Effects of Occupational Therapy on Standing Trouser-Wearing Motion in Children with Autism Spectrum Disorder
This study aimed to investigate the effect of occupational therapy (OT) on the standing trouser-wearing motion of children with autism spectrum disorder (ASD). Study participants included 12 children (6 boys and 6 girls) with an IQ ranging from 88–113 who were diagnosed with ASD by pediatricians or child psychiatrists and using child development support services and after-school day services for children with disabilities. The therapist conducted 60-min one-on-one OT interventions with participants. The total number of OT interventions for participants ranged from 5 to 11 times. During this period, participants performed one-legged standing and standing trouser-wearing motion four times as an experimental task. Parameters analyzed were foot pressure, center of pressure (COP), and motion analysis. We found that 5 of 12 participants showed improvement in trouser-wearing motion from type 1 to type 2, and three from type 2 to type 3. The anterior-posterior-COP-max, anterior-posterior-COP-trajectory, and medial-lateral-COP-trajectory of the trouser-wearing motion decreased significantly in the third and fourth experimental tasks compared with the first (p<.05); however, there was no significant difference in the medial-lateral-COP-max. Furthermore, participants could bend their trunk forward easily during the final OT intervention. These findings suggest that five sessions of play-based OT could be effective in improving standing trouser-wearing motion in children with ASD. As the effect of OT was not observed in each parameter of one-legged standing, the existence of task specificity is suggested.
Introduction
The stages of child development are neck sitting, turning over, sitting up, grasping, pawing, and walking [1, 2]. Three- year-old children can then stand on one leg for 2–3 s. Self- care for three-year-old children includes “being able to take off clothes by oneself,” “putting on tops through the head by oneself,” and “being able to unbutton buttons approximately
2.5 cm in diameter [3].” By age 6, children are generally independent in dressing/undressing.
Elementary schools in Japan require children to change their clothes in a short period between classes. Many children can stand and change their clothes in a short time. However, we often receive consultations from school teachers regarding children who have difficulty changing their clothes [4]. Problems in dressing behavior include mistaking the front and back of the upper and lower garments, mistaking the dressing procedure, and taking too long time to change. Although parents do not consider these behaviors as alarming among preschool children, they can become a problem in later life. In Japan, school teachers have difficulty dealing with the highly individualized daily activities of children. The changing clothes behavior of children who are “not good at changing clothes” can be considered as strange by other children, and they can become targets of “bullying.” Many children with autism spectrum disorder (ASD) who use day-care services for children with disabilities have difficulty changing their clothes. Of the 446 children with ASD using the service, 161 (36.1%) were perceived to be “unskilled at changing clothes” by their parents or the concerning staff. Of these 161 children, 92 (48.2%) were at a preschool-age. These pre- and post-school children exhibit trunk hypotonia and high trunk sway during changing activities. Therefore, children with ASD require more time to change their clothes owing to repetition of the same process, attempt to carry it out sluggishly, or compensatory movements. Therefore, developmental barriers include cognitive aspects, such as the front/back/left/right of clothing and motion procedures and motor performance delays that make it difficult to carry out the changing clothes operation itself.
After a 60-min intervention of one-on-one play-based OT between a therapist and a participant (age range: 5 years and 3 months to 8 years and 2 months; IQ: 82-117), a previous study reported significant reductions in the maximum excursion and total trajectory of center of pressure (COP) in the anterior-posterior direction of the first supporting leg in the standing trouser-wearing motion [4]. These participants found it easier to maintain a forward bend of the trunk while standing on one foot in the trouser-wearing motion. However, each parameter of the participants’ one-legged stand had no intervention effect. These findings may be attributed to task specificity caused by the trouser-wearing motion, and the effects of OT intervention for ASD can be applied in daily life activities.
This study aimed to determine the effect of OT intervention on the standing trouser-wearing motion of children with ASD.
Methods
Participants
Participants included 12 children, with IQ scores ranging between 82 and 113, who were diagnosed with ASD (including pervasive developmental disorders and attention- deficit hyperactivity disorder [ADHD] as complications) by pediatricians or child psychiatrists. The exclusion criteria were as follows: any health issues that could affect balance, medication changes within 6 weeks prior to participation, significant surgery within 6 months prior to testing, or history of self-injury or injury to others in a routine therapy setting.
Ethical considerations
Participants and their parents read and understood the instructions for the study and participated voluntarily. Ethical approval for this study was granted by the Ethics Committee of the Yamagata Prefectural University of Health Sciences (approval number: 1809-18 and approval date: September 27, 2018).
Tasks and OT intervention
The therapist and the participant had a one-on-one session lasting for approximately 60 min. The number of OT interventions ranged from 5–11. This study was conducted within the usual scope of OT interventions. The reason for the variation in the number of OT interventions was the mix of participants with once-weekly and twice-weekly OT interventions for their convenience.
The OT intervention comprised nine types of play (Table 1) categorized into the following three groups: spontaneous play, non-competitive games, and competitive games [4, 5]. Motion elements necessary to improve standing balance, coordination of the trunk and upper and lower extremities, and grasping ability were incorporated at each stage [6, 7, 8]. OT interventions were based on the needs of each child and included the ten key therapeutic strategies (arranging the room to entice engagement, ensuring physical safety, presenting sensory opportunities, attaining and maintaining optimal arousal levels, tailoring activities to present the just- right challenge, ensuring that activities are successful, guiding the self-regulation of behavior, creating a playful context, collaborating in activity choice, and fostering therapeutic alliances) that a therapist would use when providing sensory integration (SI)-based treatment to a child [6, 7, 8].
The participants selected three from the nine types of play [4]. Additionally, the following types of play were added to improve trouser-wearing motion (Figure 1): walking on the lumber to improve the balancing ability to stand on one leg, rolling a balance ball to improve the coordination of the upper and lower extremities in a trunk-bent position, and tug- of-war game. The purpose was to facilitate co-contraction and alternative contraction of the upper and lower extremities and trunk muscles and to improve grasping strength.

Figure 1: Three types of play to improve trouser-wearing motion of children with ASD. The left picture shows walking on a lumber (2 m long, 10 cm wide, and 10 cm high). The three spontaneous plays were walking sideways, walking in tandem, and walking while picking up cards on the course. The center picture shows rolling the balance ball. Participants pushed and rolled a balance ball 50-cm in diameter using both hands. The three non-competitive play activities were straightforward, backward and forward, and dodging obstacles along the way. The right picture shows playing of tug of war. Participants, along with a therapist, pulled a 3-m long rope. Tug-of-war was performed on the floor and on a cushion.
| Stage 1 | Stage 2 | Stage 3 | |
|---|---|---|---|
| Spontaneous play | Getting on the swing | Jumping in the big cloth bag | Jumping on a trampoline |
| Spontaneous play | (1) Participants ride while lying on their stomachs or on their backs with their faces up. | (1) Participants enter the large cloth bag, grasp the end of the bag, and stand up. | (1) Participants jump in the same position on the trampoline. |
| Spontaneous play | (2) Participants ride on a straddling seated position. | (2) Participants enter the large cloth bag and jump with the bag | (2) Participants change direction by about 90 degrees while jumping on the trampoline. |
| Spontaneous play | (3) Participants stand and pedal the swing. | (3) Participants move with the large cloth bag by jumping back and forth or in left and right directions. | (3) Participants catch balloons and balls while jumping on the trampoline. |
| Non-competitive game | Climbing up and down a 2-meter high ladder | Climbing up and down a 2-meter high bouldering wall | Climbing up and down a 2-meter high giant cushion |
| Non-competitive game | (1) Participants climb up the ladder. | (1) Participants climb up the bouldering wall. | (1) Participants climb up the giant cushion. |
| Non-competitive game | (2) Participants climb down the ladder. | (2) Participants climb down the bouldering wall. | (2) Participants climb down the giant cushion. |
| Non-competitive game | (3) Participants climb up and down the ladder. | (3) Participants climb up and down the bouldering wall. | (3) Participants climb up and down the giant cushion. |
| Competitive game | 9 m race in a posture of crawling on hands and knees | 9 m race in a high crawling posture position | 9 m race on a scooter board in prone position |
| Competitive game | (1) Participants compete with the staff. | (1) Participants compete with the staff. | (1) Participants compete with the staff. |
| Competitive game | (2) Participants will compete in a time trial. | (2) Participants will compete in a time trial. | (2) Participants will compete in a time trial. |
Table 1: Concepts of occupational therapy (OT) interventions.
