Current and Future Challenges for Vaccine Development Especially COVID-19
Global health has been greatly impacted by vaccines. Smallpox, rinderpest, and several other major infections have been eradicated. A variety of infectious diseases of childhood have been significantly improved by whom in the past decade. As polio has been virtually eradicated, and measles has been controlled successfully, it may also be eradicated soon. Vaccines can prevent infections such as pneumonia and diarrhoea which cause 6.6 million deaths each year. Due to new pneumococcal conjugate vaccines and rotavirus vaccines, childhood mortality is expected to decline further. As of now, malaria, tuberculosis, and HIV vaccines have had modest success. Vaccinations that stimulate different immune systems and it may be the most effective way to prevent these infections. On a long-term basis, vaccines may prevent or modulate diseases other than infectious diseases. It is already possible to develop cancer vaccines, and in the future it will be possible to develop vaccines for addictions, diabetes, hypertension, and Alzheimer's disease as well.
Yousaf Khan1*, Zia-Ur-Rehman2, Hakimullah3, Abdul Sattar1, Syed Amin Ullah1, Madeeha Bibi4 and Saifuddin5
Introduction
As the greatest human intervention other than clean water and sanitation, vaccination is often cited as the greatest. Infectious diseases have declined significantly and gradually in industrialized countries between the end of the nineteenth century and the present, as a result of a decrease in infectious disease mortality prior to the development and implementation of vaccines. Furthermore, improvements in housing, nutrition, and sanitation were associated with improvements in health. The health of humans and animals has undoubtedly been benefited by vaccination, especially in developing countries. During epidemics, almost half the population died from smallpox and measles. Measles was only slightly less deadly than smallpox. It describes some of vaccination’s major accomplishments, how vaccines are used globally today, and how vaccination could help global health in the future.
Global Immunization’s Current Challenges
In the context of vaccines, there have been a number of ongoing complications. Vaccine advancements, such as the expansion of primitive EPI vaccinations and the recent acknowledgement of vaccines in less developed countries, are likely to have an infinite impact on global health. They are expected to have a significant influence in particular areas of developing countries.
Boosting the Adoption of Currently Available Vaccinations
Despite regularly administering infant immunizations (polio, measles, BCG and DPT) outbreaks of these diseases are on the rise in areas of the world plagued by extreme poverty. Thousands of lives must have been saved in these areas by early vaccination with conventional EPI vaccines such as measles. The best ways to access the groups that are held responsible for rapid growth in mortality rate of children in under developed countries with prim and proper health intervention, is the sole purpose of development aims in post 2015. The practical ways include having extensive knowledge of why people in these areas are unwilling to get vaccinated, keeping vaccines readily available, and collecting data through cell phone. However, operational research is still desperately needed to support these vulnerable groups of people [1]. Because getting vaccinated might have a wide range of negative effects, it is critical to assure vaccine safety during administration. It is also noteworthy to create a clear distinction between the true side effects of vaccines and just claims such as addressed association between MMR autism vaccines [2, 3].
Poliomyelitis Eradication
Despite the fact that eradicating poliomyelitis from its roots has proven to be more difficult than anticipated, WHA took the bold step of eliminating the disease in 2000. Stereotype 1 has been largely abolished, stereotype 2 has been completely destroyed, and stereotype 3 is still alive and well in Afghanistan, Pakistan and Nigeria, with the potential to spread to countries such as Syria, Somalia, and Chad [4]. According to the team working in the eradication mission, over 400 instances of polio were reported in 2013, and the system must overcome hurdles such as technical, financial, and social to completely eradicate the disease. The current polio vaccines contain all three stereotypes (1,2,3), which has been linked to an inconsistent immune response. This problem was handled by introducing and developing monovalent and bivalent stereotype 1 vaccines. The Bill and Melinda Gates Foundation and the Rotary Club have been funding extensively in the initiative due to its high expense, with a current campaign cost of $1 billion per year. Though the world community as sponsors has no intention of abandoning the effort, spending so little money on a single disease is untenable. Additionally, there has been resistance to vaccination in countries like Nigeria and Pakistan where it has resulted to the murder of health workers. If the polio eradication program encounters opposition, the results will be catastrophic, such as outbreaks in cases and a blockade of funds provided by the international community. The recent achievement in lowering virus cases in India creates favorable conditions for more investment, and if the virus is totally eradicated, the choice to phase out oral vaccine will be made. Countries on the verge of collapse have decided to employ more expensive polio vaccines for a period of time in order to eliminate all three types [5].
