Acute Emphysematous Pyelonephritis in Adults
<p>Emphysematous pyelonephritis is an uncommon but life threatening condition, It is characterized by a gas producing acute severe necrotizing infection of renal parenchyma, perirenal and collecting system. Most of the patients have underlying uncontrolled diabetes mellitus. Escherichia Coli is the commonest organism. The computed tomography is gold standard imaging method for the diagnosis. Management strategies for this condition have evolved from invasive surgical interventions to conservative approach with antibiotics and image guided percutaneous drainage.</p>
Introduction
Emphysematous pyelonephritis (EPN) is a gas forming, severe necrotizing infection of the renal parenchyma and its surrounding tissues. Uncontrolled diabetes mellitus (DM) is the most common associated condition [1, 2]. EPN requires special attention because of associated high mortality [3]. Mortality has reduced significantly in the last two decades because of gradual shift in treatment from the primary surgical drainage to the percutaneous catheter drainage under radio-image guidance along with antibiotics [4].
To illustrate, we describe a patient who had uncontrolled DM, renal stone disease, EPN and acute kidney injury (AKI). He was successfully treated with antibiotics, percutaneous drainage and supportive treatment.
An Illustrating Case
A 41-year-old gentleman with poorly controlled type 2 DM was admitted with complaints of fever and left flank pain of 10 days duration. Nine months ago, the patient was diagnosed as DM while evaluating for lower extremity non-healing ulcers. He was not compliant to the prescribed medications and was taking alternative medicines. Past history was also significant for renal stone disease. The fever was high grade, documented up to 103°F, intermittent and was associated with chills and rigors. The flank pain was dull in character, radiating to back and associated with dysuria, however there was no history of decreased urine output. Past history was significant for renal stone disease. Laboratory investigations showed hemoglobin 78 g/l, total leukocyte count 2.57 x 103 per mm3 and platelet count of 4.93 x 103 per mm3. The renal functions were deranged (serum creatinine; 2.2 mg/dl) with hyperkalemia (serum potassium; 6.7 mg/dl) (Table 1). At admission, blood sugars were in range of 400-500 mg/dl, but ketones were undetected in blood. His glycated haemoglobin (HbA1c) was 17.1. The urine microscopic examination showed full field of pus cells and 8-10 red cells per high power field.
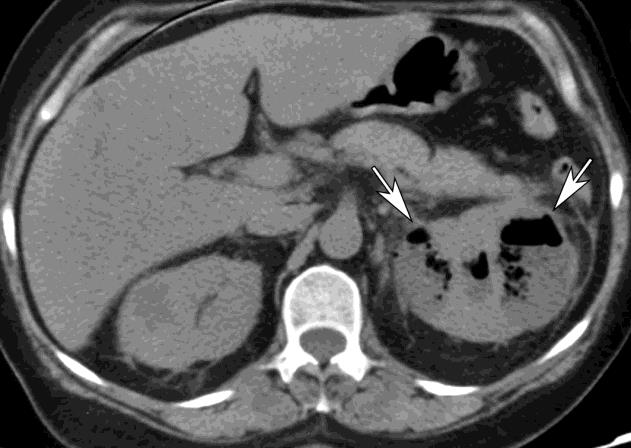
Ultrasound kidney ureter bladder (KUB) revealed bilateral enlarged kidneys with multiple air foci in left kidney suggesting EPN. The patient was started on intravenous piperacillin-tazobactum, fluid resuscitation, insulin infusion for hyperglycemia and anti-hyperkalemic measures. Subsequently, a computed tomography (CT) of KUB showed left side EPN class 3A with emphysematous ureteritis and bilateral nephrolithiasis (Figure 1). Two percutaneous catheters were placed in the right kidney under ultrasound guidance to drain the collected gas and pus. The culture of urine as well as of percutaneous drain grew Escherichia Coli, which was sensitive to piperacillin- tazobactum.