Instrumentation and data acquisition
Parameters analyzed were foot pressure and COP, which were recorded from the frontal and the right sagittal planes using two video cameras (C920; Logitech International SA, Lausanne, Switzerland). Each participant was asked to put on the 100% polyester experimental trousers that were measured to the child’s height.
Foot pressure and COP were measured using a foot pressure platform (EM-MP2703; Noraxon USA, Arizona, USA) with a time resolution of 100 Hz and a spatial resolution of 16 bits. The platform was calibrated at the time of the setup. The displacement of the COP was in the anterior–posterior direction of the short side of the platform, whereas the long side was in the medial–lateral direction. All devices were synchronized using the software (MR3 ver.3.12; Noraxon USA, Arizona, USA) used for measurement and analysis.
OT evaluation
• Clinical profiles Before the first evaluation, participants’ height, weight, leg length, and leg width were measured. The sensory sensitivity of the participants was examined using the Short Sensory Profile [9, 10].
• Experimental task All participants performed two tasks after the first through to the fourth OT experimental task. The experimental task started in the same period; the second and third experimental tasks were different for each participant; the fourth experimental task was conducted during the same period. Task 1: Participants were instructed to maintain a standing position with one leg and open their eyes for a maximum of 10 s. They stood on one foot on the platform of the foot pressure distribution analysis device. The order of the one-legged stand and the position of the upper extremities were determined by the participants. Task 2: The participants were instructed to put on the trousers while standing. The participants were instructed to change their trousers at their own pace.
• Procedure Tasks 1 and 2 after OT interventions were conducted in a quiet, well-lit room (640 lx, temperature 24 °C). Participants entered the room and were briefed on the tasks. Participants then stood upright on the platform.
The measurements were performed in the order of task 1 and task 2. The period from the start to the end of the task lasted approximately 10 min.
Definitions of terms
Terms were defined as previously described [11]. Briefly, the first swing leg (FL) was the first leg that passed through the trousers. The second leg (SL) was the second swing leg after the FL. The first support leg (FSL) was the first support leg, whereas the second support leg (SSL) was the next support leg after the FSL.
Motion phase
Task 2 was divided into five phases based on the video data, as previously described [11]. We analyzed the second and fourth phases were further divided into three stages. The first stage was when the FL or SL motions began until either was raised to the trousers of the waistline. The second stage was when the participant’s foot began to enter the trousers until the foot was fully inside the trousers. The third stage was the period from the end of the second stage until FL or SL landed on the floor.
Data analysis
The method of putting on and taking off the trousers worn by the participants and the experimental trousers was compared by several examiners to assess the reproducibility of the participants’ motions in Task 2. Based on the video, the trouser-wearing motion was divided into five phases [11]; only phases 2 and 4 were analyzed. The reasons for analyzing these phases were in accordance with previous studies [4, 11] as the characteristics were classified into three types based on a previous study [11]. Characteristics of Type 1 were: “Put swing leg on the floor during motion”, “Hook foot on the trousers and repeat the same procedure”, “Grasped the waistline of the trousers using one hand”, “Flexed the trunk slightly”, and “Flexed the hip and knee joints of the swing leg greatly”. Characteristics of Type 2 were: “Grasped of the waistline of the trousers in a higher position than the support leg knee using both hands” and “Fixed the swing leg and pulled up the waistline of the trousers to fit swing leg”. Characteristics of Type 3 were “Grasped of the waistline of the trousers near the support leg knee using both hands” and “Fixed the trousers and extended swing leg to fit the trousers”.
For Tasks 1 and 2, one-legged standing times and COPs were investigated. The maximum excursion of the COP in the anterior–posterior direction (A/P-COP-max) and in the medial–lateral direction (M/L-COP-max), the COP trajectory length in the anterior–posterior direction (A/P-COP- trajectory), and the COP trajectory length in the medial– lateral direction (M/L-COP-trajectory) were calculated based on the temporal transition of COP. SPSS statistical software (version 24.0; SPSS, Chicago, IL, USA) was used for statistical analysis. In Tasks 1 and 2, the Friedman test was used to compare the one-legged standing time, COP trajectory of the supporting leg, and COP-max from the first to the fourth time. Multiple comparisons were performed using the Wilcoxon signed-rank test with the Bonferroni correction. The significance level was set at 5% for all tests.
Results
The clinical profiles of each participant are shown in Table 2. The number of OT interventions from the first to the fourth evaluation ranged from 5-11. The sensory profiles of each participant are shown in Table 3. Regarding the sensory profiles, Eleven of the twelve participants had a definite difference (above average + 2SD) in at least one of the six sensory sensitivity items.
| Participant | Age | Diagnoses | Sex | Height (cm) | Weight (kgf) | Foot length(cm) | Foot width(cm) | Number of OT interventions |
|---|---|---|---|---|---|---|---|---|
| 1 | 8 years, 1 month | ASD (PDD) | F | 120 | 26.6 | 15.5 | 4.1 | 10 |
| 2 | 7 years, 1 month | ASD | M | 120 | 22.2 | 15.2 | 3.6 | 8 |
| 3 | 6 years, 5 months | ASD | M | 115 | 16.5 | 13.7 | 3.5 | 8 |
| 4 | 5 years, 8 months | ASD | F | 113 | 17.2 | 13.2 | 3.2 | 6 |
| 5 | 5 years, 3 months | ASD | M | 110 | 16.0 | 13.3 | 4.1 | 11 |
| 6 | 7 years, 6 months | PDD | M | 120 | 27.2 | 15.6 | 3.5 | 9 |
| 7 | 8 years, 2 months | ASD | F | 133 | 29.9 | 15.9 | 4.3 | 5 |
| 8 | 6 years, 9 months | ASD | F | 113 | 19.2 | 13.9 | 3.4 | 8 |
| 9 | 6 years, 4 months | ASD | F | 110 | 14.3 | 12.3 | 3.9 | 6 |
| 10 | 7 years, 11 months | ASD | F | 120 | 21.5 | 13.6 | 4 | 6 |
| 11 | 7 years, 6 months | ASD | M | 115 | 24.5 | 19.4 | 7.8 | 7 |
| 12 | 7 years, 11 months | ASD | M | 120 | 28.0 | 16.7 | 7.7 | 10 |
| Max | 133 | 29.9 | 19.4 | 7.8 | (11) | |||
| Min | 110 | 14.3 | 12.3 | 3.2 | (5) | |||
| Average (Median) | 117.4 | 21.9 | 14.9 | 4.4 | (7) | |||
| SD | 6.3 | 5.3 | 2.0 | 1.6 | (2) |
Table 2: Clinical profiles.
| Participant | Sensory Sensitivity | |||||
|---|---|---|---|---|---|---|
| Tactile Sensitivity | Movement Sensitivity | Underresponsive/Seeks Sensation | Auditory Filtering | Low Energy/ Weak | Visual/Auditory Sensitivity | |
| 1 | ||||||
| 2 | ||||||
| 3 | ||||||
| 4 | ||||||
| 5 | ||||||
| 6 | ||||||
| 7 | ||||||
| 8 | ||||||
| 9 | ||||||
| 10 | ||||||
| 11 | ||||||
| 12 |
Table 3: Sensory sensitivity for each participant.
