ADHD Symptoms in Children and Adolescents Improve with Longer Exercise Durations
Background: Attention deficit hyperactivity disorder (ADHD) is one of the most commonly diagnosed mental health disorders seen in children and adolescents (Center for Disease Control and Prevention [CDC]). The purpose of this study was to determine how various exercise durations were associated with ADHD symptoms among children and adolescents aged 6-17 with ADHD. Methods: The study used a quantitative, quasi-experimental non-equivalent control post-test only design. This sample was 199 parents of children and adolescents with ADHD. A one-way Analysis of Variance (ANOVA) was conducted to determine difference in ADHD symptoms measured by the ADHD Rating Scale-5 across three groups of different exercise durations. Results: The difference in ADHD symptoms among the exercise duration groups was statistically significant, F(2,196) = 6.48, p = .002. Post-hoc analysis revealed the high exercise group had lower ADHD mean score compared to the moderate exercise group, while the low exercise group did not differ significantly from the other groups. Conclusion: Further research is needed to look at other exercise parameters. Research should include a larger sample, more gender balanced groups, longitudinal study, more comprehensive assessment tools, classroom-based research, and qualitative research. Practically, exercise should be encouraged to help children and adolescents with ADHD lower their symptoms.
Introduction
Attention deficit hyperactivity disorder (ADHD) is one of the most commonly diagnosed mental health disorders seen in children and adolescents [1]. ADHD is characterized by developmentally inappropriate levels of inattention and distractibility and/or hyperactivity and impulsivity that cause impairment in adaptive functioning at school, home, or in social situations [2]. Children with ADHD have comorbidities such as oppositional defiant disorder (ODD), anxiety, and or depression [1]. The CDC reports that ADHD is a serious public health problem with costs over $30 billion annually in the United States to treat. The challenges of treating ADHD are vast due to the variations in symptoms and available options in the medical and psychological community.
ADHD affects an average of 5% of U.S. school-aged children, with reports as high as 9% [1]. The actual cause of ADHD is not known, but some theories include genetic and environmental factors [1]. ADHD can persist into adolescence and adulthood [3, 4, 5].
It is thought that comprehensive management can lead to improved long-term outcomes for children with ADHD [6, 7]. The current treatment of ADHD is medications and behavioral therapy interventions [4, 8]. These current treatment methods have limitations, as well as short-term lasting effects, thereby creating a need for alternative and complementary treatment for ADHD. Medications and behavioral therapy effects are limited in their ability to effectively treat all core symptoms. Another issue with these strategies is poor compliance by clients, which further limits the effectiveness of these treatment plans [4].
The American College of Sports Medicine (ACSM) [9] and the Center for Disease Control [1] have recommended that children and adolescents should complete aerobic or cardiorespiratory activities daily. The ACSM offers specific guidelines for children and adolescents of 60 minutes a day of accumulated physical activity, including physical education, sports, play, and transportation [9]. The CDC offers 60 minutes a day of moderate to vigorous aerobic activity three times a week, including muscle strengthening and bone-strengthening activities within those 60 minutes. The ACSM guidelines suggest that the activities should be developmentally appropriate, enjoyable to the individual, and have variety [9]. Similarly, the CDC suggests that the activities should be age-appropriate, enjoyable, and have variety. The CDC also recommends that young people are provided with opportunities and are encouraged to participate in physical activities. The ACSM suggests two to three times per week participation in muscle-strengthening activities such as jumping and or climbing activities, gymnastics, and or tumbling activities [9]. The ACSM also recommends that youths with disabilities or diseases should have their activity program specifically tailored to their needs. The CDC does not offer recommendations for physical activity for youths with disabilities or diseases.
Extensive literature supports the use of exercise for decreasing and managing ADHD symptoms [10, 11, 12, 13, 14]. There seems to be more support for aerobic-based exercise programs and activities [12, 13]. Despite the current research that supports exercise for the control of ADHD symptoms without the specific parameters, exercise cannot be prescribed as for type, intensity, and duration to be effective as an intervention [10, 11, 12, 14].
Objective
The purpose of the study was to determine which specific parameters of exercise duration were associated with lower ADHD symptoms.
Methods and Material
Population and Sample
The population was American children and adolescents ages 6 to 17 with a diagnosis of ADHD who were able-bodied and physically active. According to information from the CDC and the Health Resources and Services Administration, approximately 11% of school-aged children between ages 6 and 17 have been diagnosed with ADHD [1, 5]. The social media groups were found through the social medial site of Facebook by searching for parent groups of children with the diagnosis of ADHD.