Following these measures, the patient became asymptomatic and the peripheral leucocyte counts, serum potassium, serum creatinine, plasma sugars and serum procalcitonin normalized (Table 1). The percutaneous drainage catheters were removed after two weeks and antibiotics were given for three weeks.
| Variable | Reference range* | On Admission | On Discharge | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Hemoglobin (g/dl) | 13.5–17.5 | 7.8 | 9.3 | ||||||||
| White cell count (per mm3) | 4000–11,000 | 25,000 | 9400 | ||||||||
| Differential count (%) | |||||||||||
| Polymorphonuclear cells | 40-70 | 88 | 73 | ||||||||
| Lymphocytes | 22-44 | 8 | 16 | ||||||||
| Monocytes | 04-11 | 4 | 10 | ||||||||
| Eosinophils | 0-8 | 0 | 1 | ||||||||
| Basophils | 0-3 | 0 | 0 | ||||||||
| Platelet count (per mm3) | 150,000–400,000 | 493,000 | 368,000 | ||||||||
| Sodium (mmol/liter) | 135–145 | 126 | 136 | ||||||||
| Potassium (mmol/liter) | 3.4–5.0 | 6.7 | 4.3 | ||||||||
| Chloride (mmol/liter) | 98–108 | 99 | 108 | ||||||||
| Blood urea (mg/dl) | 10-50 | 85 | 72 | ||||||||
| Creatinine (mg/dl) | 0.60–1.50 | 2.2 | 1.85 | ||||||||
| Bilirubin (mg/dl) | |||||||||||
| Total | 0.0–1.2 | 0.4 | 0.3 | ||||||||
| Direct | 0.0–1.0 | 0.8 | 0.1 | ||||||||
| Alanine aminotransferase (U/liter) | 7–35 | 15 | 10 | ||||||||
| Aspartate aminotransferase (U/liter) | 4–37 | 21 | 12 | ||||||||
| Alkaline phosphatase (U/liter) | 67–372 | 84 | 82 |
| Protein (g/dl) | |||
|---|---|---|---|
| Total | 6.0–8.3 | 5.6 | 8.2 |
| Albumin | 3.3–5.0 | 1.9 | 2.8 |
| Calcium (mg/dl) | 8.5–10.5 | 6.5 | 8.6 |
| Phosphorus (mg/dl) | 0.6–4.5 | 3.5 | 4 |
| Magnesium (mg/dl) | 1.7–2.4 | 1.8 | 1.76 |
| Prothrombin-time international normalized ratio | 0.9–1.1 | 1.1 | - |
| Partial-thromboplastin time (sec) | 22–35 | 26 | - |
| Serum procalcitonin (ng/ml) | 0.0-0.5 | 75.7 | 0.3 |
Table 2: Laboratory data (haematological and biochemical investigations) Table 1: Laboratory data (haematological and biochemical
Table 1: Laboratory data (haematological and biochemical investigations) Table 1: Laboratory data (haematological and biochemical investigations) *Reference values are affected by many variables, including the patient population and the laboratory methods used. The ranges used at Post Graduate Institute of Medical Research, Chandigarh (India) are for adults who are not pregnant and do not have medical conditions that could affect the results. They may therefore not be appropriate for all patients.
Etiopathogenesis
Uncontrolled DM is present in up to 80% cases of EPN [5, 6]. Urinary tract obstruction (UTO), neurogenic bladder, alcohol and drug addiction, and underlying immune-deficient conditions predispose most of the remaining cases [1, 7, 8]. Most cases are bacterial and Escherichia coli being the commonest organism (almost 67% cases) [4]. Klebsiella pneumonia, Proteus mirabilis, Pseudomonas, Enterococcus, coagulase negative Staphylococcus and rarely Candida species are isolated in most of the remaining patients [1, 9, 10].
The factors involved in the pathogenesis of EPN include hyperglycemia, presence of gas forming organisms, impaired vascular supply, reduced immunity and presence of UTO. The hypoxic environment of kidney medulla in diabetic nephropathy with associated micro- vascular disease may predispose these patients to tissue ischemia and necrosis, thus potentiating the growth of gas-forming microorganisms [11]. Fermentation of glucose and lactose leads to formation of gas (mainly carbon dioxide and hydrogen) by Gram negative organism [9].
Histo-pathological examination shows features of abscess, foci of micro- or macro- infarcts, vascular thrombosis, gas-filled spaces with areas of necrosis surrounded by acute and chronic inflammatory cells implying septic infarction [5, 12].
Clinical Features
Like other urinary tract infections, EPN is much more common in females. Patients usually present in 4th or 5th decade of life [4]. Clinical presentation is similar to other cases of severe pyelonephritis and usually consists of fever with or without rigors, flank pain, renal angle tenderness, vomiting or dysuria. In severe cases, multi- organ dysfunction and septic shock occurs early in the course.