Typical performance:Average value+1SD or less
Probable difference:Average value+1SD and lower range than average value+2SD Definite difference:Above average + 2SD Table 3: Sensory sensitivity for each participant.
The results of the COP transition for one-legged standing with eyes open after the first to fourth OT experimental tasks are shown in (Table 4). The mean time required to stand on the right and left foot was not significantly different between all four tasks. There was no significant difference in mean regarding the A/P-COP-max, M/L-COP-max, the A/P- COP-trajectory, and M/L-COP-trajectory during one-legged standing values for the right and left foot after the first through to the fourth experimental task.
| Participant | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | M | SD | P-value | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| One-legged standing time (sec) | 1st | R | 10 | 8.8 | 10 | 2.2 | 6.3 | 8.9 | 9.2 | 9.7 | 9.2 | 10 | 10 | 1.7 | 8.0 | 3.0 | a: 0.211 v: 0.232 |
| L | 10 | 10 | 10 | 8.7 | 3.7 | 9.8 | 10 | 10 | 10 | 10 | 10 | 5.9 | 9.0 | 2.1 | |||
| 2nd | R | 10 | 5.3 | 10 | 7.9 | 4.1 | 6.1 | 5.0 | 10 | 10 | 10 | 10 | 8.3 | 8.1 | 2.3 | ||
| L | 10 | 7.2 | 10 | 5.7 | 10 | 6.0 | 10 | 8.8 | 10 | 10 | 5.8 | 10 | 8.6 | 1.9 | |||
| 3rd | R | 10 | 10 | 5.5 | 8.4 | 10 | 10 | 10 | 10 | 10 | 9.3 | 10 | 9.6 | 9.4 | 1.3 | ||
| L | 10 | 3.2 | 10 | 10 | 10 | 10 | 10 | 10 | 10 | 10 | 10 | 10 | 9.4 | 2.0 | |||
| 4th | R | 10 | 6.8 | 10 | 10 | 10 | 10 | 8.2 | 10 | 10 | 9.6 | 8.0 | 8.6 | 9.3 | 1.1 | ||
| L | 10 | 6.5 | 10 | 5.9 | 10 | 10 | 5.2 | 10 | 10 | 10 | 8.6 | 10 | 8.9 | 1.9 | |||
| A/P-COP-max (%) | 1st | R | 1.6 | 2.7 | 3.3 | 1.5 | 4.9 | 1.7 | 1.7 | 3.7 | 3.3 | 1.8 | 3.6 | 2.0 | 2.6 | 1.1 | b: 0.893 w: 0.456 |
| L | 1.9 | 6.1 | 2.6 | 2.2 | 3.4 | 2.3 | 2.9 | 2.3 | 4.6 | 1.8 | 2.9 | 2.9 | 3.0 | 1.2 | |||
| 2nd | R | 8.5 | 1.5 | 2.2 | 2.0 | 5.0 | 2.0 | 2.8 | 4.7 | 3.3 | 1.8 | 2.3 | 1.2 | 3.1 | 2.1 | ||
| L | 3.9 | 2.2 | 2.5 | 1.6 | 2.9 | 2.1 | 2.4 | 4.2 | 4.6 | 1.8 | 3.1 | 1.8 | 2.8 | 1.0 | |||
| 3rd | R | 2.9 | 3.9 | 2.0 | 2.2 | 3.2 | 3.3 | 3.3 | 2.3 | 2.3 | 2.4 | 2.1 | 2.1 | 2.7 | 0.6 | ||
| L | 2.1 | 2.5 | 1.6 | 1.6 | 3.5 | 1.9 | 2.2 | 3.1 | 2.6 | 5.1 | 3.8 | 2.7 | 2.7 | 1.0 | |||
| 4th | R | 4.1 | 2.5 | 2.2 | 1.5 | 3.6 | 2.2 | 2.3 | 2.9 | 3.1 | 1.8 | 3.3 | 2.0 | 2.6 | 0.8 | ||
| L | 4.2 | 4.0 | 3.4 | 4.1 | 2.0 | 2.3 | 2.7 | 2.1 | 2.6 | 2.6 | 5.5 | 1.8 | 3.1 | 1.1 | |||
| M/L-COP-max (%) | 1st | R | 2.7 | 4.3 | 4.5 | 2.2 | 4.8 | 3.7 | 3.1 | 4.0 | 3.6 | 2.6 | 3.7 | 3.2 | 3.5 | 0.8 | c: 0.166 x: 0.404 |
| L | 3.0 | 3.9 | 3.5 | 3.3 | 4.6 | 3.9 | 3.0 | 3.9 | 2.5 | 2.7 | 3.0 | 4.9 | 3.5 | 0.7 | |||
| 2nd | R | 18.2 | 4.7 | 6.2 | 3.7 | 7.4 | 2.5 | 3.3 | 6.2 | 3.6 | 2.6 | 4.3 | 2.5 | 5.4 | 4.3 | ||
| L | 5.3 | 4.7 | 3.6 | 2.0 | 3.9 | 5.1 | 3.3 | 4.6 | 2.5 | 2.7 | 3.3 | 2.8 | 3.7 | 1.1 | |||
| 3rd | R | 3.7 | 3.9 | 3.8 | 2.9 | 4.6 | 5.5 | 4.2 | 3.1 | 3.7 | 3.4 | 3.4 | 2.6 | 3.7 | 0.8 | ||
| L | 2.8 | 9.9 | 9.1 | 2.5 | 5.1 | 3.7 | 3.2 | 5.1 | 4.4 | 3.2 | 4.5 | 2.5 | 4.7 | 2.4 | |||
| 4th | R | 4.0 | 4.1 | 4.4 | 3.0 | 6.0 | 2.9 | 3.2 | 5.4 | 3.9 | 3.5 | 7.5 | 3.0 | 4.3 | 1.4 | ||
| L | 4.2 | 5.1 | 3.6 | 7.8 | 4.5 | 3.9 | 3.4 | 3.8 | 3.2 | 3.3 | 2.2 | 2.3 | 3.9 | 1.5 | |||