Parents of children between the ages of 6 and 17 with a diagnosis of ADHD were recruited using a posting of a flier to Facebook groups for parent groups of children with the diagnosis of ADHD. Parents/guardians of these children and adolescents with ADHD were asked to voluntarily participate by completing a survey asking questions about their children’s exercise and ADHD symptoms if they met the inclusion criteria stated in the flier. The survey questionnaire was created and hosted on Qualtrics.
Using G*Power software, a priori analysis was computed to determine the minimum sample size needed for this study. Based on the planned analyses (F-test ANOVA of fixed effect, omnibus, one-way analysis using a coefficient of determination of 0.5, power of 0.8, and an effect size of 0.25), a total sample size of 159 was needed. This power analysis was based on ANOVA power of 0.8 choosing 5 groups.
This quantitative non-equivalent group post-test only design involved convenience non-probability sampling as the researcher had no control over choosing the participants. The inclusion criteria for participation were a parent/guardian with a child of 6 to 17 years of age with a diagnosis of ADHD. These parents/guardians and children and adolescents were from a mixed demographic and socioeconomic composition, largely from the northeast region of the United States. The sample initially involved parents of 215 children and adolescents (male and female) with the diagnosis of ADHD. These children and adolescents were able-bodied and capable of performing physical activity and exercise. These children and adolescents were attending school and were capable of participating in physical education and all school-related physical activities. The exclusion criteria for this study were children and adolescents with any medical condition, disability, and or comorbidity that would limit them from exercising.
Instrumentation
Participants who self-selected into the survey completed informed consent, screening items, demographic questionnaires, exercise questions, and the ADHD Rating Scale-5, a valid, reliable, and easy to administer questionnaire used to diagnose and evaluate children and adolescents with ADHD [15]. The scale is based on over 20 years of research and is linked to the DSM-5 criteria for diagnosing ADHD. The ADHD Rating Scale-5 is a 22-item questionnaire that addressed 2 topics in subsections. The exercise questions (Questions 1-4) focused on exercise habits, specifically the duration of exercise performed by the children and adolescents. The second subsection addressed ADHD symptom expression for the day.
The first section of questions was formulated by the researcher based on current literature in exercise science. Questions identified activities such as playing a sport, gym participation at school, any before or after recreation programs, group exercise classes, cardio equipment usage, and jogging, running, and or any other physical activity done for the purpose of exercising. Parents/guardians were asked to track their children’s exercise for a day, reporting the amount (minutes per day) and type (aerobic or anaerobic) of their children’s exercise. The second section of the survey was the questions from the ADHD Rating Scale-5, which was used with permission from the publisher [15]. This rating scale is a questionnaire based on home behaviors that are keyed to the DSM-5 diagnostic criteria that takes 5 minutes to complete. Both sections of the survey in combination took approximately 5 minutes to complete one of two formats: child version (5-10 years old) or adolescent version (11-17) [15]. Both versions were provided, and the parent/guardian used the appropriate one for their child or adolescent depending on their age.
Method and Design
A quantitative quasi-experimental research method and non-equivalent control post-test only design was used to determine how ADHD symptoms compare across exercise groups. The use of survey methodology was implemented to gather the data on exercise and ADHD symptoms. The independent variable of exercise duration was not imposed on the subject; rather, data were collected on the amount of exercise performed by the children and adolescents via self- report reported by parents and or guardians.
The independent variable was duration of exercise, grouped by the amount of exercise in minutes of participation per day. The amount of exercise the child performed each day was tracked by parents and was put into equivalent groups of exercise depending on times reported. After the data were collected, three groups of exercise durations were compiled. The groups were as follows: (a) Group 1: 0-60 minutes, (b) Group 2: 61 to 120 minutes, (c) Group 3: 121 thru 180 minutes. These groups were arranged due to the exercise times reported back in the survey, and the current literature on recommendations for exercise times. The dependent variable evaluated was the totality of symptoms of inattention, hyperactivity, and impulsiveness in those with ADHD, in which an overall score for symptoms was obtained. The exercise parameters and outcomes of ADHD symptoms were measured with the use of survey research in which well-designed questions were answered about the exercise duration performed for a day and those from the ADHD Rating Scale-5. The results were analyzed to compare the variables to determine how ADHD symptoms compare across exercise groups of varying time frames. The target population was parents of children between the ages of 6 and 17 with the diagnosis of ADHD.
Those questionnaires fully completed were collected and were tabulated for all responded items. There was a total of 10 questionnaires not complete and not used in the data collection. The independent variable of amount of exercise was grouped into three exercise durations and compared to the dependent variable of ADHD symptoms to see the association. ANOVA was used to determine how ADHD symptoms compared across the different exercise groups. The exercise groups were based on time frames in minutes of exercise performed. Thus, ANOVA results were used to assess a potential difference between the means of the independent variables of exercise groups with regard to the dependent variable (difference in ADHD symptoms for each).
