Tuberculous Pericarditis: A Review
Pericardial tuberculosis is a life threatening condition and mainly occurs in areas where tuberculosis is endemic, like in the parts of Africa and Asia. A definite microbiological or histopathological diagnosis may not be possible in most cases, therefore, the patients of endemic regions should receive a presumptive diagnosis of tuberculous pericarditis on the basis of clinical presentation, imaging procedures and/or evidence of tuberculosis elsewhere in the body.
Introduction
Tuberculosis (TB) is the commonest cause of pericardial disease in the regions where TB is endemic, and is associated with high mortality and long term disability even with antituberculosis treatment (ATT) [1, 2, 3, 4, 5, 6]. A definite diagnosis requires demonstration of tubercle bacilli in the pericardial fluid or on the histopathological section of the pericardium [6]. However, in conditions where a definitive diagnosis is difficult to make, radio-imaging or evidence of tuberculosis in any other organ establishes the diagnosis [6]. To illustrate, we describe a patient who presented with prolonged fever and was subsequently diagnosed as pericardial TB. He was successfully treated with ATT and adjuvant steroid therapy.
An illustrative case
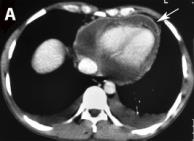
A 29-year-old male presented with history of fever for one month. Fever was low grade, maximum documented up to 102°F, associated with evening rise of temperature, chills, night sweats and involuntary weight loss. On admission, patient was hemodynamically stable. Cardiac auscultation found muffed heart sounds. Other systemic examination was normal. Laboratory investigation showed the peripheral leukocyte count 5.1x109/l and the erythrocyte sedimentation rate of 54 mm per hour. A chest radiograph revealed slightly enlarged cardiac silhouette and blunting of bilateral costo-phrenic angles. A 2D echocardiography showed moderate pericardial effusion. Subsequently, a contrast enhanced computed tomography of chest revealed pericardium wall enhancement with pericardial effusion and bilateral pleural effusion (Figure 1). Pleural fluid examination showed an exudative effusion with elevated adenosine deaminase (ADA) (52 U/L; reference <40), and no malignant cells. An HIV serology was negative. Urine analysis did not show any proteinuria. Ultrasound imaging of the abdomen was normal.
With a presumptive diagnosis of pericardial TB, patient was started on four drugs ATT along with prednisolone. At one month follow up, patient was asymptomatic and a repeat 2D echocardiography showed significant resolution of the pleuro-pericardial effusion.
Epidemiology
TB pericarditis is caused by Mycobacterium tuberculosis and is found in 1-2% of the cases of pulmonary tuberculosis [7]. Sub-Saharan Africa and the part of Asia carry largest number of TB pericarditis patients. In these endemic regions, TB is responsible for majority of clinically significant pericardial effusion (50- 70% in non-HIV infected cases and 90% in HIV-infected cases) [8, 9]. In Africa, the disease has a high association with HIV; whereas in Asia, it is usually seen in non-HIV, immunocompetent cases. In Europe and North America, TB pericarditis is rare and is usually considered as a disease of immigrant population from TB endemic areas [2, 10, 11].
It can occur at any age, and males are affected more common than females [1]. Case fatality rates are 3 times higher in HIV infected cases than in non-HIV cases [4].
Pathogenesis
Pericardial involvement results due either to direct extension from adjacent mediastinal lymph nodes or to hematogenous spread. TB pericarditis has 4 pathologic stages [5]:
a) Fibrinous exudation with polymorphonuclear leukocytosis, relatively abundant tubercle bacilli, and early granuloma formation with loose organization of macrophages and T cells; b) Serosanguinous effusion with a predominantly lymphocytic exudate; c) Absorptive stage - effusion absorption with organization of granulomatous caseation and pericardial thickening caused by fibrin, collagenosis, and ultimately, fibrosis; and d) Constrictive scarring - fibrosis or fibrocalcification of the visceral and parietal pericardium is causing diastolic filling defect and constrictive pericarditis.
HIV positive patients with low CD4 counts usually have less granulomatous inflammation, significant pericardial effusion and lower incidence of constrictive scarring stage as compared to non-HIV patients [12].