| A/P-COP- trajectory (%/ sec) | 1st | R | 13.8 | 8.1 | 5.7 | 4.4 | 7.9 | 4.7 | 3.8 | 8.8 | 3.3 | 3.9 | 5.1 | 5.2 | 6.2 | 3.0 | d: 0.592 y: 0.416 |
| L | 6.0 | 2.2 | 6.4 | 5.2 | 7.8 | 3.6 | 4.1 | 7.9 | 2.8 | 4.0 | 6.2 | 3.3 | 4.9 | 1.9 | |||
| 2nd | R | 4.4 | 5.5 | 6.0 | 5.0 | 13.0 | 4.8 | 3.5 | 9.6 | 6.4 | 3.8 | 4.8 | 3.1 | 5.8 | 2.8 | ||
| L | 4.2 | 12.4 | 7.7 | 4.3 | 5.0 | 5.0 | 3.7 | 8.4 | 6.6 | 3.9 | 6.6 | 3.7 | 6.0 | 2.6 | |||
| 3rd | R | 5.7 | 5.1 | 6.2 | 4.0 | 5.4 | 4.4 | 4.7 | 5.1 | 5.7 | 4.5 | 4.8 | 3.7 | 4.9 | 0.7 | ||
| L | 4.8 | 6.4 | 4.4 | 4.5 | 5.5 | 3.7 | 4.2 | 7.1 | 6.4 | 4.8 | 6.2 | 4.4 | 5.2 | 1.1 | |||
| 4th | R | 8.2 | 6.0 | 5.6 | 5.1 | 6.2 | 5.2 | 4.5 | 5.9 | 5.0 | 4.6 | 5.8 | 3.1 | 5.4 | 1.2 | ||
| L | 7.0 | 8.7 | 7.3 | 8.3 | 4.9 | 6.8 | 4.8 | 4.7 | 5.4 | 4.6 | 6.7 | 3.4 | 6.0 | 1.7 | |||
| M/L-COP- trajectory (%/ sec) | 1st | R | 9.9 | 5.5 | 3.3 | 2.6 | 3.1 | 4.2 | 2.9 | 4.2 | 1.2 | 2.2 | 3.5 | 4.5 | 3.9 | 2.2 | e: 0.874 z: 0.294 |
| L | 3.9 | 4.0 | 3.9 | 2.9 | 3.7 | 2.8 | 2.5 | 4.4 | 1.4 | 2.4 | 3.7 | 2.6 | 3.2 | 0.9 | |||
| 2nd | R | 3.5 | 2.6 | 6.5 | 2.7 | 7.2 | 3.4 | 1.6 | 4.2 | 4.1 | 2.5 | 3.3 | 1.9 | 3.6 | 1.7 | ||
| L | 3.1 | 4.0 | 3.8 | 2.3 | 4.0 | 3.2 | 1.8 | 4.9 | 2.5 | 2.4 | 3.2 | 2.3 | 3.1 | 0.9 | |||
| 3rd | R | 2.6 | 2.9 | 11.1 | 3.0 | 3.1 | 3.6 | 2.8 | 3.1 | 2.9 | 2.8 | 3.2 | 3.0 | 3.7 | 2.4 | ||
| L | 2.8 | 2.5 | 3.1 | 2.1 | 3.8 | 2.2 | 2.2 | 4.6 | 4.1 | 1.9 | 4.1 | 2.6 | 3.0 | 0.9 | |||
| 4th | R | 4.3 | 3.2 | 4.6 | 2.4 | 5.9 | 2.7 | 2.8 | 3.6 | 3.1 | 2.8 | 3.7 | 2.5 | 3.5 | 1.0 | ||
| L | 3.6 | 2.6 | 5.5 | 5.1 | 5.7 | 3.8 | 2.7 | 3.6 | 2.6 | 2.3 | 3.9 | 2.4 | 3.7 | 1.2 |
Table 4: Center of Pressure (COP) transition under one-legged standing with eyes open.
Table 4: Center of Pressure (COP) transition under one-legged standing with eyes open. A/P indicated anterior to posterior side. A/P direction of COP amplitude was normalized by dividing the COP amplitude by the foot length. M/L indicated latelal to medial side. M/L direction of COP amplitude was normalized by dividing the COP amplitude by the foot width. OT indecated occupational therapy. M and SD indicated mean and standerd diviation. Abbreviations for the images as well as Table 5. a, b, c, d, e: 1st OT vs 2nd OT vs 3rd OT vs 4th OT of right foot. v, w, x, y, z: 1st OT vs 2nd OT vs 3rd OT vs 4th OT of left foot.
Participant 1 2 3 4 5 6 7 8 9 10 11 12 M SD p-value
1st F 1.5 1.8 2.6 2.8 2.2 1.4 3.5 1.8 1.7 1.7 1.8 1.5 2.0 0.6
S 1.4 0.9 1.7 1.4 3.2 1.2 1.2 1.9 1.7 1.1 1.5 4.2 1.8 1.0
One-legged standing time during wearing torsors(sec)
2nd F 1.4 3.1 1.6 3.5 5.7 1.6 1.7 1.6 2.2 1.7 1.5 0.8 2.2 1.3 S 1.4 2.1 1.7 2.8 2.4 2.4 1.9 2.4 1.6 1.1 1.1 1.0 1.8 0.6
3rd F 1.4 1.8 3.4 3.0 1.6 1.9 1.7 1.4 2.7 1.2 1.7 1.9 2.0 0.7 S 1.3 2.2 2.1 1.4 1.4 2.5 1.9 1.2 1.9 0.7 1.4 0.8 1.6 0.6 f: 0.252 q: 0.443
- 4th
- F
- 1.1
- 2.0
- 2.0
- 2.5
- 1.9
- 1.4
- 1.1
- 1.5
- 1.8
- 1.6
- 1.6
- 1.4
- 1.7
- 0.4
- S
- 0.8
- 1.4
- 2.4
- 1.6
- 1.7
- 0.9
- 1.8
- 1.4
- 1.4
- 1.3
- 1.0
- 1.4
- 1.4
- 0.4
- 1st
- F
- 3.2
- 4.2
- 3.4
- 3.3
- 4.7
- 4.3
- 4.5
- 4.5
- 3.3
- 3.0
- 3.3
- 3.5
- 3.8
- 0.6
- S
- 2.7
- 3.5
- 4.3
- 2.9
- 3.3
- 1.9
- 1.4
- 4.6
- 2.3
- 3.9
- 3.3
- 4.8
- 3.2
- 1.1
- 2nd
- F
- 0.9
- 3.2
- 3.6
- 3.3
- 6.9
- 1.9
- 2.7
- 3.9
- 3.7
- 3.0
- 2.3
- 0.9
- 3.0
- 1.6
- S
- 3.2
- 2.5
- 1.8
- 4.6
- 2.1
- 4.2
- 4.8
- 2.7
- 5.1
- 3.9
- 2.5