Study Procedures
The investigator posted a flier with a link to the informed consent and survey to Facebook for parents/guardians of children and adolescents with ADHD. The survey started with screening questions to assure that all participants met inclusion criteria. Demographic data were collected on all participants, including race, education level, age, and marital status of parent/guardian. Once the demographic questions were answered, the survey questions appeared with instructions on answering the questions about exercise and ADHD symptoms for a day.
The completed surveys were retrieved from Qualtrics and analyses in Statistical Package for the Social Sciences (SPSS 26). Data cleaning took place by looking at the data in order to detect errors, inconsistencies, or unanswered items through the Qualtrics software program. The independent variable was the duration of exercise in minutes of time per a day. After the data were collected, the duration of exercise was grouped into 3 semi-equivalent duration groupings. The groups were determined after the data were collected to ensure each group had similar number of participants.
Descriptive statistics, frequencies, and outlier detection
were used to assure the data were approximately normal as described above. Surveys with missing data were eliminated, and the exercise duration was coded and grouped into three groups of semi-equivalent duration groupings of time frames. The 3 groups of exercise based on duration were low (0-60 minutes), moderate (61-120 minutes), and high (120- 180 minutes; see (Table 1). These groups were arranged due to the exercise times reported back in the survey, and the current literature on recommendations for exercise times. There was exercise time reported over 180 minutes and up to 820 minutes per day. These higher exercise times over 180 minutes consisted of 16 participants who were eliminated, as it was thought that these might be exaggerated exercise times reported or were simply outliers. The data from a total of 199 participants, after the higher exercise times were eliminated, were used for analysis.
| Dependent Variable: Score | |||
|---|---|---|---|
| Exercise groups | Mean | Std. Deviation | N |
| 0-60 | 42.31 | 17.13934 | 62 |
| 61-120 | 49.26 | 22.46965 | 105 |
| 121-180 | 35.34 | 18.14033 | 32 |
| Total | 44.85 | 20.83615 | 199 |
Table 1: Descriptive Statistics: Exercise Groups.
Bonferroni post-hoc tests were used to answer further questions on the difference between the exercise groups. Specifically identifying which group of exercise duration is associated with the lowest ADHD symptoms, Bonferroni post-test was appropriate as the F score was significant, indicating that there was a difference between the exercise groups.
Results
The survey sample consisted of 215 parent/guardian participants who were asked questions regarding their children’s exercise and ADHD symptoms. The subjects ranged in age from 18 to 75 with the 25-34 age group being the largest (n = 84, 39.1%). As listed in Table 2, subjects were mostly White (n = 75, 34.9%) with Asian as the second largest group (n = 69, 32.1%). Most of these parents/guardians reported they were married or resided with a domestic partner (n = 123, 57.2%). The highest education level was a bachelor’s degree (n = 76, 35.3%) with the master’s degree coming next (n = 32, 14.9%) and some college being the third (n = 24, 11.2%). Data on gender of the children and adolescents was not collected. All the demographic information is provided below in (Table 2).
| Marital Status | Total sample (%) | ||
|---|---|---|---|
| Single, never married | 38 | 17.7 | |
| Married or domestic partnership | 123 | 57.2 | |
| Divorced | 5 | 2.3 | |
| Separated | 2 | 0.9 | |
| Did not answer | 47 | 21.9 | |
| Education | |||
| Nursery school to 8th grade | 1 | 0.5 | |
| Some high school, no diploma | 2 | 0.9 | |
| High school graduate, diploma or the equivalent | 13 | 6 | |
| Some college credit, no degree | 24 | 11.2 | |
| Trade/technical/vocational training | 3 | 1.4 | |
| Associate degree | 7 | 3.3 | |
| Bachelor’s degree | 76 | 35.3 | |
| Master’s degree | 32 | 14.9 | |
| Professional degree | 8 | 3.7 | |
| Doctorate degree | 2 | 0.9 | |
| Did not answer | 47 | 21.9 |
Table 2: Demographic Characteristics of Parent/Guardian.
A one-way ANOVA was conducted to determine if ADHD symptoms measured by the ADHD Rating Scale-5 were different for groups of different exercise durations. Participants were classified into three groups of exercise duration: low (n = 62), moderate (n = 105), and high duration of exercise (n = 32). There were no outliers, as assessed by boxplot for values greater than 1.5 box-lengths from the edge of the box; data were normally distributed for each group, as assessed by Shapiro-Wilk test (p > .05); and there was homogeneity of variances, as assessed by Levene’s test of homogeneity of variances (p = .126).
