The Effect of Antiphospholipid Antibodies on the Structure of the Placental Villi
Two placentas at term were obtained of two woman pregnancy with diagnostic of phospholipid syndrome who were treated by means of antithrombotic therapy using acetylsalicylic acid and heparin. Newborns were born alive. Normal placenta as control was taken. Of each placenta five small specimens were taken of the basal plate. Three slides by specimen were prepared for light microscopy and 45 histological slides in total were stained with H&E. Trophoblast suffered changes remarkable. This appears thinner, interrupted, in denudation, accumulations of syncytium are expelled toward intervillous space, fragments of villi are observed, villi with disorganized structure are seen affected by edema. Immature villi affected by these changes are dominant in these observations. Antiphospholipids, antibodies have produced persistent immaturity.
Introduction
Antiphospholipid syndrome (APS) is classified as the association of thrombotic events and/or obstetric morbidity in patients persistently positive for these antiphospholipid antibodies (aPL). It is the most frequently acquired risk for recurrent pregnancy loss, placental dysfunction, stillbirth, intrauterine death, preeclampsia, premature birth and fetal growth restriction [1]. In positive mouse models complicated with this syndrome the histopathology and expression of apoptosis in placenta, with induced thrombosis associated and fewer mitotic cells has been observed [2].
Pathological studies of human placenta have shown the proinflammatory capacity of aPL via the complement system and proinflammatory cytokines [3]. The effects of Investigation Paper aPL are most constant and severe during pregnancy. Placental insufficiency, thrombosis, infarcts, hemorrhage, endothelial damage, trophoblastic basal membrane increased vasculitis, microembolization, hypercoagulability and placental ischemia are of pathophysiologic significance in APS [4].
It is likely that disregulated placental coagulation and resultant vasculopathy are the cause of fetal loss [5] although APS has been increasingly diagnosed in patients without underlying autoimmune disease [6]. This syndrome also can be observed in woman with maternal hypertension [7]. New mechanisms are described by which aPL could cause placental thrombosis and infarction, acting directly on the surface anticoagulant expressed of throphoblast cells [8]. So it has been hypothesized that aPL bind to cells and induce procoagulant activity via phospholipid binding proteins [9].
Significant differences studied using statistic anova have been indicated between mature and immature placental villi, terminal villi, fibrinoid deposition, edema, fibrosis and syncytial knots when compared the placental villi affected by aPL with placenta control [10].
Death of the citotrophoblast, scarcity of these cells, fewer transformation of cytotrophoblast cells into syncytial cells and death of syncytium, expulsion of large fragments of this to the intervillous space, denutation of the syncytiotrophoblast; are frequent events observed when the placental villi is attacked by aPL [11].
It is possible that these antibodies attack the plasma membrane of the trophoblast, interrump it, and regions denudated of syncytium provoke a decreased interchange of gases and nutrients, which could disarrange the stromal region of the villi. The vessels of the stromal region suffer this effect and the thrombi so originated could to be contributing with the instability of the villi. Although antithrombotic therapy will be used we can to know if contribute or not with the stability of the villous tree.
In this work our objective is to describe the hystopathological changes observed on the placental villi complicated with APS.
Material and Methods
Two placentas at term were obtained of two woman pregnancy with diagnostic of APS which were treated in the Maracay Central Hospital by means of antithrombotic therapy using acetylsalicylic acid and heparin of molecular weight low according to protocol [12]. A placenta of normal pregnancy at term without any pathology was obtained as control. Consent informed was given to the two woman pregnancy and the approval of the ethical committee of our institution according to Helsinky declaration. The newborns were born alive. Of each placenta were taken five small specimens of the maternal surface selected at random from the region central parabasal in the vertical plane. Three slides by specimen were prepared for light microscopy and 45 histological slides in total were stained with H&E. Each slide could to have of 1-3 cuts of 3-5um for their observation.
Olivar Clemente CS. The Effect of Antiphospholipid Antibodies on the Structure of the Placental Villi. Cell Cellular Lif Sci J 2019, 4(1): 000135.