- 1.6
- 3.2
- 1.2
- A/P-COPmax (%)
- 3rd
- F
- 2.4
- 2.6
- 4.2
- 3.3
- 3.3
- 2.5
- 2.6
- 2.2
- 1.6
- 1.9
- 1.5
- 1.6
- 2.5
- 0.8
- S
- 2.3
- 1.8
- 3.5
- 2.8
- 2.7
- 3.7
- 3.1
- 3.2
- 5.5
- 4.4
- 2.5
- 1.2
- 3.1
- 1.1
- 4th
- F
- 1.5
- 3.4
- 1.4
- 4.3
- 3.3
- 2.1
- 2.0
- 1.9
- 2.1
- 1.6
- 1.9
- 1.0
- 2.2
- 1.0
- S
- 2.4
- 3.2
- 2.9
- 3.3
- 3.6
- 6.1
- 2.8
- 2.6
- 4.1
- 3.5
- 3.7
- 2.7
- 3.4
- 1.0
- 1st
- F
- 2.5
- 5.1
- 3.6
- 4.9
- 12
- 9.1
- 3.9
- 3.5
- 4.5
- 2.9
- 3.3
- 8.4
- 5.3
- 3.0
- S
- 1.9
- 5.2
- 5.1
- 4.2
- 5.5
- 11.4
- 1.2
- 5.7
- 2.9
- 6.9
- 8.5
- 3.0
- 5.1
- 2.9
- 2nd
- F
- 3.0
- 5.8
- 3.1
- 4.8
- 20
- 4.5
- 3.5
- 4.3
- 4.9
- 2.9
- 1.6
- 0.7
- 5.0
- 5.1
- S
- 3.2
- 4.0
- 3.8
- 5.4
- 5.5
- 12.1
- 3.2
- 6.9
- 9.8
- 6.9
- 8.3
- 3.0
- 6.0
- 2.9
- M/L-COPmax (%)
- 3rd
- F
- 3.2
- 3.4
- 7.9
- 5.1
- 0.9
- 2.9
- 4.2
- 2.6
- 3.5
- 0.9
- 2.3
- 2.6
- 3.3
- 1.9
- S
- 2.9
- 4.3
- 3.1
- 3.8
- 1.7
- 10.2
- 3.6
- 4.1
- 8.3
- 9.1
- 2.1
- 2.8
- 4.7
- 2.9
- 4th
- F
- 2.9
- 5.7
- 4.1
- 4.7
- 3.5
- 4.4
- 2.9
- 3.0
- 5.0
- 2.3
- 2.1
- 2.6
- 3.6
- 1.2
- S
- 4.0
- 3.0
- 3.7
- 5.9
- 2.2
- 2.8
- 3.8
- 4.3
- 3.9
- 13.8
- 10.6
- 2.0
- 5.0
- 3.6
- 1st
- F
- 9.4
- 15.5
- 7.3
- 11.2
- 10.4
- 11.6
- 9.1
- 10.4
- 5.7
- 6.1
- 8.0
- 11.2
- 9.7
- 2.7
- S
- 9.3
- 24
- 18.3
- 16.1
- 7.2
- 11.0
- 5.1
- 16.0
- 9.4
- 17.5
- 10.0
- 5.9
- 12.5
- 5.8
- 2nd
- F
- 7.0
- 7.5
- 9.7
- 10.9
- 12.1
- 14.0
- 9.9
- 9.3
- 8.3
- 9.2
- 6.4
- 5.4
- 9.1
- 2.4
- S
- 10.2
- 9.2
- 7.3
- 12.2
- 6.6
- 12.5
- 11.4
- 11.2
- 17.2
- 15.8
- 13.2
- 5.3
- 11.0
- 3.5
- A/P-COPtrajectory
- (%)
- 3rd
- F
- 7.2
- 8.1
- 3.6
- 8.5
- 7.1
- 8.7
- 8.9
- 8.5
- 7.1
- 7.5
- 6.4
- 6.1
- 7.3
- 1.5
- S
- 7.2
- 8.9
- 11.3
- 12.8
- 10.6
- 10.5
- 8.3
- 13.7
- 17.1
- 24.7
- 7.2
- 5.7
- 11.5
- 5.2
- 4th
- F
- 8.1
- 8.8
- 6.0
- 10.0
- 7.9
- 8.3
- 6.5
- 8.2
- 5.6
- 6.3
- 7.1
- 5.7
- 7.4
- 1.4
- S
- 7.1
- 9.9
- 6.9
- 15.9
- 9.3
- 9.9
- 6.3
- 9.7
- 5.3
- 12.2
- 14.7
- 8.3
- 9.6
- 3.3
- 1st
- F
- 4.6
- 10.3
- 4.4
- 6.1
- 7.2
- 10.1
- 4.3
- 4.8
- 5.9
- 3.0
- 5.6
- 10.8
- 6.4
- 2.6
- S
- 2.8
- 10
- 5.8
- 10.1
- 6.7
- 19.3
- 1.7
- 6.5
- 4.7
- 6.5
- 15.4
- 4.2
- 7.8
- 5.2
- 2nd
- F
- 4.0
- 5.4
- 2.8
- 7.2
- 5.1
- 6.2
- 5.0
- 4.8
- 3.8
- 4.3
- 3.5
- 1.5
- 4.5
- 1.5
- S
- 5.4
- 6.0
- 5.9
- 5.1
- 8.0
- 5.0
- 6.1
- 2.0
- 9.7
- 9.2
- 15.5
- 7.7
- 7.1
- 3.4
- M/L-COPtrajectory
- (%)
- 3rd
- F
- 3.4
- 6.9
- 3.3
- 5.8
- 1.6
- 5.3
- 4.6
- 4.2
- 5.6
- 1.8
- 2.9
- 3.9
- 4.1
- 1.6
- S
- 3.6
- 5.7
- 4.6
- 6.0
- 2.7
- 5.6
- 3.8
- 8.6
- 6.8
- 11.7
- 5.0
- 3.7
- 5.6
- 2.5
- 4th
- F
- 5.0
- 7.6
- 3.7
- 5.9
- 3.6
- 6.7
- 4.8
- 3.9
- 5.0
- 2.4
- 2.9
- 3.8
- 4.6
- 1.5
- S
- 5.6
- 5.1
- 3.2
- 6.8
- 2.5
- 5.8
- 3.4
- 6.1
- 3.3
- 14.8
- 16.3
- 3.2
- 6.3
- 4.5
- 1st
- 2
- 1
- 2
- 1
- 1
- 2
- 1
- 2
- 2
- 2
- 1
- 1
- 2nd
- 3
- 2
- 2
- 2
- 1
- 2
- 2
- 2
- 2
- 2
- 2
- 2
- 3rd
- 3
- 2
- 2
- 2
- 2
- 3
- 2
- 2
- 2
- 2
- 2
- 2
- 4th
- 3
- 2
- 2
- 2
- 2
- 3
- 2
- 2
- 2
- 2
- 2
- 3
- Type
Table 5: COP transition during trouser-wearing with eyes open.
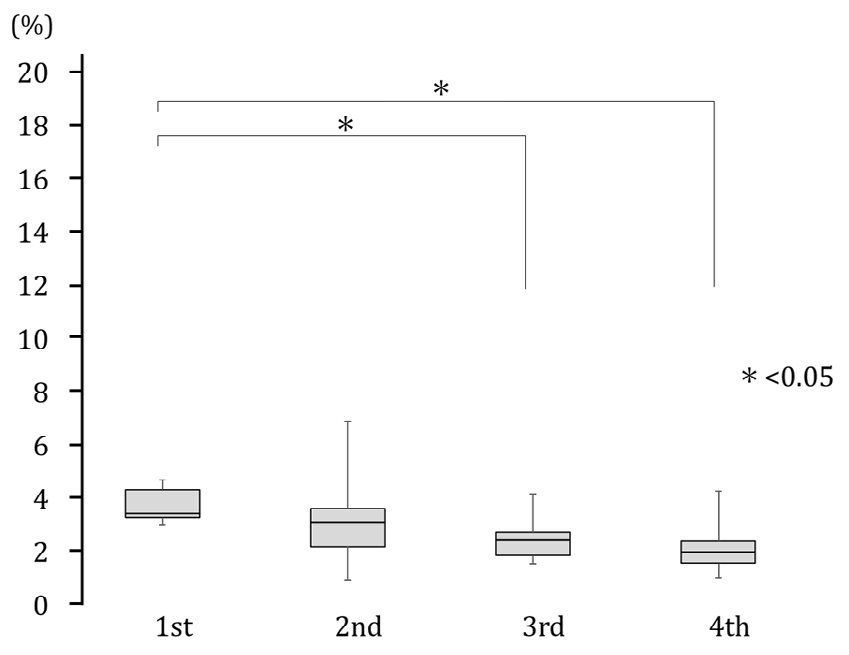
The COP transition during trouser wearing with eyes open was assessed after the first through to the fourth experimental task are shown in Table 5, Figures 2 to 4. The mean time required standing on the right and left foot was not significantly different between all tasks.