ADHD score increased from the low exercise duration (n = 62, M = 42.3, SD = 17.1), to moderate exercise duration (n = 105, M = 49.3, SD = 22.5), and decreased from moderate to high exercise duration (n = 32, M = 35.3, SD = 18.1). The difference between the exercise duration groups was statistically significant, F(2,196) = 6.48, p = .002.
| Sum of Squares | df | MS | F | p | Observed Powerb | |
|---|---|---|---|---|---|---|
| Corrected Model | 5332.321a | 2 | 2666.16 | 6.481 | 0.002 | 0.903 |
| Intercept | 283034.618 | 1 | 283035 | 688.03 | 0 | 1 |
| Exercise Groups | 5332.321 | 2 | 2666.16 | 6.481 | 0.002 | 0.903 |
| Error | 80628.453 | 196 | 411.37 | |||
| Total | 486330 | 199 | ||||
| Corrected Total | 85960.774 | 198 |
Table 3: ** ANOVA Results: Exercise groups and ADHD score.
R Squared = .062 (Adjusted R Squared = .052) Computed using alpha = .05 Table 3: ANOVA Results: Exercise groups and ADHD score.
There was an increase in the ADHD score from the low exercise duration group (M = 42.3, SD = 17.1) to the moderate exercise duration group (M = 49.3, SD = 22.5), which was not statistically significant. Bonferroni post hoc analysis Table 4 revealed that there was a statistically significant difference in ADHD score from the moderate exercise duration group (M = 49.3, SD = 22.5) to the high exercise duration group (M = 35.3, SD = 18.1) with a mean decrease of 14, 95% CI [4.0, 23.8], which was statistically significant (p = .002). No other group differences were statistically significant. The group means were statistically significantly different (p < .05). Therefore, the null hypothesis was rejected, and the alternative hypothesis was accepted.
| for header rows | for data cells | for header rows | for data cells | for header rows | for data cells | |
|---|---|---|---|---|---|---|
| (I)Exercise | (J)Exercise | MD(I-J) | Std. Error | Sig | Lower Bound | Upper Bound |
| 0-60 | 61-120 | -6.95 | 3.25 | 0.101 | -14.79 | 0.89 |
| 121-180 | 6.96 | 4.41 | 0.349 | -3.7 | 17.62 | |
| 61-120 | 0-61 | 6.95 | 3.25 | 0.101 | -0.89 | 14.79 |
| 121-180 | 13.91* | 4.1 | 0.002 | 4.05 | 23.8 | |
| 121-180 | 0-61 | -6.96 | 4.41 | 0.349 | -17.62 | 3.7 |
| 61-120 | -13.91* | 4.1 | 0.002 | -23.8 | -4.02 |
Table 4: Multiple Comparisons of dependent variable of ADHD score: Bonferroni Post Hoc Tests. Based on observed means. The error
Discussion
The overall study was to determine the specific parameters of exercise duration that were most strongly associated with lower ADHD symptoms. The exercise group of 121-180 minutes was most associated with lower reported ADHD symptoms. Bonferroni post-hoc tests were used to answer further questions on the difference between the exercise groups. Specifically identifying that exercise duration of high exercise duration of 121-180 minutes was most significantly different in association with ADHD score symptom means when compared to the moderate exercise duration group.
The results in this study of the high exercise duration group having lower ADHD symptom scores when compared to the low exercise duration group had no statistical significance. The moderate exercise duration group did not have a significant difference from the low exercise duration group as well. The statistically significant result of the high exercise group associated with lower ADHD scores when compared to the moderate exercise duration suggests that longer exercise duration may be better to lower ADHD symptoms. The difference in ADHD scores from the low to moderate to high exercise duration in this study did not follow what would be expected in a relationship with lowering ADHD scores as exercise time increased.
This study is partially in alignment with many findings in the literature that exercise is beneficial in helping control ADHD symptoms in children and adolescents. The research and literature designate different durations of exercise, with most showing positive results in lowering ADHD symptoms, and longer durations having best positive results [13, 14, 16, 17]. There is still not a lot of evidence for the best duration of exercise to be effectively used in exercise intervention in children and adolescents with ADHD. Yet, previous research has focused prominently on exercise durations under the 1.5-hour (90 minute) mark, showing significant decreases in ADHD symptomology associated with more exercise. The current study showed no change in symptomology between the low to mid group, which conflicts with previous findings. In other words, there was no association between more exercise and lower ADHD symptomology except within the high exercise duration group (120-180 minutes). In addition to finding no decrease in ADHD symptomology between the low and moderate duration groups, the current study suggested that longer exercise durations may be needed to reduce ADHD symptomology.