Pericardial Effusion
Development of pericardial effusion is usually insidious or subacute in TB. The clinical presentation is usually with chronic nonspecific systemic symptoms like fever, night sweats, fatigue, anorexia and weight loss. Chest pain, dry cough, dyspnea on exertion, orthopnea are common [7]. However, acute severe chest pain characteristic of acute pericarditis is uncommon. As extrapulmonary TB is among the commonest cause of fever of unknown origin in TB endemic regions, one should always keep possibility of pericardial TB in these patients. Heart failure like presentation is common in parts of sub-Saharan Africa. In Transkei region of South Africa, TB pericarditis associated heart failure is known as “Transkei heart” because of its high prevalence [13].
Clinical features of cardiac tamponade may ultimately appear with large effusion; and include hypotension, pulsus paradoxux, jugular venous distension (with a prominent x descent and a diminished y descent), and muffled or absent heart sounds.
Chronic Constrictive Pericarditis (CCP)
CCP results after resolution of an acute infection or resorption of a chronic pericardial effusion. Patients usually present with gradually progressive dyspnea, fatigue, weakness, ascites and peripheral edema [13]. Ascites is more prominent than peripheral edema and usually occurs earlier (ascites precox), a sequence opposite to that is often seen in congestive heart failure of other etiologies. Anasarca, generalized muscle wasting, or orthopnea occurs in advanced stages. Physical examination reveals jugular venous distension (with prominence of both x and y descent), soft heart sounds and a pericardial knock. Congestive hepatomegaly with or without jaundice is also common.
Effusive Constrictive Pericarditis
The mixed form of TB pericarditis, pericardial effusion accompanied by constrictive pericarditis is common in endemic regions. This clinical hemodynamic syndrome results due to constriction of the heart by the visceral pericardium with a tense pericardial effusion in a free pericardial space [14]. Patients with this condition remain symptomatic after the drainage of the pericardial fluid alone, because the constriction remains untreated.
Diagnosis
The diagnosis of pericardial TB is not always straight forward; and mainly depends on echocardiography, chest imaging (usually CT or MRI), pericardial fluid analysis and evidence of TB elsewhere in the body. An electrocardiogram (ECG) and a chest radiograph are abnormal in almost all cases of TB pericardial effusion. ECG usually shows nonspecific ST segment and T wave abnormalities. The PR segment deviation and the ST segment elevation characteristic of acute pericarditis is uncommon [15, 16]. Low voltage QRS complexes suggest a large pericardial effusion. Electrical alternans, a pathognomonic for cardiac tamponade, occurs very rarely.
On chest radiograph, pericardial effusion appears as an enlarged and rounded cardiac silhouette, and may produce a characteristic “money bag” or “water bottle” appearance of the heart. Echocardiography is the first line investigation for all suspected cases of pericardial disease [6]. A significant amount of pericardial effusion with fibrinous material of “porridge like” appearance suggests exudative effusion, but is not specific for TB [6].
Radio-imaging (CT or MRI) may enable diagnosis at an early stage by showing the nature and amount of effusion, the pericardial thickening (>3 mm) and other findings suggestive of TB [2, 17]. Accompanying active pulmonary parenchymal lesions occur in almost one third cases. The pleural effusion is seen in almost half of the cases [7, 10, 18]. The characteristic mediastinal or tracheobronchial lymphadenopathy i.e. >10 mm size, central necrosis, conglomerated, sparing of hilar lymph nodes favors the diagnosis of TB. Therefore, microscopy and culture of the sputum or the broncho-alveolar lavage fluid, pleural fluid analysis, trans-bronchial needle aspiration from mediastinal nodes may be very helpful in establishing the diagnosis.
A diagnostic pericardiocentesis under echocardiographic guidance is recommended, whenever possible. In 80% cases, tuberculous pericardial effusion is hemorrhagic. The effusion is typically a protein rich exudate with predominance of lymphocytes or monocytes and a raised ADA level [6, 11]. Pericardial ADA cutoff reference range of 30-60 IU/L has almost 90% sensitivity and 70% specificity [8, 9]. Pericardial lysozyme and interferon-γ levels have also shown diagnostic utility, however data are limited and are not widespread available due to technical problems [9, 19].
Demonstration of tubercle bacilli in the pericardial fluid by direct smear microscopy, culture or polymerase chain reaction (PCR) establishes a definite diagnosis. Microscopy with Ziehl-Neelson staining has a very low diagnostic yield. Culture of pericardial fluid using Lowenstein-Jensen or double strength Kirchner medium grows Mycobacterium tuberculosis in up to two third of cases; however results may not be available for weeks, which limits the clinical utility. Quantitative PCR testing for nucleic acids of M. tuberculosis (Xpert MTB/RIF) in pericardial fluid has lower sensitivity than culture; but can detect pericardial TB in less than 2 hours and simultaneously detects a gene responsible for resistance to rifampicin, rpoB [6, 11].