Regarding the A/P-COP-max during the trouser-wearing motion, the mean values of the FSL decreased significantly after the third and fourth experimental tasks compared to the first (p= .030, p= .024). However, there was no significant difference in A/P-COP-max in SSL. Regarding the M/L-COP-
max, the FSL and SSL mean values were not significantly different after the first through to the fourth experimental task.
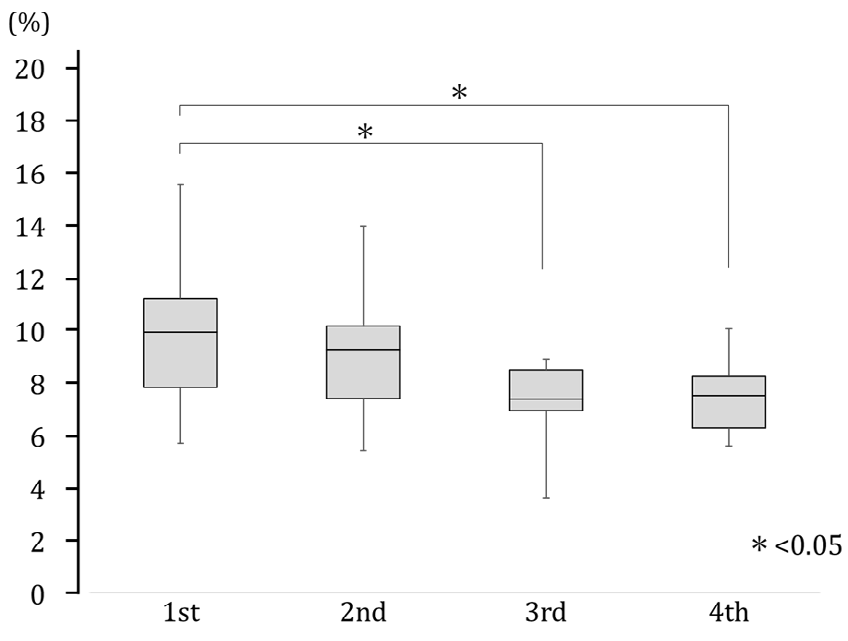
Regarding the A/P-COP-trajectory, the mean values of the FSL decreased significantly after the third and fourth experimental tasks compared to the first (p= .048, p= .024). However, there was no significant difference in the A/P-COP trajectories of the SSL.
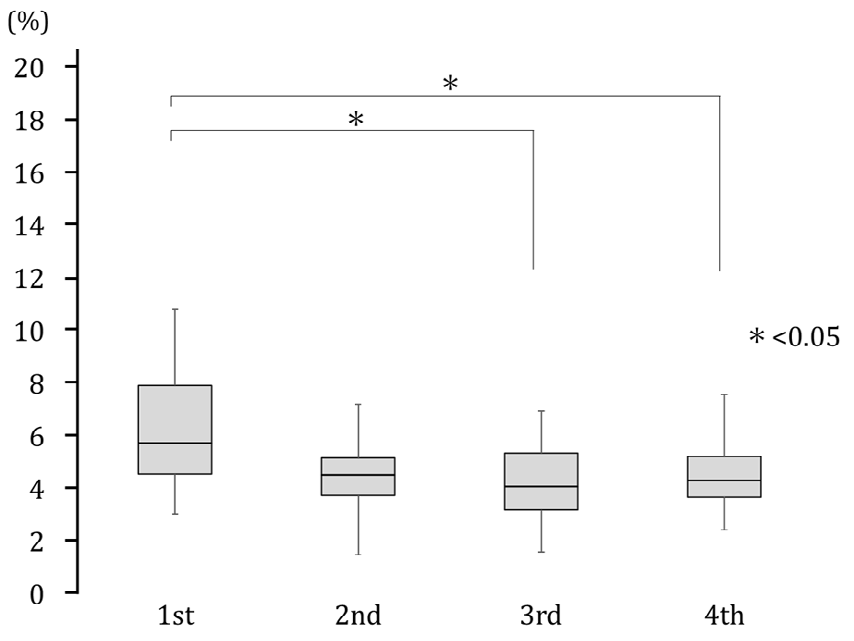
Regarding the M/L-COP-trajectory, the mean values of the FSL decreased significantly after the third and fourth experimental tasks compared to the first (p= .024, p= .048). However, there was no significant difference in the M/L-COP trajectories of the SSL.
The types of the first, second, third and fourth times are shown in (Table 5). The median number of OT interventions from the first to the second measurement was 3, from the second to the third measurement was 5, and from the third to the fourth measurement was 7. Five participants changed from type 1 to 2. Two participants changed from type 2 to 3. One participant changed from type 1 to 3. Four participants did not change their type during this period.
The trouser-wearing motion, foot pressure distribution, and COP at the first and fourth experimental tasks in Participant 1 are shown in (Figure 5). The type in Participant 1 changed from 2 to 3. Immediately after the FL left the floor (A and a), trunk bending was greater in the fourth task than in the first. The foot pressure distribution was similar; however, the pressure at the heel was stronger in the fourth. The COP of the first was located almost at the center of the foot, while that of the fourth was located at the heel. In the comparison of FL with maximal flexion (B and b), trunk bending was greater in the fourth than in the first task, and the foot of the FL was located at the height of the knee of the FSL. The foot pressure of the first experimental task was high in the first phalanx, and the COP was located in the second to the third metatarsal area. The foot pressure distribution of the fourth metatarsal area was high, and the COP was located in the fifth metatarsal area. A comparison of the initiation of FL extension (C and c) also showed greater trunk bending at the fourth task. The foot pressure was locally higher in the first phalanx, and the COP was located in the second to the third metatarsal area. The COPs were similar to those at the maximum flexion of the FL. For the comparison between D and d, the FL in the first task was held in position, and the trousers were pulled up with both hands. While pulling up the trousers with both hands in the fourth, the FL was extended and passed through the hem. In the first task, the foot pressure was high at the first phalanx, and the COP was located in the third metatarsal area. In the fourth task, foot pressure was high in the fifth metatarsal to the heel area, and the COP was located in the center of the foot. Comparing E and e, the motions of the first through to fourth were similar. The foot pressure of the first time was distributed over the entire foot, and the COP was almost at the center of the foot.
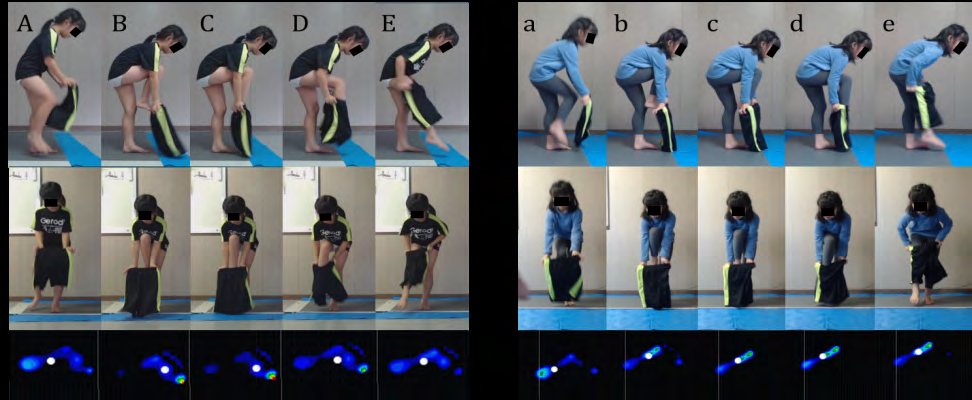
Figure 5: Photographic playback of trouser-wearing motion of participant 1 after the first and fourth OT interventions. The left pictures show the foot of first leg (FL) from the take-off to the landing after the first OT experimental task, whereas the right pictures show the same movements after the fourth OT experimental task. Top photos indicate the sagittal plane; middle, frontal plane; and bottom, foot pressure distribution and the COP of the first support leg (FSL). The dark blue color indicates a weak pressure, whereas the green color indicates a strong pressure. The white circles indicate COP. “A” and “a” show when the FL begins to move. “B” and “b” show when the foot of the FL has reached the waistbandof the trousers. “C” and “c” show the moment when the foot of the FL was inserted into the waistband of the trousers. “D” and “d” show the moment when the FL’s foot passes through the hem of the trousers. “E” and “e” show the moment just before the FL foot is placed on the floor. Abbreviation here are used in figure 6.