Results
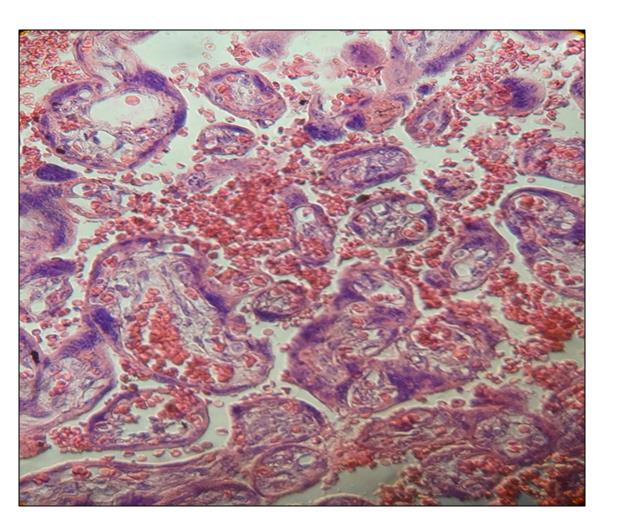
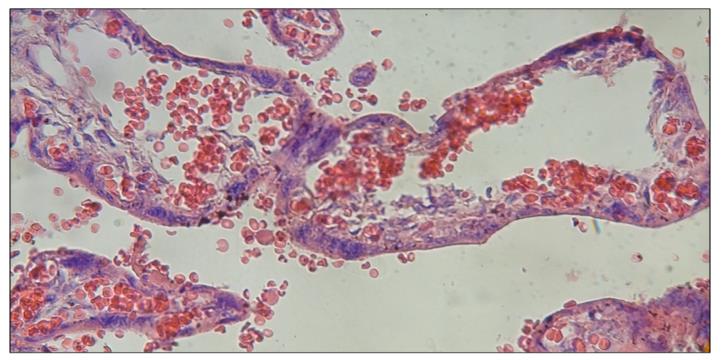
The throphoblast has suffered remarkable changes. This appears in occasions very thinner, interrumped and the villi is in denudation partially. Prominents accumulations of syncytium can be seen. Accumulate regions of syncytium are expelled toward intervillous space. The general wrappen of the placental villi is lost in numerous villi. Fragments of syncytium are observed in debris of placental villi in the intervillous space (Figure 1).