Diagnostic pericardial biopsy is rarely done for diagnosis of pericardial TB in endemic regions and is not required before starting empirical treatment. In non endemic areas, pericardial biopsy must be considered before considering empirical ATT. Presence of granulomatous inflammation with or without caseous necrosis or acid fast bacilli on histopathology confirms the diagnosis in up to two third of cases; But, it needs expertization in the procedure and in advanced cases, may show only fibrosis. Tuberculin skin test (Mantoux) is not helpful in the diagnosis of pericardial TB in adults [6].
For endemic areas, when pericardiocentesis or pericardial biopsy is not possible, the European Society of Cardiology 2015 guidelines proposed a diagnostic score of >6 to make the presumptive diagnosis of pericardial TB, based on the following criteria: fever (1), night sweats (1), weight loss (2), globulin level >40 g/L (3), and peripheral leukocyte count <10x109/L(3) [6]. In this condition, ATT should be started immediately [6].
Treatment
Treatment regimen of ATT for pericardial TB is generally the same as that for pulmonary TB (for both HIV infected and non-HIV cases). Initially, an intensive phase consisting of four drugs, isoniazid (5 mg/kg/day), rifampin (10 mg/kg/day), pyrazinamide (15-30 mg/kg/day), and ethambutol (15-25 mg/kg/day) is given for 2 months and is followed by a continuation phase of isoniazid and rifampin (same dosing) for 4 months [6].
Adjunctive corticosteroid therapy has long been used to decrease the pericardial inflammation which results in effusion and constriction. However, the benefit of steroid treatment in terms of mortality and constrictive pericarditis is controversial. In a study from South Africa, 143 patients with TB pericarditis and constrictive physiology were randomized to receive placebo or prednisolone for first 11 weeks of ATT [21]. Rapid clinical recovery and reduced requirement for pericardiectomy were noted in adjuvant steroid group. However, a recent large randomized trial (the IMPI study) involving 1400 patients showed that adjunctive prednisolone did not improve the combined all cause death outcomes and was associated with increased incidence of HIV associated malignancies [22]. But, the incidences of constrictive pericarditis and hospitalization were both significantly decreased. Of the patients enrolled in this trial, more than 70% of the enrollees lack a microbiological diagnosis, and two thirds were HIV infected and most of them were not on antiretroviral treatment. A supplemental analysis including HIV-negative patients showed a small mortality benefit.
In conclusion, adjunctive corticosteroids may be used in patients with tuberculous pericarditis without HIV infection. In HIV-infected patients, it should not be routinely administered [6]. The suggested regimen is prednisolone 60 mg daily for 4 weeks, followed by 30 mg daily for 4 weeks, 15 mg daily for 2 weeks, and 5 mg daily for 1 week [21].
Pericardiectomy is required in the setting of persistent constrictive pericarditis despite 1-2 months of ATT.
Chronic constrictive pericarditis requires extended pericardiectomy [6].
Conclusion
Pericardial TB is the commonest cause of significant pericardial effusion, cardiac tamponade, effusive- constrictive pericarditis, and CCP in sub-Saharan Africa and parts of Asia, and carries high mortality and morbidity. In these TB endemic areas, a definite diagnosis of TB pericarditis may not be established in most cases. ATT with or without adjuvant steroid therapy should be started promptly. Prolonged fever with pericardial effusion and thickened pericardium in a patient from TB endemic area is TB pericarditis until proven otherwise.
References
-
Mayosi BM, Wiysonge CS, Ntsekhe M, Volmink JA, Gumedze F, et al. (2006) Clinical characteristics and initial management of patients with tuberculous pericarditis in the HIV era: the Investigation of the Management of Pericarditis in Africa (IMPI Africa) registry. BMC Infect Dis 6: 2.
-
Cherian G (2004) Diagnosis of tuberculous aetiology in pericardial effusions. Postgrad Med J 80(943): 262- 266.
-
Mutyaba A, Balkaran S, Cloete R, du Plessis N, Badri M, et al. (2014) Constrictive pericarditis requiring pericardiectomy at Groote Schuur Hospital in Cape Town, South Africa: causes and peri-operative outcomes in the HIV era (1990–2012). J Thorac Cardiovasc Surg 148(6): 3058-3065.
-
Mayosi BM, Wiysonge CS, Ntsekhe M, Gumedze F, Volmink JA, et al. (2008) Mortality in patients treated for tuberculous pericarditis in sub-Saharan Africa. S Afr Med J 98(1): 36-40.