New Vaccines are being Introduced
Many routine vaccines, such as hepatitis B, rotavirus, hemophilus influenza stereotype b (Hib), pneumococcal and meningococcal polysaccharide/protein conjugate and human papillomavirus (HPV) have been introduced and used by industrialized countries since the start of the globally recognized EPI program in 1974. Despite the fact that the vaccines indicated have proven to be effective, their use in developing countries has been relatively slow. In Africa and Asia, the use of the hepatitis B vaccine in the normal EPI required nearly a score of years. Nonetheless, Hepatitis b is the sole cause of liver cancer in the aforementioned countries. Its usage delayed due to the vaccine’s prohibitive cost, as well as the difficulty in influencing health officials to approve child vaccination for targeted therapies. The use of Hepatitis B vaccine has increased to 80% as a result of the price reduction. Pneumonia and diarrhea are still blamed in impoverished nations for a number of fatal infections in children, including streptococcus pneumonia (the pneumococcus), Hib, and rotavirus [6]. It must, as a consequence, lower child mortality rates by producing effective pneumococcus and rotavirus vaccinations and including them in EPI programs [7, 8]. It’s still unclear whether pneumococcal immunizations have the same mind-blowing effect in impoverished areas as they did in developed nations. Introducing these vaccinations into routine immunization programs in developing countries has been fraught with difficulties. Due to the high cost of these vaccinations, they are more complicated to make than the first generation of pediatric vaccines. To address the main issue, the Global Alliance for Vaccines and Immunization (GAVI) (www. gavialliance.org (accessed 8 November 2013) was established in 2000 and has received significant funding from global contributors, totaling more than $1 billion annually, allowing the organization to fund the costs of these new immunizations for countries with a GDP of less than $1550 and to provide assistance for improvements in immunization conveyance programs. The Advanced Market Commitment, an alternative financing technique that has drawn in key assets from many significant donors, has also benefited the presentation of pneumococcal form vaccines.
GAVI established three specific vested parties, the pneumococcal and rotavirus Accelerated Development and Introduction Plans (ADIPs) and the Hib Initiative, to assist potential beneficiary countries in their enthusiasm for the value of providing these new vaccinations to their networks. These groups, which were based in higher education institutions but collaborated closely with Ministries of Health and Finance, non-legislative offices, and the pharmaceutical industry, aided in the production of local data on the burden of disease by providing training to all areas of the community on the significance of the contamination in question and, on occasion, attempted itemized epidemiological examinations and even antibody preliminaries [9]. They also facilitated negotiations with the pharmaceutical industry on plan pricing. Hib and pneumococcal form immunizations have been introduced much more quickly in countries with high youngster mortality as a result of the activities of these and other gatherings than hepatitis B immunization. Currently, 30 and 15 of the 56 GAVI-qualified countries have offered pneumococcal and rotavirus vaccines, respectively. Several GAVI-eligible countries are making significant economic progress and may soon surpass the GDP threshold that qualifies them for GAVI financing. Finding strategies to promote routine immunization in these countries when they become lower middle-income countries would be a challenge, using a layered evaluation framework and bulk purchasing are two options being considered. The inoculation plan at present utilized in most of emerging nations was grown, generally experimentally, when there was just a predetermined number of antibodies in the normal vaccination timetable and when it was viewed as those immunizations ought to be in every way given in the primary year of life when center participation is most noteworthy. Nonetheless, as an ever-increasing number of immunizations are added to the inoculation plan, this approach has must be inspected in view of the potential for immunological impedance between immunizations when given together and in light of the fact that the vaccination plan created for the first EPI antibody may not be the one that will give the best resistant reaction for some of the as of late evolved antibodies. In this manner, all things considered, more regular attendances at an immunization center will be required and that inoculation of kids should stretch out into the second year of life, as is as of now the case in many industrialized nations. Since inoculation reactions, as well as the study of disease transmission of numerous irresistible illnesses, can fluctuate fundamentally between populaces, vaccination plans should be intended to address nearby issues and a ‘one-size fits all’ approach is no longer appropriate. The only goal of vaccination programs in impoverished or underdeveloped countries is to avoid deadly diseases in newborn babies due to their extraordinary vulnerability at such a young age. Apart from that, the health benefits provided by vaccines are not confined to the first year of life; rather, they cover a wide range of treatments, such as curing cancer and meningococcal illness in adults through HPV vaccination of adult children [10, 11].
