presents in both chiropractic an physical therapy offices. Many times patients are given a multimodal approach to the correction of forward head posture. This paper looks to investigate what the current literature says about the role of exercise in forward head posture. Methods: The search strategy was performed using Pubmed for case studies and RCT’s within the last 5 years using the terms “anterior head, craniocervical flexion and exercise”. This search criterion resulted in 20 papers within the last 5 years. Further analysis for appropriate titles brought this number to 3 relevant papers. Conclusion: There is high-quality evidence to support the idea that exercise can be used to effectively manage those suffering from forward head carriage aka. upper crossed syndrome.
Focused Clinical Question
The focused clinical question that is being posed for this paper is “What is the role of exercise in the management of forwarding head posture aka. Upper crossed syndrome”.
Search Strategy
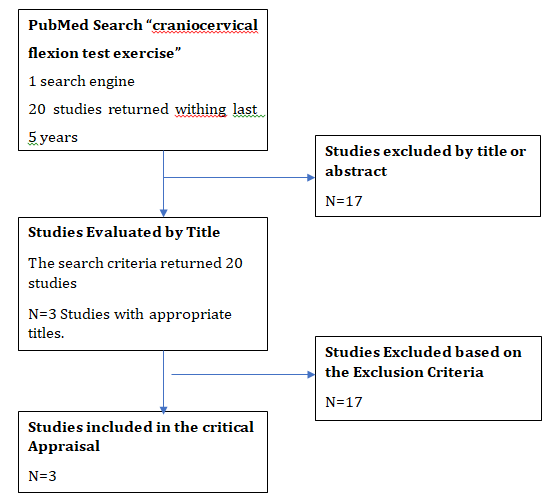
The search strategy for this paper began with a pub med review consisting of the terms anterior head, an exercise which returned few relevant papers within the allotted time bracket of 0-5 years. This prompted a second, more detailed search using the terms “craniocervical flexion and exercise”. This search criterion resulted in 20 papers within the last
5 years. Further analysis for appropriate titles brought this number to 3 relevant papers (Figure 1).
Evidence Quality
Evidence quality was assessed using the PEDro assessment for the remaining three studies (Table 1). With an average PEDro score of 8.67/10 the quality of evidence brought to answer this clinical question is high. The PEDro assessment was selected as the quality evaluation method as the three papers obtained were randomized clinical trials.
Results of Search
The results of the search brought back 20 papers with only 3 meeting the inclusion criteria for answering the focused clinical question of this critically appraised topic in comparing cranio-cervical flexion to exercise. The other 17 were either irrelevant or compared other modalities to the effects of exercise and cranio-cervical angles. Evidence quality was assessed using the PEDro assessment for the remaining three studies See (Table 1).
| Article 1 | Article 2 | Article 3 | |
|---|---|---|---|
| Study Title | Efficacy of Deep Cervical Flexor Muscle Training on Neck Pain, Functional Disability, and Muscle Endurance in School Teachers: A Clinical Trial | Progressive shoulder-neck exercise on cervical muscle functions in middle-aged and senior patients with chronic neck pain | Comprehensive corrective exercise program improves alignment, muscle activation and movement pattern of men with upper crossed syndrome: randomized controlled trial |
| Participants (Test subjects with relevant variables) | Sixty-five teachers (age, 25-45 years) with more than 5 years of teaching experience participated in this study | A total of 72 subjects aged ≥45 years with chronic neck pain | 24 men |
| Inclusion / Exclusion Criteria | The inclusion criteria included a chronic NP score of more than 5 on the numeric pain rating scale (NPRS), mild-to-moderate disability on neck disability index (NDI), and poor results on the CCF test. The exclusion criteria included the presence of any neurological signs or symptoms, history of spinal surgery, and any ongoing treatment for the pain. | Inclusion criteria: aged 45 years or older, experienced intermittent or continued neck pain for >3 months in the past year, measured ≥30 mm on the Visual Analogue Scale, were able to express themselves coherently, and had the patience to fill out the questionnaire. Excluded (N.=14) - Not meeting inclusion criteria (N.=6) - Declined to participate (N.=4) - Working factors (N.=4) | Inclusion criteria: Having any abnormality in the position and rhythm of the scapula, as measured by the scapular dyskinesis test, having postural changes such as excessive thoracic kyphosis (≥42°), forward head (≥44°) or round shoulder (≥49°) as measured by flexicurve and photogrammetry, respectively17. Exclusion criteria were having any visible malalignment in the pelvis or lower extremities, have a rotation higher than 5 degrees on the forward bending test because of scoliosis, which was measured with a scoliometer17, have a history of joint diseases in the spine, shoulder, and pelvis, fracture, surgery, and have a bodyweight outside the normal range (BMI between 18 and 25)42 |
| Outcome Measures | Pain intensity was measured using NPRS. The subjects rated their pain on the 0-10 rating scale, where 0 implied no pain and 10 implied the worst possible pain [28]. Endurance of DCF muscles was measured by the CCF test using a pressure biofeedback instrument (Stabilizer TM, Chattanooga Group, Inc., Chattanooga, TN). Functional disability was assessed using the NDI questionnaire. | Primarily the cranio-cervical Flexion Test. Secondary, the Superficial Cervical Muscle Strength Test (consisting of superficial neck flexor and extensor muscle strength). Outcomes measures were assessed before and after the intervention. | age, weight, height, BMI Surface electromyography of the selected muscles, including the upper trapezius (UT), middle trapezius (MT), lower trapezius (LT), and serratus anterior (SA) Scapular Dyskinesis Test Forward head and shoulder angles Thoracic kyphosis angle |