-
Mayosi BM, Burgess LJ, Doubell AF (2005) Tuberculous pericarditis. Circulation 112(23): 3608- 3616.
-
Adler Y, Charron P, Imazio M, Badano L, Barón- Esquivias G, et al. (2015) 2015 ESC guidelines for the diagnosis and management of pericardial diseases: the Task Force for the diagnosis and management of pericardial diseases of the European Society of Cardiology (ESC) Endorsed by: The European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J 36(42): 2921-2964.
-
Fowler NO (1991) Tuberculous pericarditis. JAMA 266(1): 99-103.
-
Koh KK, Kim EJ, Cho CH, Choi MJ, Cho SK, et al. (1994) Adenosine deaminase and carcinoembryonic antigen in pericardial effusion diagnosis, especially in suspected tuberculous pericarditis. Circulation 89(6): 2728-2735.
-
Burgess LJ, Reuter H, Carstens ME, Taljaard JJ, Doubell AF (2002) The use of adenosine deaminase and interferon-g as diagnostic tools for tuberculous pericarditis. Chest 122(3): 900-905.
-
Sagrista-Sauleda J, Permanyer-Miralda G, Soler-Soler J (1988) Tuberculous pericarditis: ten year experience with a prospective protocol for diagnosis and treatment. J Am Coll Cardiol 11(4): 724-728.
-
Chang SA (2017) Tuberculous and Infectious Pericarditis. Cardiol Clin 35(4): 615-622.
-
Reuter H, Burgess LJ, Schneider J, Van Vuuren W, Doubell AF (2005) The role of histopathology in establishing the aetiology of pericardial effusions in the presence of HIV. J Lab Clin Med 48(3): 295-302.
-
Strang JI (1984) Tuberculous pericarditis in Transkei. Clin Cardiol 7: 667-670.
-
Sagrista-Sauleda J, Angel J, Sanchez A, Permanyer- Miralda G, Soler-Soler J (2004) Effusive-constrictive pericarditis. N Engl J Med 350: 469-475.
-
Rooney JJ, Crocco JA, Lyons HA (1970) Tuberculous pericarditis. Ann Intern Med 72(1): 73-78.
-
Habashy AG, Mittal A, Ravichandran N, Cherian G (2004) The electrocardiogram in large pericardial effusion: the forgotten “P” wave and the influence of tamponade, size, etiology, and pericardial thickness on QRS voltage. Angiology 55(3): 303-307.
-
Goo JM, Im JG. (2002) CT of tuberculosis and nontuberculous mycobacterial infections. Radiol Clin North Am 40(1): 73-87.
-
Strang J, Nunn A, Johnson D, Casbard A, Gibson DG, et al. (2004) Management of tuberculous constrictive pericarditis and tuberculous pericardial effusion in Transkei: results at 10 years follow-up. QJM 97(8): 525-535.
-
Aggeli C, Pitsavos C, Brili S, Hasapis D, Frogoudaki A, et al. (2001) Relevance of adenosine deaminase and lysozyme measurements in the diagnosis of tuberculous pericarditis. Cardiology 94(2): 81-85.
-
Schepers GW (1962) Tuberculous pericarditis. Am J Cardiol 9(2): 248-276.
-
Strang J, Gibson D, Nunn A, Girling DJ, Nunn AJ, et al. (1987) Controlled trial of prednisolone as adjuvant in treatment of tuberculous constrictive pericarditis in Transkei. Lancet 2(8573): 1418-1422.
-
Mayosi BM, Ntsekhe M, Bosch J, Pandie S, Jung H, et al. (2014) Prednisolone and Mycobacterium indicus pranii in tuberculous pericarditis. N Engl J Med 371: 1121-1130.
- The Muculent Bleb-Mucinous Cystic Neoplasm-Hepatobiliary Region
- Insulin Sensitizers as Anti-Aging Agents: Unveiling Synergies with Albumin, GLP-1RA, Klotho Protein, and Metformin in the Quest to Combat Aging
- Reprogramming of GLP-1 Response at Prediabetes for the Prevention of Type 2 Diabetes: The Role of Albumin and GLP-1 Receptor Agonists
- The Mingled Allies-Combined Hepatocellular Carcinoma and Cholangiocarcinoma
- Compilation and Embodiment-Leydig Cell Tumour Testis
- Glucolipotoxicity: A Novel Different Perspective on the Causes of Cancer