The Long-Term Future of Newly Developed Vaccine
Developmental Stages of the New Vaccines
The development of novel vaccines is difficult due to the morphological changes and life cycles of various species, such as the malarial parasite, which has antigenic diversifications that affect humans. In the literature, influenza and HIV viruses are examples of organisms with complicated structures. For infectious disease, various vaccine such as those for the corona and dengue viruses, are developed using a variety of known technologies. Using both conventional and newly designed vaccinations, the results are more beneficial for complete control of these infectious diseases [12]. Researchers are increasingly concerned about the limited results of HIV, tuberculosis, and malaria vaccines, making the development of new vaccines is a difficult challenging task for them in their quest to eradicate all of these infectious diseases [13, 14]. Reverse vaccinology, attenuated whole vaccines, and their comprehensive structural analyses are just a few of the unique methodologies being researched for the synthesis of new vaccines. These methods will be used to determine the antigenic and immunological responses that HIV and influenza virus strains elicit. The use of RNA instead of DNA to induce an immune response is being investigated for the development of novel nanostructure particles. However, antigens that provides a high level of protection for antibody responses to infectious diseases, such as malaria. These antibody responses will increase CD8T and CD4 cell responses. Moreover, adjuvants are playing an important role for enhancing immune response that are being tested. Adjuvants are also important for improving immune responses that are being studied [15, 16]. Vaccines are developed by storing them at room temperature in needle- free devices [17].
Financial Expenditure for the Development of New Vaccines
Some organisms that induce infectious diseases, including as typhoid Japanese B, tuberculosis, dengue, pneumococcal, HIV, influenza, and corona virus, are currently being studied in order to develop a cost-effective vaccine for all such infectious disease that will be a boon to humans. The United Kingdom, the United States, China, and other developed nations provide financial and technical support to their researchers, as well as large sums of money for the creation of new vaccines that will benefit humanity. Every country should have a standard national vaccination policy, and the number of vaccines should be expanded while maintaining their quality. The vaccine’s cost should be kept to a minimal, and its effectiveness will be closely evaluated. Because people in some developing nations are suspicious about vaccines, public awareness of vaccines should be prioritized. A large amount of money, time, and a standard technique were required to synthesize a new vaccine. As a result, in an industrialized market, the vaccination should be expensive, and the average person will not be able to afford it. Manufacturing companies should develop a vaccine that is both affordable and effective for a large number of people [18].