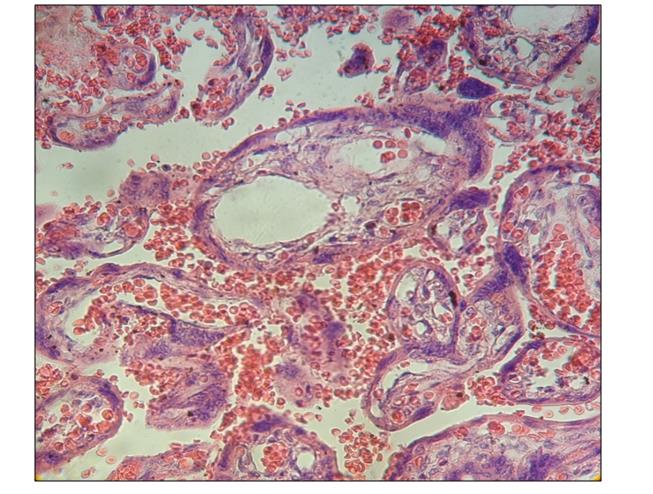
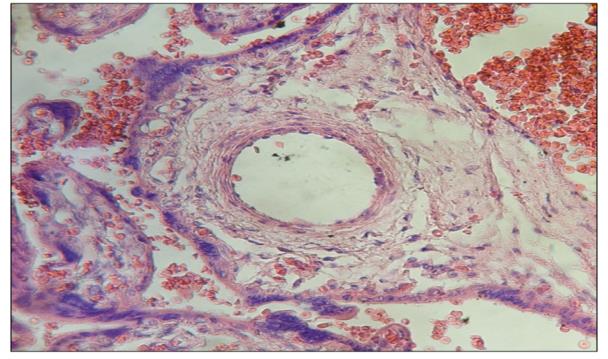
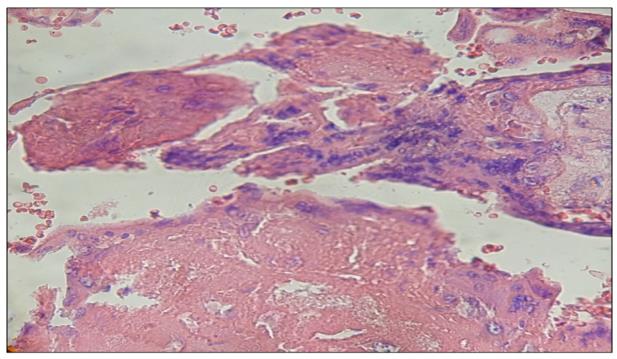
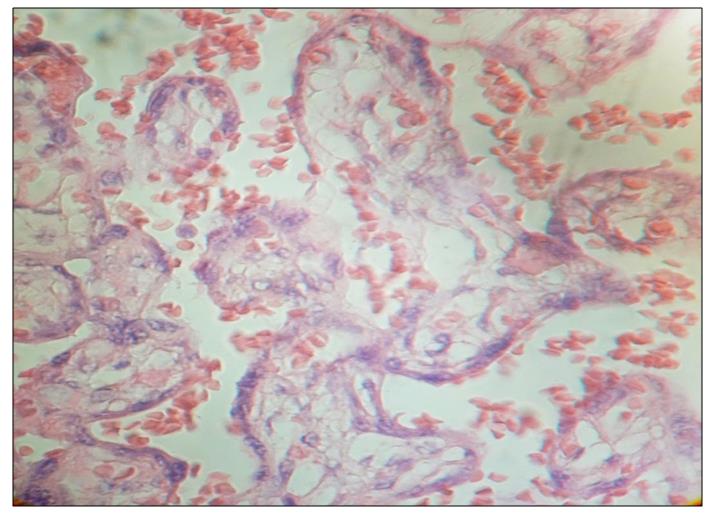
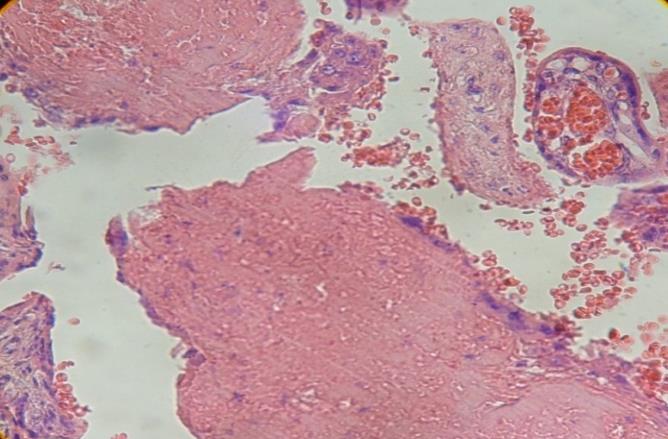
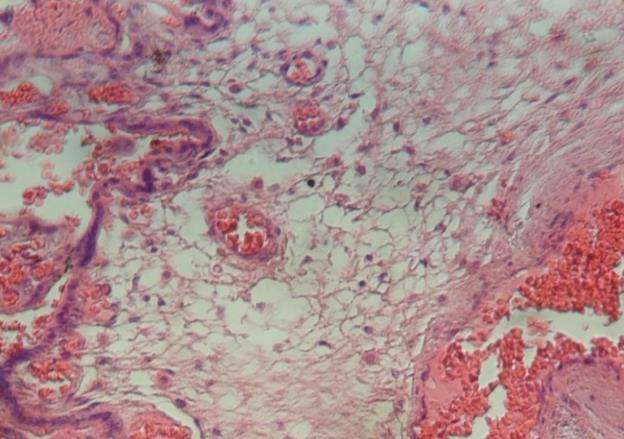
The vessels in the stromal region have the endothelium interrumped (Figure 2). In infarcted regions the vessels present degeneratives changes in the muscular layer provoked by edema (Figure 3). Regions of stem villi are seen with deposition of fibrinoid in their stroma (Figure 4).