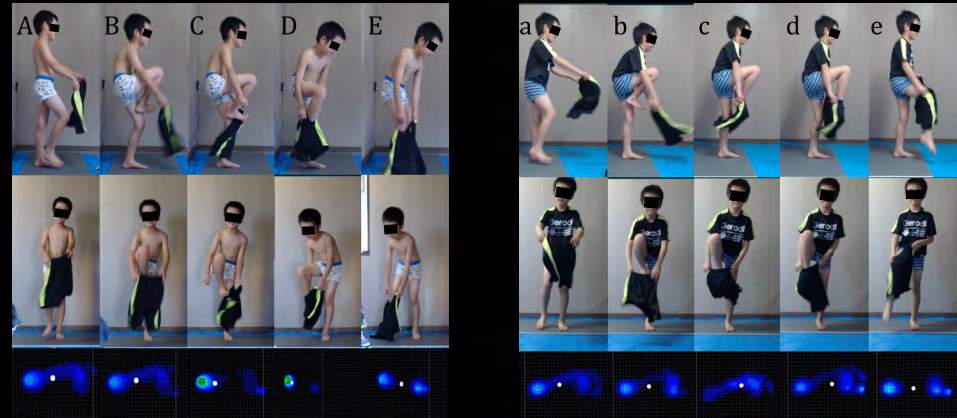
The trouser-wearing motion, foot pressure distribution, and COP at first through fourth experimental tasks in Participant 02 were shown in Figure 6. The type in Participant 02 changed from 1 to 2. Immediately after the release of the FL (A and a), there was greater forward bending of the trunk for the fourth. Both feet pressure distributions were slightly higher at the heel, and COP was almost at the center of the base of support of the FSL. The comparison in FL with maximal flexion (B and b) showed that while the trunk forward bending in the first was slight, it was greater in the fourth. The foot pressure distribution and COP of the fourth were not clearly different from the first, although trunk forward bending was greater. Comparing the initiation of FL extension (C and c), the first, the FL kicked the waistline of the trousers, and the right hand left the trousers because the ankle joint was not plantar flexed. In contrast, the fourth FL had ankle joint plantar flexion and was smoothly inserted into the trousers. The first foot pressure was high at the heel, and the COP was located near the heel. On the contrary, the foot pressure of the fourth time was distributed to the anterior and lateral sides of the sole, and the COP was located near the fourth and fifth metatarsal area. In the comparison of D and d, where the FL’s foot passed through the hem of the trousers, the first foot did not pass smoothly through the hem, resulting in trunk rotation. In contrast, the fourth, the waist position of the trousers was maintained with both upper extremities to smoothly pass the foot. In the first, the foot pressure was even higher at the heel, and the COP was at the heel. Contrastingly, the foot pressure of fourth was increased in the toe, but the COP was almost in the center of the foot. Comparing the first and fourth (E and e), the hand in the first execution left the trousers and the FL moved toward the floor. On the contrary, the leg of the FL smoothly passed through the hem of the trousers, and the trunk was extended in the fourth. Even though the motions were different, the foot pressure and COP at that time were similar.
Discussion
Previous studies have shown that postural sway during static standing in children with ASD was 438% greater on medial sway and 104% greater on anterior-posterior sway than in children with normal development [12]. At the onset of walking, there was no difference in the backward COP shift mechanism, suggesting that the mechanism that generates forward momentum is not impaired. However, children with ASD had a significantly smaller lateral COP shift, suggesting either instability or an alternative strategy for generating momentum in the medial direction. Furthermore, linear and nonlinear analyses of COP data were used to elaborate on abnormalities in postural control in children with ASD. The COP data of children with ASD showed more repetitive patterns and less complex postural control during static stance, suggesting regular or restricted postural control [13].
Upon standing on one leg, many children with ASD lose balance, starting from the lower trunk and pelvic area. Although the tonic and lax components of the trunk and lower extremity muscles of the participants in this study were not clear, postural and muscle tone problems were evident. Another report investigated the relationship between balance control and the diagnostic and symptom severity indices in children with ASD and their peers with typical development (TD) [12, 14, 15, 16]. They found that balance deficits in ASD were not associated with symptom severity and that in TDs, the duration of one-legged standing increased with increasing age [15]. The anterior–posterior and lateral components of COP during one-legged standing were smaller in participants aged 8-12 years than in those aged 4-7 years [17].
The median age of the participants in this study was 7 years and 1 month, and the median number of OT interventions was seven (3 months). The time to stand on one leg was not significantly different from the first to the fourth task on either side. This includes a ceiling effect because the target time for one-legged standing was set at 10 s based on the time required for the trousers-wearing motion, based on a previous study [11]. In addition, there was no noticeable change in excursion and trajectory length during the one- legged stand from the first to the fourth task. Therefore, these findings suggest that OT interventions in children with ASD were not related to improving the balance ability to stand on one leg. In addition, sensory sensitivity was the only result of the first evaluation. Therefore, its influence is unclear.
On the contrary, there was no significant difference in the time required to stand on one leg during the trouser-wearing motion from the first to the fourth experimental task for both sides. However, the A/P-COP-max and trajectory length of the FSL while standing on one leg during the trouser-wearing motion showed a significant decrease in the third and final (fourth) experimental task compared to the first. The median number of OT interventions performed before the third measurement was five. This suggests that approximately five OT interventions improved the balance ability in the anterior-posterior direction while standing on one leg in the trouser-wearing motion was improved. Since there was no significant difference in M/L-COP-max, the instantaneous medial-lateral sway when wearing trousers did not change. The participants in this study may have used a strategy to adjust the instantaneous COP sway with A/P-COP-max.
Contrastingly, the decrease in M/L-COP-trajectory length suggests that the ability to balance in the medial-lateral direction was also improved to some extent. In a previous study, the standing trousers-wearing motion characteristics of TDs were divided into three types [11]. Type 1 was more common in 4-year-olds, and type 3 was more common in 6-year-olds, indicating a relationship between the type of standing trousers-wearing motion and the developmental stage. In one-legged standing, the total time increased, and the path velocity, the A/P and M/L direction velocity and maximum displacement decreased as the type changing [11]. Type 1 had most of the children losing balance while standing on FSL. In contrast, type 3 had a good one-legged balance in both FSL and SSL. Type 2 showed characteristics between types 1 and 3, which were similar in children with ASD.
Moreover, 70% of the participants changed their type in the fourth experimental task (median; seven sessions of OT) compared to the first. This change is summarized in three points from the motion analysis. First, the stability of the trunk increased, and the participants were able to maintain the forward bending posture of the trunk during FSL. Next, the FL movement became easier, and it was easier to align the foot with the waist of the trousers. Finally, the waist of the trousers was able to firmly grasp both hands.