Researching exercise effects on ADHD symptoms in children and adolescents is not an easy task as there are many variables that cannot be controlled. These confounding variables that cannot be controlled are factors that may influence the results. Confounding variables include types of ADHD, medications, other therapies, type of exercise, and intensity. Of course, individual differences may exacerbate the complexity of covarying influences as children and adolescents vary to greater or lesser degrees in their types of ADHD (e.g., degree of impulsivity or hyperactivity), medications (e.g., type, dosage), therapy (e.g., type, frequency), type of exercise (e.g., cardiovascular versus strength training), and intensity (e.g., heart rate and oxygenation capacity). Still, other individual variables such as nutrition, sleep, home environment, and several other socioeconomic factors are likely to differentially affect how exercise may relate to ADHD symptomology. Such individual factors and potential covariates underscore the importance of not making causal assumptions based on the findings.
The children and adolescents were not asked to stop medication and or other therapies in this study, which could have influenced the findings as medications and or other therapies could have been related to lower symptoms [18]. Another factor that may have influenced the results was the time of day the exercise was performed. Not much is known on how the time of day performing exercise may impact ADHD symptoms [12]. This study did not involve collection of data on the time of day the exercise was performed which may have impacted the results. It is necessary to stipulate that differences in ADHD symptomology were not necessarily due to exercise. For example, while exercising, the potential interaction of exercise with other variables such as Vitamin D exposure cannot be determined with the data collected. Thus, the findings should be understood amidst the study limitations.
It is possible that the longer durations of exercise could have been lower intensity, and the types of exercises may be considered easier to perform. Potentially, the shorter durations could have been higher intensities of exercises that were more difficult. Both of these possible situations could have influenced the results. This was not a pre/post design study, so it is feasible that those children and adolescents may have self-selected into exercise groupings based on their symptomology. Those with lower ADHD symptoms may have been exercising for longer durations due to the ability to sustain attention longer. Those children and adolescents with higher ADHD symptoms may find it more difficult to sustain exercise for moderate or high durations due to difficulty focusing attention and staying on task [19]. It is possible that the participants with already lower ADHD symptoms exercise longer. It is also possible that the children and adolescents with lower ADHD symptoms exercised less which would fit with the conclusion of longer exercise durations having greater impact on reducing symptoms in those children and adolescents with higher symptoms.
As previously stated, it is difficult to explain the reason that ADHD symptoms increased from low to moderate durations, despite not being a statistically significant difference. Whereas previous studies showed a reduction in symptoms as duration of exercise increased, the current study found no such decrease. ADHD symptomology appeared to increase as exercise duration increased, although this study supports more research with longer exercise times, specifically because there was not a statistically significant increase in ADHD symptoms between low exercise duration (0-60 minutes) to moderate exercise duration (61-120 minutes), indicating that it may not be a dose-related effect, wherein more exercise would have a greater effect on lowering symptoms. A possible explanation could be that exercise at low to moderate durations may exaggerate ADHD symptoms, whereas longer durations of exercise may help a child or adolescent overcome their initial arousal from exercise and begin to experience some relief or reduction of their symptoms. Thus, it is possible that high exercise of 121 to 180 minutes could lower ADHD symptoms due to exhaustion of the child or adolescent, leading to fewer symptoms. Of course, there is the aforementioned possibility that those children and adolescents with lower ADHD symptoms may be more likely to complete longer exercise durations due to better focus, attention, and ability to complete tasks.
Existing literature confirms that exercise has positive effects on ADHD symptoms of hyperactivity, inattention, and impulsivity, as well as improvement in cognition, working memory, and improved peer relations [10, 12, 14, 20]. Although this study aligns with the existing literature in essence regarding ADHD symptom decreases associated with longer exercise, the lack of change in ADHD symptoms between the low and moderate groups raised new questions about a potential dose-related effect. Future research should further investigate how ADHD symptomology may be potentially heightened (or engaged) due to initial arousal of exercise. Research should also investigate neurophysiological underpinnings of symptomology during exercise across time, controlling for individual factors (e.g., average intensity of ADHD symptoms for the individual child). Just as exercise could initially arouse and increase ADHD symptoms, physical exhaustion due to longer exercise durations could play a role in calming physiological arousal. It is unclear what effect physiological calming (e.g., due to physical tiring) could have on the ability of a child with ADHD to enhance their cognitive focus and, ultimately, improve their academic success. The potential for exercise to arouse or engage, rather than reduce, ADHD symptomology is surprising given a previous linear assumption, wherein ADHD symptoms decreased as exercise duration increased.