Copyright© Olivar Clemente CS.
Degenerative changes are observed in these stem villi induced by edema (Figure 5). In numerous placental villi the stromal region is disorganized (Figure 6). Placental villi in total destructive form can be noted (Figure 7). Immature intermediate villi were seen with accented degenerative changes at level of stromal and trophoblastic regions (Figure 8).
Olivar Clemente CS. The Effect of Antiphospholipid Antibodies on the Structure of the Placental Villi. Cell Cellular Lif Sci J 2019, 4(1): 000135.
Copyright© Olivar Clemente CS.
Discussion
Interruptions of the syncytium provoked by aPL on the plasma membrane of it impede the normal interchange of gases and nutrients and the villi cannot maintain the normal fetal development causing fetal loss [13]. An uncovered villi absorb interstitial plasma is hydrated, swollen and exploit in fragments toward the intervillous space. These imagens are similar to the noted when the placenta is associated with zika virus and others viruses [14]. Degeneratives changes in the muscular layer and endothelium of vessels produce disorganization of the stromal region and the normal cytoarchitecture of the villi is disarranged originating villous death.
It is possible that the fibrinoid noted in stem villi is acting as an immunoprotective function or immunoabsorptive sponge since the fibrinoid can to express target antigens that bind circulating maternal antibodies and the resulting immune complexes contribute to the deposition of fibrinoid [15].
aPL have interrupted the syncytium [16] and the entrance of fluids to the stromal region disarrange it which present clear zones without tissue indicating edema. The interrupted endothelium is associated to this process. aPL have originated an generalized destructive effect in all the different types of villi which place the villous tree in no favorable conditions for the interchange of gases and nutrients.
It has been demonstrated by transmission electron microscopy that aPL bind to mitochondria in the syncytium and can cause mitochondrial swelling. aPL disrupt mitochondria increasing the extrusion of necrotic multinucleated syncytial aggregates [17] which trigger placental dysfunction.
Although antithrombotic therapy was used in the patients the placental lesions were maintained at term. This APS in early pregnancy produce fetal death in utero not explained after of 10 weeks of pregnancy. It has been mentioned that thrombosis frequently observed in the placentas of patients with APS is not an observation universal, nor is present in a sufficient degree to account to pregnancy loss suggesting that obstetric complications observed in APS may be due to induced trophoblast dysfunction [18]. The rupture of stromal channels in immature intermediate villi is contributing with large empty spaces demonstrated in the fig 2 of Lopez, et al. [10].
Olivar Clemente CS. The Effect of Antiphospholipid Antibodies on the Structure of the Placental Villi. Cell Cellular Lif Sci J 2019, 4(1): 000135.
The major findings in placentas from APS patients are ischemic hypoxic changes caused by thrombosis, decidual vasculopathy, thrombi, chronic villitis, fibrosis, hypovascular villi, decreased number of syncytiovascular membranes, increased number of syncytial knots, atherosis and decreased placental weight [19] which have provoked a permanent grade of immaturity in the placental villous tree.
In conclusion, an immature placental villous tree with throphoblast suffering changes remarkable has been found. Interrupted, denudated, swollen, and associated to debris of fragments of placental villi indicating that many villi have exploited in the intervillous space and the normal cytoarchitecture of the villi has been disarranged in the stromal region provoking their death and a permanent immaturity of the placental villous tree.
References
-
Schreiber K, Hunt BJ (2016) Pregnancy and antiphospholipid syndrome. Sem Tromb Hemost 42(7): 780-788.
-
Velayuthaprabhu S, Matsubayashi H, Sugi T, Nakamura M, Ohnishi Y, et al. (2013) Expression of apoptosis in placenta of experimental antiphospholipid syndrome mouse. Am J Reprod Immunol 69(5): 486-494.
-
Esteve Valverde E, Ferrer Olivares R, Alijotas Reig J (2016) Síndrome antifosfolipídico obstétrico. Rev Clin Esp 216: 135-145.