| Results | On day 0, there were no significant differences in the age, pain, muscle endurance, and disability levels between the groups. After initiating the intervention, although there were improvements in both groups, there was a statistically significant improvement in muscle endurance, pain, and disability in subjects who received additional training with pressure biofeedback. | RESULTS: After the intervention, the experimental group had a 56.48 point improvement in the performance index of the CGFT (P<0.001), a 1.71-kg improvement in superficial neck flexor strength (P<0.001), indicating that in 6-week intervention significantly influenced the improvement of cervical muscle functions. | Our results demonstrated that the CCEP can improve the movement patterns (scapular dyskinesis) and the alignments of the head, shoulder, and thoracic spine in people with UCS. These results showed positive effects for up to 4 weeks of detraining |
| Evidence Quality Score | SORT B, 2b PEDro Score: 9/10 | SORT B 2b PEDro Score: 8/10 | SORT A, 1b PEDro Score: 9/10 |
| Supportive Answer | Yes | Yes | Yes |
Table 1: Study Articles.
Results of Evidence Quality Assessed
Examined sixty-five teachers (age, 25-45 years) with more than 5 years of teaching experience [3]. The inclusion criteria included a chronic numerical pain score of more than 5 on the numeric pain rating scale (NPRS), mild-to-moderate disability on The Neck Disability Index (NDI), and poor results on the cranio-cervical flexion test (CCFT). The exclusion criteria included the presence of any neurological signs or symptoms, history of spinal surgery, and any ongoing treatment for the pain. Pain intensity was measured using NPRS. The subjects rated their pain on the 0-10 rating scale, where 0 implied no pain and 10 implied the worst possible pain. Endurance of the deep cervical neck flexor muscles was measured by the CCFT using a pressure biofeedback instrument (Stabilizer TM, Chattanooga Group, Inc., Chattanooga, TN). Functional disability was assessed using the NDI questionnaire. On day 0, there were no significant differences in age, pain, muscle endurance, and disability levels between the groups. After initiating the intervention, although there were improvements in both groups, there was a statistically significant improvement in muscle endurance, pain, and disability in subjects who received additional training with pressure biofeedback. Due to the design and caliber of this study, it was awarded a SORT B, 2b, and a PEDro Score: 9/10 [4]. Investigated A total of 72 subjects aged ≥45 years with chronic neck pain. Inclusion criteria: aged 45 years or older, experienced intermittent or continued neck pain for >3 months in the past year, measured ≥30 mm on the Visual Analogue Scale, were able to express themselves coherently and had the patience to fill out the questionnaire [4]. Excluded (N.=14) for not meeting inclusion criteria. (N.=6) - declined to participate, (N.=4) were excluded for working factors, and for (N.=4) the primary test was the cranio-cervical flexion test. The secondary test was the Superficial Cervical Muscle Strength Test (consisting of superficial neck flexor and extensor muscle strength). Outcomes measures were assessed before and after the intervention.
Results
After the intervention, the experimental group had a 56.48 point improvement in the performance index of the CCFT (P<0.001), a 1.71-kg improvement in superficial neck flexor strength (P<0.001), indicating that in 6-week intervention significantly influenced the improvement of cervical muscle functions. The design criteria along with the structure of the study earned this paper a SORT B score of 2b and a PEDro Score: 8/10.
Seidi, et al. [2] analyzed 24 men. Inclusion criteria: Having any abnormality in the position and rhythm of the scapula, as measured by the scapular dyskinesis test, having postural changes such as excessive thoracic kyphosis (≥42°), forward head (≥44°) or round shoulder (≥49°) as measured by “flexicurve” and photogrammetry, respectively. Exclusion criteria were having any visible malalignment in the pelvis or lower extremities, having a rotation higher than 5 degrees on the forward bending test because of scoliosis, which was measured with a scoliometer having a history of joint diseases in the spine, shoulder, and pelvis, fracture, surgery, and have a bodyweight outside the normal range (BMI between 18 and 25). Outcomes measured consisted of age, weight, height, BMI. Surface electromyography of the selected muscles, including the upper trapezius (UT), middle trapezius (MT), lower trapezius (LT), and serratus anterior (SA). Scapular Dyskinesis Test, forward head and shoulder angles, and thoracic kyphosis angle angles were measured as well. The results demonstrated that the cranio- cervical exercise program can improve the movement patterns (scapular dyskinesis) and the alignments of the head, shoulder, and thoracic spine in people with upper cross syndrome. These results showed positive effects for up to 4 weeks of detraining. This study was awarded a SORT score of A, 1b, and a PEDro score: of 9/10.