Laboratory Diagnosis
Blood investigations commonly reveal leucocytosis, pyuria, bacteriuria, azotemia, metabolic acidosis, hyperglycemia or thrombocytopenia. Blood culture may be positive in almost half of the cases [12]. Ultrasound KUB is initial imaging of choice and is helpful to rule out urinary tract obstruction [13, 14]. A plain radiograph of KUB may show gas formation in renal parenchyma, however less sensitive and are rarely used now a day’s [15]. CT confirms the diagnosis and allows accurate delineation of the extent of the disease [12].
Management
Treatment depends on the illness severity and underlying host status. It includes adequate empirical antibiotics, source control and intensive supportive care. Empirical effective antibiotics should be started immediately to cover Gram negative bacilli according to local prevalence of the causative organisms and antibiotic susceptibility data. Beta-lactamase inhibitors, cephalosporins or aminoglycosides are usually preferred. Empirical monotherapy with quonolones or co- trimoxizole is not justified because of the increasing widespread resistance. Later, antibiotics should be modified according to the culture sensitivity of urine, blood or pus (drained under image guidance). Duration of antibiotics is usually 10 to 14 days, but should be modified according to improvement in clinical and laboratory parameters.
In accordance to the old dictum “pus anywhere in the body must be taken out”, open surgical drainage or emergency nephrectomy was the mainstay of the treatment in the past. As it was associated with high mortality, there has been a gradual shift in treatment of EPN from invasive to more conservative approaches with the availability of better imaging modalities, potent antibiotics and image-guided drainage [16]. Image guided aspiration or drainage of pus and gas has now become the standard part of the management. A systemic review showed that appropriate antibiotics and percutaneous drainage with or without elective nephrectomy has lower mortality than medical management or emergency nephrectomy alone [4]. Nephrectomy is indicated in the patients who do not respond to percutaneous drainage, Acute Pyelonephritis (Diagnosed on the basis of clinical features and urine analysis) antibiotics and have poor renal function on nuclear imaging, such as EC (ethylenedicystein) scan.
Supportive care consists of fluid, electrolyte and acid base management; glycemic control; and vasopressor support (in hypotension). Many patients require aggressive intravenous fluid to restore hydration and insulin infusion to achieve euglycemia. A proposed algorithm for the management of acute EPN in adults is given in Figure 2.
Prognostic factors: Based on the radiological findings on CT, two prognostic classification systems have been widely used to guide management.
Clinical suspicion of EPN (Host status: Diabetes, known or suspected urinary tract obstruction) (Complications at presentations: acute kidney injury, acute brain dysfunction, thrombocytopenia, multi-organ dysfunction, shock) Imaging (preferably CT) suggesting EPN Presence of poor prognostic factors requires intensive care (EPN class 3 or 4 on CT classification And/ or Acute kidney injury, acute brain dysfunction, thrombocytopenia, multi-organ failure or septic shock)
- Empirical antibiotics with coverage of Gram negative organisms
- Fluid, electrolyte and acid base management, blood sugar control
- Image guide percutaneous drainage or aspiration No clinical improvement or worsening or Poor renal function on nuclear imaging Consider urologist consultation for elective nephrectomy Figure 2: Proposed algorithm for acute emphysematous pyelonephritis in adults.
Wan et al. classified EPN in two types [5]. Type 1: Renal parenchymal necrosis with either presence of a streaky gas pattern or the absence of fluid collection. Type 2: Renal or perirenal fluid collection associated with a bubbly gas pattern or gas in the collecting system. Huang and Tseng provided a more detailed classification which found to have good correlation with staging and management [12]. Class 1: Gas in the collecting system only Class 2: Gas in the renal parenchyma only. No extension to the extrarenal space Class 3A: Extension of gas or abscess to the perinephric space (defined as the area between the fibrous renal capsule and the renal fascia) Class 3B: Extension of gas or abscess to the pararenal space Class 4: EPN bilateral kidneys or in a single functioning kidney Patients with EPN Class 1 and 2 have good outcome with medical management and percutaneous drainage. Class 3 and 4 with other poor prognostic factors like AKI, thrombocytopenia, acute brain dysfunction, multi-organ failure and septic shock have poor outcome [12, 17].