-
Gil I, Echavarria E, Molina J (1989) Actualizaciones. Anticuerpos antiphospholípids. Acta Med Colomb 14(5): 321-332.
-
Lockshin MD (1998) Pregnancy loss and antiphospholipid antibodies. Lupus 7(Suppl 2): S86- S89.
-
Dielmis J, Radoncic E, Ivanisevic M (2001) Antiphospholipid antibody syndrome and fetal outcome. Acta Med Croatica 55(3): 123-130.
-
Corosu R, Roma B, Cocola M, Marziali M (1998) Antiphospholipid síndrome in obstetrics. Minerva Ginecol 50(12): 9-13.
-
Vinatier D, Dufour P, Cosson M, Houpeau JL (2001) Antiphospholipid syndrome and recurrent Copyright© Olivar Clemente CS. miscarriages. Eur J Obstet Gynecol Reprod Biol 96(1): 37-50.
-
Atsumi T, Koike T (1998) Antiphospholipid syndrome. Nihon Rinsho 56(1): 215-223.
-
Lopez GA, Pante B, Pereira L, Paez A, Tovar O, et al. (2016) Lesiones estromales y trofoblasticas en vellosidades placentarias de gestantes con síndrome antiphospholipido en terapia antitrombotica. Electron J Biomed 2: 11-22.
-
Tong M, Viall CA, Chamley LW (2015) Antiphospholipid antibodies and the placenta: A systematic review of their in vitro effects and modulation by treatment. Human Reprod Update 21(1): 97-118.
-
Bates SM, Greer IA, Middeldorp S, Veenstra DL, Prabulus AM, et al. (2012) VTE, Thrombophilia, antithrombotic therapy, and pregnancy. Antithrombotic therapy and prevention of thrombosis. 9th (Edn.), American College of Chest Physicians. Evidence Based Clinical Practice Gidelines. Chest 141(2): e691S-e736S.
-
Benirschke KE, Kaufmann P (2000) Pathology of the human placenta. 4ed. New York: Springer Verlag. Olivar Clemente CS. The Effect of Antiphospholipid Antibodies on the Structure of the Placental Villi. Cell Cellular Lif Sci J 2019, 4(1): 000135.
-
Castejon OC, Pinto RMG (2018) Zika virus in placental villi at 28 weeks of pregnancy. J Emerg Rare Dis 1(1): 1-5.
-
Swinburne LM (1970) Leucocyte antigens and placental sponge. Lancet 296(7673): 592-594.
-
Parke AL (2006) Placental Pathology in antiphospholipid syndrome. In: Khamastha MA (Eds.), Hughes síndrome, Springer, London: pp 362- 374.
-
Pantham P, Viall CA, Chen Q, Kleffmann T, Print CG, et al. (2015) Antiphospholipids anti bodies bind syncytiothrophoblast mitochondria and alter the proteome of extruded syncytial nuclear aggregates. Placenta 36(12): 1463-1473.
-
Caruso A, De Carolis S, Di Simone N (1999) Antiphospholipid antibodies in obstetrics: new complexities and sites of action. Human Reprod Update 5(3): 267-276.
-
Gharavi AE, Pierangelli SS, Levy RA, Harris EN (2001) Mechanisms of pregnancy loss in antiphospholipid syndrome. Clin Obstet Gynecol 44(1): 11-19. Copyright© Olivar Clemente CS.
- The Muculent Bleb-Mucinous Cystic Neoplasm-Hepatobiliary Region
- Insulin Sensitizers as Anti-Aging Agents: Unveiling Synergies with Albumin, GLP-1RA, Klotho Protein, and Metformin in the Quest to Combat Aging
- Reprogramming of GLP-1 Response at Prediabetes for the Prevention of Type 2 Diabetes: The Role of Albumin and GLP-1 Receptor Agonists
- The Mingled Allies-Combined Hepatocellular Carcinoma and Cholangiocarcinoma
- Compilation and Embodiment-Leydig Cell Tumour Testis
- Glucolipotoxicity: A Novel Different Perspective on the Causes of Cancer