Clinical Bottom Line
There is statistically significant data to demonstrate that corrective exercise can improve cervical muscle endurance, pain, and disability [3]. Improvement in superficial neck flexor strength and overall cervical muscle function was able to be obtained in as little as a 6-week intervention [4]. The use of corrective exercise improved alignments of the head, shoulder, and thoracic spine in people with upper crossed syndrome even after 4 weeks of detraining [2].
Strength of Recommendation
With an average PEDro score of 8.87 (Table 1), there is high-quality evidence to support the notion that exercise is an effective intervention for increased cranio-cervical angle, upper crossed syndrome, and forward head posture.
Implications for Practice, Education, and Future Research
Of the three studies that passed the inclusion criteria for answering the focused clinical question, an average of 8.67 on the PEDro assessment was achieved. Such a score is directly indicative of high-quality evidence in favor of the use of exercise for the treatment of forwarding head posture aka upper crossed syndrome. Each study viewed a cohort of different ages and gender. One study demonstrated improvement in muscle endurance, pain, and disability while another suggested cervical muscle strength improvement. The final study demonstrated improvements in the movement pattern such as scapular dyskinesis along with the alignment of the head, shoulder, and thoracic spine in people with upper crossed syndrome.
Overall clinicians should feel confident in prescribing corrective exercise for those suffering from upper crossed syndrome as the exercises are both cost and time effective.
The selection of exercise can range from simplistic chin tucks and cranio-cervical flexion exercises to band-based resistance training for both the upper back and neck. Doing so supports the development of the deep cervical flexor, longus colli and longus capitus [3], while simultaneously strengthening the various upper back and neck muscles. Positive outcomes consist of reduced forward head posture, cervical spine pain and abnormal postures of the head, neck, and thorax.
Future research should be done to capitalize on the differences between exercises and outcomes along with the volume of exercise and outcomes. Follow-up research of this type can help establish if these results would be reached in a shorter time with higher loads, or does more time under tension matter, therefore, meaning higher reps and lighter loads? Such research would aid caregivers in overall program design and prescription.
Despite outcomes, both medical and non-medical providers should proceed with caution when dealing with cervical spine pain. Being diligent in ruling out red flags is crucial when evaluating spinal pain due to the rate at which the viscera can refer pain to this region. Various red flags can present as cervical spine pain therefore the ability to recognize and act quickly is essential. Nausea, vomiting, dizziness, and anxiety can all be signs of serious or life- threatening conditions associated with cervical spine pain. Practitioners should have an emergency response plan in place in case any of these symptoms present before, after, and during any neck exercise program.
References
-
Ferracini GN, Chaves TC, Dach F, Bevilaqua Grossi D, Fernández de Las Peñas C, et al. (2017) Analysis of the cranio cervical curvatures in subjects with migraine with and without neck pain. Physiotherapy 103(4): 392-399.
-
Seidi F, Bayattork M, Minoonejad H, Andersen LL, Page P (2020) Comprehensive corrective exercise program improves alignment, muscle activation and movement pattern of men with upper crossed syndrome: Randomized controlled trial. Scientific reports 10(1): 20688.
-
Iqbal ZA, Alghadir AH, Anwer S (2021) Efficacy of Deep Cervical Flexor Muscle Training on Neck Pain, Functional Disability, and Muscle Endurance in School Teachers: A Clinical Trial. Biomed Res Int 7190808.
-
Lin IH, Chang KH, Liou TH, Tsou CM, Huang YC (2018) Progressive shoulder-neck exercise on cervical muscle functions in middle-aged and senior patients with chronic neck pain. Euro J physical and rehabilitation medicine 54(1): 13-21.
- Electrolyte Considerations for Athletes
- Comprehensive Rehabilitation in Adults with Diabetic Peripheral Neuropathy: A Literature Review on Frequency, Intensity, and Duration Parameters
- Exercise Duration and Its Association with ADHD Symptom Severity in Children and Adolescents: A Parent-Reported Survey Study
- Adaptation of the Adult Neurophysiology of Pain Questionnaire for Use in Pediatrics
- A Non-Pharmacological Multidisciplinary Pain Program within a Hospital Wellness Program: A Mixed Methods Study
- The Effect of Frenkel's Exercise with PNF on Functional Reach in Stroke Survivors: A Randomized Control Trial