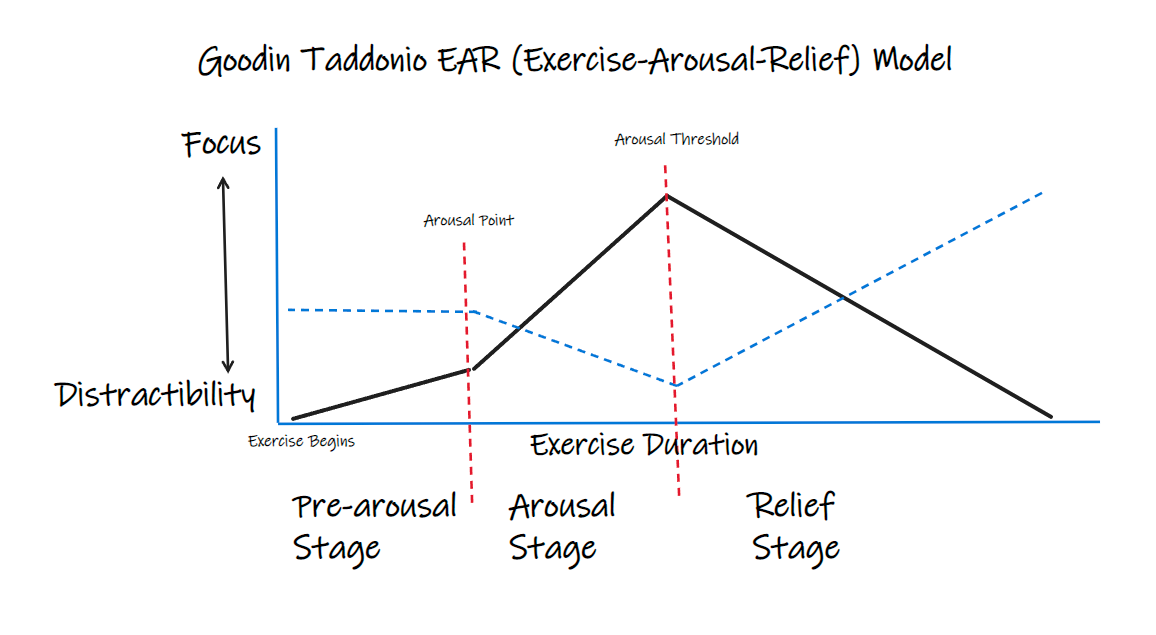
The complex relationship of exercise with symptomology cannot be simply explained by a premise that ADHD symptoms are aroused or engaged during exercise because of the lower amounts of symptomology in the low exercise duration group. Figure 1 illustrates an initial model depicting the theorized progression of Focus and ADHD symptomology across time during exercise. Perhaps, as depicted in our model, lower amounts of ADHD symptoms in the low group were due to not engaging ADHD distractibility fully, such that there may be an “arousal point” during exercise before which symptoms remain at baseline and, after which, symptoms are aroused or exacerbated. Perhaps their symptoms increase in relation to psychophysiological factors, such that they experience emotional excitement and physiological arousal. With continued exercise (i.e., longer duration), a child or adolescent may reach a second duration point that could mark an “arousal threshold” sufficient for exhausting their “excess” arousal and begin to experience some relief or reduction in symptoms by extinguishing overstimulation related to their ADHD. Thus, the midgroup could have gotten enough play and exercise to activate some ADHD triggers per the upward trend from low to mid. Field practitioners might say the children and adolescents at this threshold or duration of exercise have successfully achieved “getting their wiggles out.” The high exercise duration group may have actually shown the benefit of exercise eventually having a “taming” effect on ADHD symptoms after the child is worn out, perhaps. In reaching and surpassing their arousal threshold, the child or adolescent may benefit from greater emotional and cognitive regulation, mitigating distractibility and impulsivity, while allowing greater focus and attention on foci of need (e.g., academic tasks).
Although no causal assumptions can be made from the findings of the current study, it could be that allocating higher durations of exercise for those with ADHD may be worthy of further consideration in interventions to help lower ADHD symptoms. The relationship between exercise duration and ADHD symptomatology in the current study suggests the potential that exercise could be a mitigating factor in ADHD symptoms. With fewer ADHD symptoms, children and adolescents may be more successful in school, have better relationships, and better self-regard [4]. Exercise can easily be implemented into the day of a child or adolescent, and it is recommended for improving overall health. Exercise has been shown to help lower ADHD symptoms in several studies. [7, 20, 21, 22].