Conclusion
EPN is a life threatening condition. It usually occurs in patients with uncontrolled DM. E coli and Klebsiella are responsible in most of the cases. Prompt administration of empirical antibiotics and percutaneous drainage of the pus and the gas along with high quality supportive care is cornerstone of the management. Management is guided by clinical presentation, presence of organ failure and CT staging. Nephrectomy should not be delayed in patients who do not improve with percutaneous drainage.
References
-
Michaeli J, Mogle S, Perlberg S, Heiman S, Caine M (1984) Emphysematous pyelonephritis. J Urol 131(2): 203-208.
-
Pontin AR, Barnes RD, Joffe J, Kahn D (1995) Emphysematous pyelonephritis in diabetic patients. Br J Urol 75(1): 71-74.
-
Kaiser E, Fournier R (2005) Emphysematous pyelonephritis: diagnosis and treatment. Ann Urol (Paris) 39: 49.
-
Somani BK, Nabi G, Thorpe P, Hussey J, Cook J, et al. (2008) ABACUS Research Group. Is percutaneous drainage the new gold standard in the management of emphysematous pyelonephritis? Evidence from a systematic review. J Urol 179(5): 1844‑1849.
-
Wan YL, Lee TY, Bullard MJ, Tsai CC (1996) Acute gas- producing bacterial renal infection: correlation between imaging findings and clinical outcome. Radiology 198(2): 433-436.
-
Falagas ME, Alexiou VG, Giannopoulou KP, Siempos II (2007) Risk factors for mortality in patients with emphysematous pyelonephritis: A meta-analysis. J Urol 178(3): 880-885.
-
Godec CJ, Cass AS, Berkseth R (1980) Emphysematous pyelonephritis in a solitary kidney. J Urol 12: 119- 121.
-
Morehouse HT, Weiner SN, Hoffman JC (1984) Imaging in inflammatory disease of the kidney. Am J Roentgenol 143: 135-141.
-
Tang HJ, Li C, Yen MY, Chen YS, Wann SR, et al. (2001) Clinical characteristics of emphysematous pyelonephritis. J Microbiol Immunol Infect 34(2): 125-130.
-
Khaira A, Gupta A, Rana DS, Gupta A, Bhalla A, et al. (2009) Retrospective analysis of clinical profile, prognostic factors and outcomes of 19 patients of emphysematous pyelonephritis. Int Urol Nephrol 41(4): 959-966.
-
Tseng CC, Wu JJ, Wang MC, Hor LI, Ko YH, et al. (2005) Host and bacterial virulence factors predisposing to emphysematous pyelonephritis. Am J Kidney Dis 46(3): 432-439.
-
Huang JJ, Tseng CC (2000) Emphysematous pyelonephritis: clinical radiological classification, management, prognosis and pathogenesis. Arch Intern Med 160(6): 797-805.
-
Shokeir A, El-Azab M, Mohsen T, El-Diasty T (1997) Emphysematous pyelonephritis: A 15 year experience with 20 cases. Urology 49(3): 343-346.
-
Pagnoux C, Cazaala J, Me´jean A, Haas C (1997) Pye´lone´phrite emphyse´mateuse chez le diabe´tique. Rev Med Interne 18: 888-892.
-
McHugh T, Albanna S, Stewart N (1998) Bilateral emphysematous pyelonephritis. Am J Emerg Med 16(2): 166-169.
-
Ubee SS, McGlynn L, Fordham M (2011) Emphysematous pyelonephritis. BJU Int 107(9): 1474‑1478.
-
Bhat RA, Khan I, Khan I, Mir T, Palla N (2013) Emphysematous pyelonephritis: Outcome with conservative management. Indian J Nephrol 23(6): 444-447.
- The Muculent Bleb-Mucinous Cystic Neoplasm-Hepatobiliary Region
- Insulin Sensitizers as Anti-Aging Agents: Unveiling Synergies with Albumin, GLP-1RA, Klotho Protein, and Metformin in the Quest to Combat Aging
- Reprogramming of GLP-1 Response at Prediabetes for the Prevention of Type 2 Diabetes: The Role of Albumin and GLP-1 Receptor Agonists
- The Mingled Allies-Combined Hepatocellular Carcinoma and Cholangiocarcinoma
- Compilation and Embodiment-Leydig Cell Tumour Testis
- Glucolipotoxicity: A Novel Different Perspective on the Causes of Cancer