Vaccination’s Long-Term Future
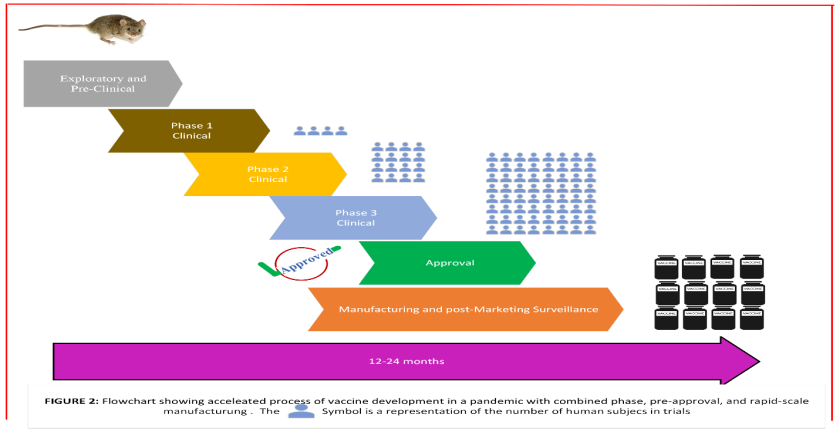
Even though it is impossible to determine how long some vaccines, such as malaria, tuberculosis, HIV, and corona, will work in a human’s life. Some vaccines are given for life, while others are given for a fixed period of time, depending on the vaccine’s efficacy. The eradication of these lethal diseases should be the final goal. Vaccination is clearly effective in the prevention and treatment of infectious diseases. Because of the development of vaccines, life on earth is feasible. Vaccines have the potential to save millions of lives each year. Whenever a pandemic (influenza, HIV, dengue fever, corona fever, etc.) broke out, it was quickly exterminated primarily to vaccinations. The discovery of numerous vaccines has improved the living conditions of underdeveloped countries, and the elimination of the terrible disease has been nipped in the bud. Infectious diseases such as tuberculosis, influenza, dengue fever, HIV, SARS, and Covid-19 threaten the lives of people in developing countries. People were also suffering with non-infectious diseases such as cancer, diabetes, and cardiovascular disease, in addition to infectious diseases, making life very difficult for the common man [19]. Is vaccination effective in the treatment of non-infectious diseases? Yes, vaccines are beneficial in the eradication of non-infectious diseases. Vaccination has recently been used to remove many types of cancer. Vaccines against the Epstein-Barr and Helicobacter pylori viruses are also available. This demonstrates that vaccines give people a new lease on life. Furthermore, several chronic diseases, such as hypertension and diabetes, are developing as lethal diseases that have proven difficult to control in the past with vaccines. However, immunizations have helped to control these life- threatening infections to some extent. Because the general public has limited access to primary healthcare facilities. However, vaccination is now a feasible reality for controlling hypertension and diabetes [20]. Furthermore, there is no vaccine available to protect against addictions like smoking. Recently, vaccines against addictions have been almost completed, requiring a large concentration of antibody to overcome the problem [21]. Another breakthrough in vaccine developmental milestone is the production of an Alzheimer’s disease vaccine that will be used to eradicate the disease [22]. In the near future, vaccines for pediatric illnesses will be produced, protecting children from potentially fatal infections. The vaccines for child poliovirus, tuberculosis, measles, and corona virus are all clear examples of modern worlds Figure 1 & 2.

Conclusion
Vaccines targeting non-infectious diseases will likely be developed in the next decade. New vaccines will be debated for their cost-effectiveness and affordability. These vaccines will be more expensive in developing countries, where they could be most helpful. An enhanced national immunization program is currently covered by international aid, primarily GAVI. There is no longer any GAVI support for many developing countries, including in sub-Saharan Africa. It may be necessary for lower middle-income countries to contribute more to their national vaccination programmes despite efforts to facilitate this transition.
References
-
Arora NK, Lal AA, Hombach JM, Santos JI, Bhutta ZA, et al. (2013) The need for targeted implementation research to improve coverage of basic vaccines and introduction of new vaccines. Vaccine 31(S2): 129-136.
-
Wakefield AJ, Murch SH, Anthony A, Linnell J, Casson DM, et al. (1998) Ileal-lymphoid-nodular hyperplasia, non- specific colitis, and pervasive developmental disorder in children. Lancet 351(9103): 637-641.
-
Glass RI, Parashar UD (2014) Rotavirus vaccines balancing intussusception risks and health benefits. N Engl J Med 370(66): 568-570.
-
(2013) Polio eradication: where are we now? Lancet 382(9902): 1381.
-
WHO (2013) Polio Eradication and Endgame Strategic Plan 2013–2018.
-
UNICEF (2015) Committing to child survival: a promise renewed.
-
Klugman KP, Cutts F, Adegbola RA, Black S, Madhi SA, et al. (2008) Meta-analysis of the efficacy of conjugate vaccines against invasive pneumococcal diseases. In: Siber GR, et al. (Eds.), Pneumococcal vaccines: the impact of conjugate vaccine. ASM Press, Washington DC, pp. 317-326.