Several limitations and considerations are noteworthy in understanding the value of the findings and implications for future research. One factor that might have influenced the interpretation of the results was the methods and design chosen to conduct this study. This study was a quantitative non-equivalent group post-test only design that used a grouping independent variable of exercise durations to compare the dependent variable of ADHD symptoms across these groups. By nature of this type of study that collected data post-test only, the ADHD scores could not be compared to pre-test (baseline) scores to determine if the intervention of exercise was what caused any change. Also, the post- test data collected in this study were grouped durations of exercise (low, moderate, and high time frames) that were compared to each other, which could have obscured specific times of exercise that may have been more associated with lower ADHD symptoms.
With regard to the sample, other issues are worthy of note with respect to the value and meaning of the findings. Although the sample size met the appropriate power analysis for a one-way ANOVA, a larger sample size could provide a greater effect or a more accurate representation of the relationships between variables [23]. The use of a second party survey (parent report of child behavior) could have influenced the results of this study as it relies on parent perception and estimation, rather than recorded observations of the activity. Parents may have asked their child to report their daily exercise, potentially resulting in inaccurate reports. Observing the activity of each child and timing the activity in vivo could have provided more accurate and different results. In terms of presentation bias, parents may have tried to answer survey questions in ways that made their children appear healthy and appropriate to what they perceived their child could be doing. For example, if the parent believed the researchers would be impressed by a longer duration of exercise, the parent may have been inclined to inflate the amount of exercise time reported, whether consciously or subconsciously.
Recommendations for Future Research
Although this study strictly analyzed ADHD symptoms across grouped exercise times of different durations, the findings support past research that asserts more exercise is beneficial in lowering ADHD symptoms [16, 17]. This study found that the high exercise group of 121-180 minutes of exercise was associated with lowest ADHD symptoms. This implies that exercise might be considered as a tool for intervention in children and adolescents with ADHD to help control their symptoms. The efficacy of duration for mitigating ADHD symptomatology requires further research.
The study’s imitations were the method of data collection, parents answering about their child’s exercise, data collection on duration of exercise only, and lack of control of extraneous variables. Given the limitations in this study, further research should consider collecting data on types of exercise, intensity of exercise, time of day performed, and how long after the exercise was the ADHD symptoms assessed. Further research should also be done with more specific time frames, including higher than previously reported durations of exercise. Other methods of data collection should also be considered, including tracking of exercise and physical activity through true experimental conditions with pre- and post-testing of ADHD symptoms, including control groups for comparison. This would allow for a more robust study with the ability to have specific exercise parameters to determine which are the most effective at lowering ADHD symptoms.
Research is needed to investigate the most effective types of exercise, as well as optimal duration, frequency, and intensity of exercise to ascertain improvements in the symptoms of ADHD. Further recommendations for future research include increasing the sample size, developing a more longitudinal study, choosing comprehensive assessment tools, and collecting qualitative data.
Conclusion
ADHD is a chronic neurological diagnosis with symptoms of inattention, hyperactivity, and impulsivity. Children and adolescents diagnosed with ADHD suffer great consequences that affect academics, social skills, and mental health [4]. Exercise can be an alternative option to medications and can be helpful in controlling ADHD symptoms [20, 24, 25]. Currently, there are still no exact parameters of exercise (time, duration, intensity, and type) identified that are considered optimal for use in intervention in the treatment of ADHD in children and adolescents. This study was important in that it found support of previous research findings on exercise use to lower ADHD symptoms specifically longer exercise durations, however, the lack of clarity in the findings strongly supports further research on this topic to find the optimal parameters. Further research that provides understanding of how specific parameters of exercise associated with lower ADHD symptoms could provide better ability to plan and implement programs and interventions to assist children and adolescents with ADHD lower the symptoms and lead more successful life.
Competing Interest
The authors declare that they have no competing interests.
References
-
Center for Disease Control and Prevention (2019).
-
American Psychological Association (2019).
-
Elizabeth A, Micah S, Joy TL (2017) Interventions for ADHD in children and teens: A focus on ADHD coaching. Pediatric Nursing 43(3): 121-131.
-
Children and Adults with Attention-Deficit/Hyperactivity Disorder (CHADD) (2019).
-
Health Resource and Service Administration (2019).
-
Pontifex MB, Saliba BJ, Raine LB, Picchietti DL, Hillman CH (2013) Exercise improves behavioral,
-
neurocognitive and scholastic performance in children with attention-deficit/hyperactivity disorder. The Journal of Pediatrics 162(3): 543-551.
-
Rassovsky Y, Alfassi T (2019) Attention improves during physical exercise in individuals with ADHD. Frontiers in Psychology 9(1): 1-9.