A resting-standing study compared the effects of SI therapy in children with ASD and TD and found an immediate effect of SI therapy, with a decrease in COP after the intervention [18]. One-legged standing, the subject of our study, is more challenging than resting standing. Nevertheless, there was a significant decrease in A/P-COP- max and A/P-COP-trajectory during one-legged standing in FSL in the third and final experimental tasks compared to the first time.
Therefore, these findings suggest that the three types of play added in the regular OT intervention program promoted changes in trousers-wearing motion in the standing position. Rolling the balance ball includes pushing and rolling the balance ball forward with both hands, as well as maintaining the trunk posture. This element is presumed to have improved the retention of trunk posture and the manipulation of trousers in that posture when passing the lower extremities through the trousers in a standing position. Walking on the lumber includes the elements of matching the foot of the swing leg to the width of the lumber and maintaining balance with the support leg to prevent falling on the floor. We speculate that this element controlled the COP of the support leg and improved control of the swing leg when passing the foot through the trousers in the standing position. The element of the tug of war is to pull the rope grasped with both hands in the direction of the body. These findings inferred that this element caused the child with ASD to grasp the waistline of the trousers tightly with both hands and pull it up in the direction of the body.
The framework for OT intervention was presented to a child with ASD by a therapist. The specific choices were then decided by the child with ASD. The therapist then adjusted the difficulty level to ensure that each play was successful. The therapist participated in the play with the child and was constantly involved in a supportive manner. Children with ASD were independently engaged in these activities. These OT interventions were conducted using play and SI theories [19].
These findings suggest that five sessions of play-based occupational therapy could be effective in improving standing trouser-wearing motion in children with ASD. Moreover, the effect of occupational therapy was not observed in each parameter of one-legged standing, suggesting the existence of task specificity.
Limitations of the Study
This study was conducted in addition to regular OT intervention. Therefore, there was no comparison between the ASD and control groups. In addition, the OT menu intervals and intervention frequencies of the participants differed. This was because additional interventions were performed during the participants’ regular OT menu. In the future, we would like to add an analysis using the ABA method to clarify the details.
Conclusion
Our findings suggest that five sessions of play-based OT could be effective in improving the standing trouser-wearing motion of children with ASD. Furthermore, the effect of OT was not observed in each parameter of one-legged standing, suggesting the existence of task specificity. Therefore, play- based OT interventions could be reflected in the specific training of activities of daily living.
Conflict of Interest
The authors declare that they have no conflict of interest.
Acknowledgements
The authors thank Dr. Reiko Tsuchida, president of The Japanese Academy of Sensory Integration, Prof. Kazumi Hirayama, Emeritus Prof. Shinji Satake, and Prof. Junko Goto for their valuable suggestions on this study. We also thank the staff of Kanon Co. Ltd., and the parents of the participants for their excellent assistance. Part of this paper was presented at the 54th Japanese Occupational Therapy Conference & Expo in Niigata, Japan, and the 55th Japanese Occupational Therapy Conference & Expo in Sendai, Japan. This works was partly supported by grants from the Yamagata Health Support Fundatuion.
Funding
Not applicable
References
-
Enjoji M, Gouya N (1977) The Enjoji scale of infant Analytical Development. Keio University Press, Japan.
-
Ueda R (1980) Denver Developmental Screening Test. Japanese Edition. Ishiyaku Publishers, Japan.
-
Fukuda E (2017) [Slowly developing children shine: A prescription for play] Yukkuri Hattatsu shiteiru Kodomo ga Kagayaku Asobi no Shohosen (in Japanese). CBR-Publishers, Japan.
-
Morikawa A, Ito K, Matsuda N, Morikawa S, Fujii H (2021) Occupational therapy program for children with autism spectrum disorder to improve trousers- wearing motion in the standing position. Annals of Physiotherapy & Occupational Therapy 4(4): 1-17.
-
Fidler SG, Velde PB (1999) Activities: Reality and symbol. SLACK Inco 61-79.
-
Dunkerley E, Tickle Degnen L, Coster WJ (1997) Therapist-child interaction in the middle minutes of sensory integration treatment. American Journal of Occupational Therapy 51(10): 799-805.
-
Pfeiffer BA, Koenig K, Kinnealey M, Sheppard M, Henderson L (2011) Effectiveness of sensory integration interventions in children with autism spectrum disorders: A pilot study. American Journal of Occupational Therapy 65(1): 76-85.
-
Tickle Degnen L, Coster W (1995) Therapeutic interaction and the management of challenge during the beginning minutes of sensory integration treatment. Occupational Therapy Journal of Research 15(2): 122- 141.
-
Tani I, Ito H, Hirashima T, Iwanaga R, Hagiwara T, et al. (2015) Standardization of the Japanese Version of the short sensory profile: Reliability and validity. Clinical Psychiatry 57(6): 419-429.
-
Tomchek SD, Dunn W (2007) Sensory processing in children with and without autism: A comparative study using the short sensory profile. American Journal of Occupational Therapy 61(2): 190-200.
-
Matsuda N, Kato K, Ito K, Morikawa A, Suzuki K, et al. (2021) Differences in the motion of typically developing children aged 4–6 years putting on trousers in a standing position. Yamagata J Health Sci 25.
-
Fournier KA, Kimberg CI, Radonovich KJ, Tillman MD, Chow JW, et al. (2010) Decreased static and dynamic postural control in children with autism spectrum disorders. Gait & Posture 32(1): 6-9.
-
Fournier KA, Amano S, Radonovich KJ, Bleser TM, Hass CJ (2014) Decreased dynamical complexity during quiet stance in children with autism spectrum disorders. Gait & Posture 39(1): 420-423.
-
Geuze RH (2003) Static balance and developmental coordination disorder. Human Movement Science 22(4- 5): 527-548.
-
Graham SA, Abbott AE, Nair A, Lincoln AJ, Müller RA, et al. (2015) The Influence of Task Difficulty and Participant Age on Balance Control in A.S.D. Journal of Autism & Developmental Disorders 45(5): 1419-1427.
-
Molloy CA, Dietrich KN, Bhattacharya A (2003) Postural stability in children with autism spectrum disorder. Journal of Autism & Developmental Disorders 33(6): 643-652.
-
Zumbrunn T, MacWilliams BA, Johnson BA (2011) Evaluation of a single leg stance balance test in children. Gait & Posture 34(2): 174-177.
-
Smoot Reinert S, Jackson K, Bigelow K (2015) Using posturography to examine the immediate effects of vestibular therapy for children with autism spectrum disorders: A feasibility study. Physical & Occupational Therapy in Pediatrics 35(4): 365-380.
-
Bundy AC (2002) Play theory and sensory integration. Sensory integration: theory and practice. 2nd (Edn.), F. A. Davis, Philadelphia, US.
- Electrolyte Considerations for Athletes
- Comprehensive Rehabilitation in Adults with Diabetic Peripheral Neuropathy: A Literature Review on Frequency, Intensity, and Duration Parameters
- Exercise Duration and Its Association with ADHD Symptom Severity in Children and Adolescents: A Parent-Reported Survey Study
- Adaptation of the Adult Neurophysiology of Pain Questionnaire for Use in Pediatrics
- A Non-Pharmacological Multidisciplinary Pain Program within a Hospital Wellness Program: A Mixed Methods Study
- The Effect of Frenkel's Exercise with PNF on Functional Reach in Stroke Survivors: A Randomized Control Trial