-
Glass RI, Parashar U, Patel M, Gentsch J, Jiang B (2013) Rotavirus vaccines: Successes and challenges. J Infect 68 (Suppl 1): S9-S18.
-
Levine OS, Bloom DE, Cherian T, de Quadros C, Sow S, et al. (2011) The future of immunization policy, implementation, and financing. Lancet 378(9789): 439- 448.
-
Crosignani P, De Stefani A, Fara GM, Isidori AM, Lenzi A, et al. (2013) Towards the eradication of HPV infection through universal specific vaccination. BMC Public Health 13: 642.
-
Daugla D, Gami JP, Gamougam K, Naibei N, Mbainadji N, et al. (2013) Effect of a serogroup A meningococcal conjugate vaccine (PsA-TT) on serogroup A meningococcal meningitis and carriage in Chad: a community study [corrected]. Lancet 383(9911): 40-47.
-
Sabchareon A, Wallace D, Sirivichayakul C, Limkittikul K, Chanthavanich P, et al. (2012) Protective efficacy of the recombinant, live-attenuated, CYD tetravalent dengue vaccine in Thai schoolchildren: a randomized, controlled phase 2b trial. Lancet 380(9853): 1559-1567.
-
Rerks-Ngarm S, Pitisuttithum P, Nitayaphan S, Kaewkungwal J, Chiu J, et al. (2009) Vaccination with ALVAC and AIDSVAX to prevent HIV-1 infection in Thailand. N Engl J Med 361(23): 2209-2220.
-
Tameris MD, Hatherill M, Landry BS, Scriba TJ, Snowden MA, et al. (2013) Safety and efficacy of MVA85A, a new tuberculosis vaccine, in infants previously vaccinated with BCG: a randomized, placebo-controlled phase 2b trial. Lancet 381(9871): 1021-1028.
-
RTS S Clinical Trials Partnership, Agnandji ST, Lell B, Soulanoudjingar SS, Fernandes JF, et al. (2011) First results of phase 3 trial of RTS, S/ASO1 malaria vaccine in African children. N Engl J Med 365(20): 1863-1875.
-
RTS S Clinical Trials Partnership, Agnandji ST, Lell B, J Fernandes JF, Abossolo BP, Ondo Methogo BGN, et al. (2012) A phase 3 trial of RTS, S/AS01 malaria vaccine in infants. N Engl J Med 367(24): 2284-2295.
-
Edens C, Collins ML, Ayers J, Rota PA, Prausnitz MR (2013) Measles vaccination using a microneedle patch. Vaccine 31(34): 3403-3409.
-
Moxon R, Snape MD (2013) The price of prevention: what now for immunization against meningococcus B? Lancet 382(9890): 369-370.
-
Liu MA (2011) Cancer vaccines. Phil Trans R Soc B 366(1579): 2823-2826.
-
Bachmann MF, Jennings GT (2011) Therapeutic vaccines for chronic diseases: successes and technical challenges. Phil Trans R Soc B 366(1579): 2815-2822.
-
Maurer P, Bachmann MF (2007) Vaccination against nicotine: an emerging therapy for tobacco dependence. Expert Opin Investig Drugs 16(11): 1775-1783.
-
Winblad B, Andreasen N, Minthon L, Floesser A, Imbert G, et al. (2012) Safety, tolerability, and antibody response of active Ab immunotherapy with CAD106 in patients with Alzheimer’s disease: randomized, double-blind, placebo-controlled, first inhuman study. Lancet Neurol 11(7): 597-604.
- Effects of 5-HTP and Melatonin on the Sleep Cycle of Medical Students
- Adsorption of Bisphenol A on NH4OH- Modified Rice Husk and Sugar Cane Bagasse Biochar
- Comparative Assessment of the Reinforcement Efficiency of Palm Fruit Fibre and Coconut Fibre in High Density Polyethylene (HDPE) Matrix Composite
- Importance of Bio Compounds Naturally Present in Food with Functionality in Animal Metabolism
- Sub-Acute Study on the Cardiotoxic Effects of Monosodium Glutamate Ingestion in Albino Rat
- Weight Management and Its Natural Solutions: A Review