-
Danielson ML, Bitsko RH, Ghandour RM, Holbrook JR, Kogan MD, et al. (2018) Prevalence of Parent-Reported ADHD Diagnosis and Associated Treatment among U.S. Children and Adolescents. Journal of Clinical Child and Adolescent Psychology 47 (2): 199-212.
-
American College of Sports Medicine (2019).
-
Archer T, Kostrzewa RM (2011) Physical exercise alleviates ADHD symptoms: regional deficits and development trajectory. Neurotox Research 21(2): 195- 209.
-
Cerrillo UAJ, García HA, Sánchez LM, Pardo GMJ, Santos Gómez JL, et al. (2015) The effects of physical exercise in children with attention deficit hyperactivity disorder: a systematic review and meta-analysis of randomized control trials. Child: Care, Health & Development 41(6): 779-788.
-
Den Heijer AE, Groen Y, Tucha L, Fuermaier AB, Koerts J, et al. (2017) Sweat it out? The effects of physical exercise on cognition and behavior in children and adults with ADHD: A systematic literature review. Journal of Neural Transmission 124(l 1): 3-26.
-
Matuszewich L (2018) A look at effects of stimulant treatment on ADHD. Psychology Today.
-
Reale L, Bartoli B, Cartabia M, Zanetti M, Costantino MA, et al. (2017) Comorbidity prevalence and treatment outcome in children and adolescents with ADHD. European Child & Adolescent Psychiatry 26(12): 1443- 1457.
-
DuPaul GJ, Power TJ, Anastopoulos AD, Reid R (2016) ADHD rating scale-5 for children and adolescents: Checklists, norms, and clinical interpretation. The Guilford Press, pp: 126.
-
Berger NAA, Müller A, Brähler E, Philipsen A, Zwaan DM (2014) Association of symptoms of attention-deficit/ hyperactivity disorder with symptoms of excessive exercising in an adult general population sample. BMC Psychiatry 14(1): 1-9.
-
Gonzalez VR, Heredia VL, Crespo I, Valle DM, Olmedillas H (2020) A systematic review of acute exercise as a coadjutant treatment of ADHD in young people. Psicothema 32(1): 67-74.
-
Manzano SS, Ariza RA, Cruz DLTM, López MEJ (2018) Acute and chronic effect of physical activity on cognition and behavior in young people with ADHD: A systematic review of intervention studies. Research in Developmental Disabilities 77(1): 12-23.
-
Giorgio DA, Kuvacic G, Milic M, Padulo J (2018) The brain and movement: How physical activity affects the brain. Montenegrin Journal of Sports Science & Medicine 7(2): 63-68.
-
Bowling A, Davison K, Haneuse S, Beardslee W, Miller DP (2017) ADHD Medication, Dietary Patterns, Physical Activity, and BMI in Children: A Longitudinal Analysis of the ECLS-K Study. Obesity 25(10): 1802-1808.
-
Grassmann V, Alves MV, Galduróz SRF, Galduróz JCF (2017) Possible Cognitive Benefits of Acute Physical Exercise in Children With ADHD: A Systematic Review. Journal of Attention Disorders 21(5): 367-371.
-
Powell L, Parker J, Harpin V (2018) What is the level of evidence for the use of currently available technologies in facilitating the self-management of difficulties associated with ADHD in children and young people? A systematic review. European Child & Adolescent Psychiatry 27(11): 1391-1412.
-
Gillard J (2020) One-Way Analysis of Variance (ANOVA). In A First Course in Statistical Inference. Springer, pp: 91-101.
-
Ng QX, Ho CYX, Chan HW, Yong BZJ, Yeo WS (2017) Managing childhood and adolescent attention- deficit/hyperactivity disorder (ADHD) with exercise: A systematic review. Complementary therapies in medicine 34 (1): 123-128.
-
Vysniauske R, Verburgh L, Oosterlaan J, Molendijk ML (2020) The effects of physical exercise on functional outcomes in the treatment of ADHD: a meta-analysis. Journal of Attention Disorders, 24(5): 644-654.
- Electrolyte Considerations for Athletes
- Comprehensive Rehabilitation in Adults with Diabetic Peripheral Neuropathy: A Literature Review on Frequency, Intensity, and Duration Parameters
- Exercise Duration and Its Association with ADHD Symptom Severity in Children and Adolescents: A Parent-Reported Survey Study
- Adaptation of the Adult Neurophysiology of Pain Questionnaire for Use in Pediatrics
- A Non-Pharmacological Multidisciplinary Pain Program within a Hospital Wellness Program: A Mixed Methods Study
- The Effect of Frenkel's Exercise with PNF on Functional Reach in Stroke Survivors: A Randomized Control Trial